
Abstract
Thrombosis of synthetic grafts commonly used in cardiovascular surgery is a major complication. We examined whether pretreatment of the graft with heparin reduces the risk of early thrombosis. A circuit was assembled to compare two pairs of shunts simultaneously in the same animal. The study shunts were pretreated with heparin. After 2 hours of circulation, clot formation was evaluated by image analysis techniques. The pretreated grafts had fewer blood clots adhered to the surface by direct visual inspection. The image analysis showed 5 vs. 39 clots, 0.01% vs. 1.8% clotted area, and 62 vs. 5630 clot pixel area between the treated and non-treated grafts respectively, p < 0.05. Pretreatment of the synthetic graft with heparin prior to implantation reduces the risk of early clot formation. This simple practice might be helpful to prevent initial thrombosis of the graft and later occlusion.
Introduction
Synthetic grafts are being used commonly as replacements for blood vessels. These grafts may bypass an occluded peripheral vessel to supply blood flow, for instance, to an ischemic limb. In the setting of cyanotic congenital cardiac disease, synthetic grafts may supply blood to pulmonary circulation for oxygenation as an aortopulmonary shunt. The primary limiting factor in using these synthetic grafts is their inherent nature as an artificial surface to be prone to clotting due to activation of the coagulation system. Multiple techniques and modalities have been used to reduce the risk of thrombosis in the grafts, 1 the most traditional being systemic anticoagulation and platelet inhibitors. The risk of such treatments is high and may shift the pendulum to the other extreme of excessive bleeding. Other techniques have been focused on manipulation of the graft itself to reduce the risk of thrombosis. For instance sophisticated technology in material engineering has launched specific methods in fabricating less thrombogenic materials, improving surfaces and physical properties in these grafts. 1
One of the most common materials in use as a synthetic graft is polytetrafluoroethylene (PTFE). Its physical properties, including flexibility and biocompatibility by being an inert material, make it a favorable graft. Despite these properties, thrombosis of these grafts remains a major complication. Some groups have developed techniques to reduce the clot formation by specific treatments 2 or by surface manipulation of the grafts. For instance, the Gore Propaten Vascular Graft utilizes a covalent bonding technology to adhere heparin to the graft surface, known as Carmeda® BioActive Surface (CBAS). This technique supposedly allows blood flowing through the graft to resist clotting. Another group has showed carbon-lining decreases platelet accumulation and improves patency in small-diameter PTFE grafts in the acute phase. 3
No matter where the graft is implanted, it is subject to thrombosis. Clot formation on the graft surface either reduces the diameter, which impedes the blood flow, or generates thromboembolic events in the target organ. Such an event bears a high risk to the end organ ranging from ischemic damage or necrosis of the organ due to systemic hypoxemia.
Based on our prior lab experience, we observed that when the PTFE graft was exposed to heparin prior to implantation, the risk of graft thrombosis was reduced both in short and long term. We designed this study to evaluate whether simple treatment of a graft with heparin affects the clotting on the graft. We hypothesized that minimizing the early clot formation on the graft surface, which acts as a nidus for further clot propagation, will potentially reduce the risk for further clots.
Material and methods
The animal protocol was approved by Oregon Health and Science University's Institutional Animal Care and Use Committee. The animals received humane care, according to policies of the Position of the American Heart Association on research animal use (American Heart Association, 1985) and National Research Council: Guide for Care and Use of Laboratory Animals, 1996.
A circuit was assembled for simultaneous comparison of two groups of PTFE grafts in Yorkshire pigs 30–40 kg, Figure 1. This circuit simulated a systemic-pulmonary shunt and it was composed of three major components: an inflow cannula, comparison branches, and an outflow cannula. The inflow cannula (16 Fr.) was placed in the aorta and was secured with a purse string suture. It was then connected by a Y-connector to two major branches which further branched by secondary Y-connectors to secondary branches. The secondary branches were all connected to comparison grafts: 7 cm pieces of 5 mm diameter PTFE which connected proximally to the inflow branches and distally to outflow branches. In this setup, half the branches belonged to the control group and the second half to the study group. The outflow branches were all connected to the outflow cannula. The outflow cannula (20 Fr.) was placed in the pulmonary artery and also secured with a purse string suture. The study group of grafts was treated with heparin prior to placement in the circuit. This treatment included placement of the grafts in a container of heparin solution diluted with normal saline (100 units/ml) for 15 minutes. With installation of the circuit, blood flowed from the aorta through the inflow cannula to both the control and study branches simultaneously. The branches were all the same size and had the same properties with the only difference being exposure to heparin. Blood returned to the pig through the outflow cannula to the pulmonary artery.
Assembled circuit in the second animal. The inflow cannula is on the left side of the image branching to two arms dividing further to study and control graft limbs. All branches drain to the outflow cannula on the right side of the image, connected to the pulmonary artery. The side connectors used for the pressure monitoring lines (not shown here).
Overall 12 grafts were tested in this study; six grafts treated with heparin were compared to six non-treated grafts. In this standardized circuit the hemodynamic or thrombotic effects would be identical in all branches. The only variable was the exposure to heparin prior to exposure to blood flow. Basic hemodynamics, such as blood pressure and oxygen saturation, were monitored during the study. No vasopressor or inotropic agents were required. To ensure that no other physical factors, including the lay of the branches or kinks at the connection sites, affected the flow in the branches, pressures were monitored continuously from ports in the cannulae directly proximal and distal to the inflow and outflow branches. A gradient would be indicative of asymmetry or presence of mechanical problem in the system. The animal was treated with a dose of 30 units/kg of heparin prior to cannulation. After 120 minutes of blood flow and circulation in this set, the cannulae were clamped and disconnected from the animal. The PTFE grafts were cut from the branches and sliced open longitudinally to expose the inner surface. The grafts then were gently irrigated in normal saline solution to remove the blood, leaving only clots if any to their surface.
Digital images were taken in a standard technique of lighting and were coded for each graft for a blinded analysis. The images were analyzed by image analysis software. The density and area of the pixels was proportionate to the amount of the clot formed on the graft surface.
We then analyzed the obtained images using ImageJ software developed by NIH. Based on the data achieved from this clot quantification technique, we developed software for automatic quantification of clot density. After performing preprocessing, the software applies a binary filter to convert the image to binary format, where each pixel is either white or black, and then detects the clots by applying connected component labeling algorithm,4,5 where each blood clot is detected as a separate component. The number of members (pixels) in each detected component corresponds to the density of the clot. Quantification of the clots using this program provided objective and absolute parameters as total number of the clots (n), ratio of clot area to total graft surface (%), and density of the pixels as pixel area, indirectly measuring the total clot surface in pixels. All the parameters were averaged for all the grafts in each group and compared between the groups using the statistical model as follows.
Statistical analysis
All results are recorded as continuous variables. These variables are presented as mean ± standard deviation and were compared using a Students t-test in a univariate analysis of variance model. In all comparisons a p value less than 0.05 was considered significant.
Results
With initiation of the flow in the circuit, the heart rate increased about 10 beats per minute in each animal for a period of about 2 minutes, due to relative volume loss with blood filling the circuit. No other hemodynamic changes were observed throughout the study. No pressure difference was found between the study and the control branches, reflecting the similarity in the structure and lack of any distortion or asymmetry in the branches. The equal pressure and identical diameter also granted identical flows in both groups.
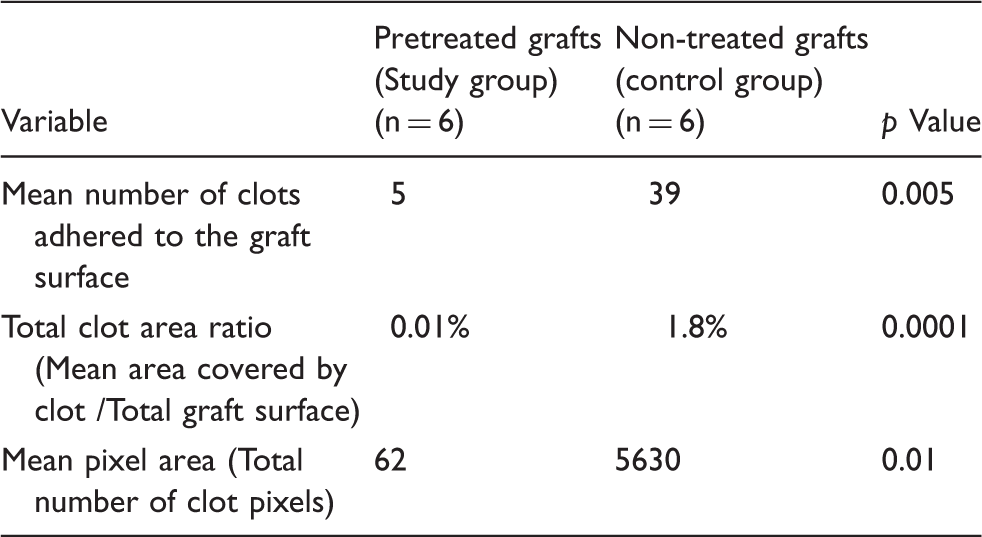
By direct visual inspection of the grafts, the pretreated grafts had fewer blood clots adhered to the surface, Figure 2. The image analysis showed five clots in average in the study group compared to 39 clots in the control group, p = 0.005. The total clot area as ratio to total graft surface was significantly smaller in the study group 0.01% vs. 1.8% clotted area, p = 0.0001, indicating less graft surface was covered with clots. The clot representing pixel area (number) was 62 pixels in the study group compared to 5630 pixels in the control group, p = 0.01. These results are presented in Table 1.
Sample grafts from the study group, pretreated with heparin (left) and the control group, not treated with heparin (right). The grafts are sliced open and held by an instrument to show the inside surface of the graft. Comparison between the heparin pretreated and non-treated grafts by image analysis technique. Compared to non-treated grafts, the pretreated grafts had fewer numbers of clot particles and less graft surface covered by clots.
Discussion
Synthetic vascular grafts have been widely used and have been an important tool in vascular and cardiovascular surgery for nearly 50 years. These studies aim to improve outcomes with synthetic grafts and decrease complications. The primary problem with small- and medium-sized grafts is the partial or complete occlusion of these grafts by thrombus.6,7 Other graft complications may include intimal hyperplasia at the anastomosis, serum leakage, mineralization, diffuse inflammation, infection, pseudoaneurysm formation, and changes in physicochemical characteristics of the graft. 8 Many factors may increase the risk of graft thrombosis. Some of these factors might be patient-related, such as hypercoagulable states, and some are graft- and procedure-related, such as manipulation of the graft creating damaged and uneven surfaces or stasis regions in kinks or folds.
It is known that most blood clots formed on the graft surface are generated in the initial exposure of the blood to the surface and activation of the clotting cascade. Any clot adhered to the graft surface becomes a nidus for additional activation of the clotting cascade and clot formation, and the process continues as a vicious cycle. It is possible that prevention of this initial process would reduce the clot formation on the graft in the long term.
Small-diameter vascular grafts, which are more prone to thrombosis than larger grafts, are used frequently as systemic-pulmonary shunts or as systemic bypass grafts. In many occasions these grafts are the only conduits for blood supply and their stenosis or occlusion by thrombus affords high risk of mortality. Small-diameter synthetic vascular grafts have shown significantly poorer performance when used in below-knee revascularization techniques. 9 Thrombosis of vascular shunts can, and often does, occur very early post-implantation. Li and colleagues 10 reported 1-year Kaplan-Meier event rates for shunt occlusion of 11% and 16% for closed and open (with cardiopulmonary bypass) shunts, respectively. In another review by Alkhulaifi and colleagues, 11 4 out of 75 (5%) neonatal patients receiving a systemic-to-pulmonary shunt had an acute thrombotic event within the first 24–48 hours post-operatively. All four required a reoperation, consisting of either a complete repair or a replacement of the shunt. 11
Some groups are focusing their studies on changes that a synthetic graft undergoes once implanted 8 or methods to improve endothelialization inside the graft12,6 to reduce risk of thrombosis.
In this study, our group examined application of a simple method to reduce risk of early thrombosis of these small-diameter grafts. The idea behind this study was based on our previous research experience, when we observed fewer thrombotic events in a PTFE graft when it was exposed to heparin before implantation. 13
The unique simultaneous comparison of the grafts in this study mimics a modified Blalock-Taussig shunt, often used in congenital cardiac surgery. The pretreatment of the vascular shunts with heparin by simply soaking them in heparin before implantation reduced the amount of clots formed on the graft surface. It is possible that some heparin molecules are adhered to the graft surface and they prevented the clot formation in the first exposure in the same mechanism of commercially available techniques of graft coating. However, the heparin bath just before the implantation might function as a “fresh coat” and prove more effective in this setting.
The idea of pre-treating vascular grafts is one that has been explored in past studies. In the late 90 s, Phaneuf and colleagues explored the effectiveness of both polyurethane and modified Dacron grafts coated with hirudin, a potent direct thrombin inhibitor. 6 Many studies followed using hirudin-based compounds or other direct thrombin inhibitors to coat Dacron grafts. Results were varied, but overall promising, which lead to further investigations for graft treatment. Heparin, an indirect thrombin inhibitor, has shown promising results in other studies. Not only does it indirectly inhibit thrombin production, it also inhibits the proliferation of vascular smooth muscle, 6 thereby minimizing the risk of intimal hyperplasia as well as thrombus. The luminal surface of PTFE grafts is hydrophobic, which inhibits endothelialization in situ and allows for increased thrombus formation. Heparin causes the graft to become more hydrophilic, thereby reducing the risk of thrombosis.14,15
A variety of different techniques have already been developed to coat bypass tubing with heparin, based on the molecule’s different binding properties.16,17 One such technique, heparin immobilization (CBAS), is based upon covalent end-point attachment of heparin to a biomaterial surface. 9 Using this same technology, CBAS-treated PFTE grafts have shown significant promise in reducing risk of thrombosis when used in canine carotid artery interposition grafts. 9 Heyligers and colleagues 18 used the PFTE grafts with heparin immobilization in a human ex-vivo study. In this study, the treated grafts were compared with control grafts. Using scanning electron microscopy, the standard PFTE grafts revealed deposition of platelets and fibrin, whereas there were no platelets or fibrin observed on the treated grafts. 18 It is feasible that pre-treating PFTE grafts with a heparin bath could produce similar results.
By using image analysis software, to detect and quantify the clots in this experimental model, we were able to demonstrate a significantly diminished amount of thrombus present in the grafts that were pre-treated with a heparin bath as compared to the control group. Quantification of clot by image analysis provided a unique method to objectively and directly evaluate the thrombus formation on the graft surface independent of the consequences and clinical results, which appear in later stages. This innovative technique has enabled us to assess very small clots in the early stages of graft use as the process commences before it progresses to generate large-size clots with hemodynamic and thromboembolic effects.
This study is limited by the short term of observation, effect of additional exposure to synthetic material in tubing, difference in thrombogenicity of swine versus human, and small number of observations. The study is standardized to a similar exposure of all the grafts to the same hemodynamic and thromobogenic environment with the only variable between the groups being heparin exposure. The observer bias was eliminated by numerical coding of the grafts and blinded analysis of the samples. Lastly, this experiment was designed to evaluate only the clot formation as an end result and is unable to explain the scientific mechanisms.
In conclusion, pretreatment of synthetic vascular grafts with heparin is a simple technique that potentially minimizes graft thrombosis. This easy maneuver could have a positive impact on the associated risks and complications of these vascular grafts. This technique is easily reproducible and applicable in any clinical setting; however, larger studies to prove the concept in human subjects and to understand the biological mechanisms of this phenomenon are warranted.
Footnotes
Acknowledgement
A similar version of this study has been presented as a poster presentation at CRT (Cardiovascular Research Technologies) meeting in February25, 2013, Washington, DC.
Funding
This research received no specific grant from any funding agency in the public, commercial, or non-profit sectors.
Conflict of interest
None declared.