
Abstract
The object of the study is to determine the long-term outcomes of surgical treatment of patients with popliteal artery entrapment syndrome at a single institute. We retrospectively reviewed 19 limbs of 16 consecutive patients who underwent surgery for popliteal artery entrapment syndrome at our hospital over the past 36 years. The popliteal artery was stenotic in 11 limbs, occlusive in 7 limbs, and compressed and deviated by the medial head of the gastrocnemius muscle but not damaged in 1 limb. Six limbs were treated with autologous saphenous vein bypass, 10 with bypass or venous patch graft concomitant with musculotendinous section, and 3 limbs underwent musculotendinous section alone. The 10-year cumulative patency of the 13 limbs treated with bypass was 100%, although two of them showed occlusion at 23 and 12 years after surgery. One patient who received a venous patch graft showed occlusion 15 years after surgery. Additionally, one asymptomatic patient with an apparently non-damaged popliteal artery who received preventive musculotendinous section alone showed stenosis of the artery 2 years after musculotendinous section. In conclusion, the bypass patency observed in this study was excellent in the long term. Careful examination of popliteal artery anatomy using imaging studies is essential for selecting the appropriate surgical procedure for popliteal artery entrapment syndrome.
Introduction
Popliteal artery entrapment syndrome (PAES) is a compression syndrome of the popliteal artery known to cause limb ischemia. The surgical strategy for PAES depends on the extent of arterial injury, the severity of the anatomical abnormality, and the clinical presentation. 1 Surgical release of the entrapment mechanism is one of the basic treatment policies, and vein graft bypass or venous patch is generally performed for a damaged or occluded popliteal artery.2–4 If the artery appears normal, only myotomy of the medial head of the gastrocnemius muscle and excising abnormal tendinous bands is reported all that is required.2–6
In previous studies, the patency of the bypass graft has been reported to be good, however, this may be, at least partly, owing to the fact that the patient populations included mainly young and physically active individuals.2,7 In addition, we have also reported good outcomes of 11 limbs in 10 patients with PAES who underwent surgical treatment and concluded that musculotendinous section (MTS) with or without bypass, may represent the optimal surgical method for these patients. 8 Based on this previous study, we have now added eight limbs in six patients, and in the present study, we retrospectively review the long-term (approximately 30 years) follow-up data of the patients. Although we revealed an excellent bypass patency in the long-term, we experienced one case whose popliteal artery showed stenosis only 2 years after MTS. Herein, we discuss the validity of our strategies for PAES, especially of MTS alone.
Patients and methods
We retrospectively reviewed 19 limbs in 16 consecutive patients who underwent surgery for PAES in our hospital over the past 36 years from 1976 to 2011. The follow-up periods ranged from 2 to 27 years (median: 15 years).
PAES was diagnosed using various imaging modalities such as computed tomography (CT), magnetic resonance imaging (MRI), duplex scanning, and intra-arterial digital subtraction angiography (IADSA). CT and MRI are useful for evaluating the various anatomic forms of PAES, namely: an anomalous course of the popliteal artery and development of the medial head of the gastrocnemius muscle, or existence of an accessory ligament. Doppler pulse evaluation and photoplethysmography test were useful for identifying fading of the pulse of the foot or toe during provocative maneuvers such as passive dorsiflexion or active plantar flexion of the foot, which is an unique sign of PAES. IADSA was sometimes performed for surgical planning of the bypass and venous patch grafting. Preoperative examination included measuring the ankle-brachial index (ABI) and the skin perfusion pressure to evaluate the risks of critical limb ischemia and tissue loss.
For PAES classifications, the most common classification system was used, which divides PAES into four types, as follows. Type 1: the medial head of the gastrocnemius muscle arises normally from the upper posterior medial condyle of the femur, and the popliteal artery is displaced in an exaggerated loop passing medially around and beneath the muscle origin; type 2: the medial head of the gastrocnemius muscle arises laterally, and the artery descends medially and beneath it, but its course is vertical and does not show exaggerated looping; type 3: The popliteal artery is compressed by an accessory slip of muscle from the medial head of the gastrocnemius, being entrapped beneath the accessory head; and type 4: the popliteal artery is entrapped by the deeper popliteus muscle or by a fibrous band in the same location. 5
The selections of the surgical procedures in our institute depends on the anatomy of the popliteal fossa and the features of the popliteal artery. Bypass was performed for popliteal artery occlusion of the long segment, whereas venous patch graft was performed for relatively short segments. These procedures were performed concomitant with MTS which depended on the type of PAES. MTS alone was performed for compressed and non-damaged popliteal arteries (Figure 1).
Flow chart of the popliteal artery entrapment syndrome (PAES) patients in our hospital.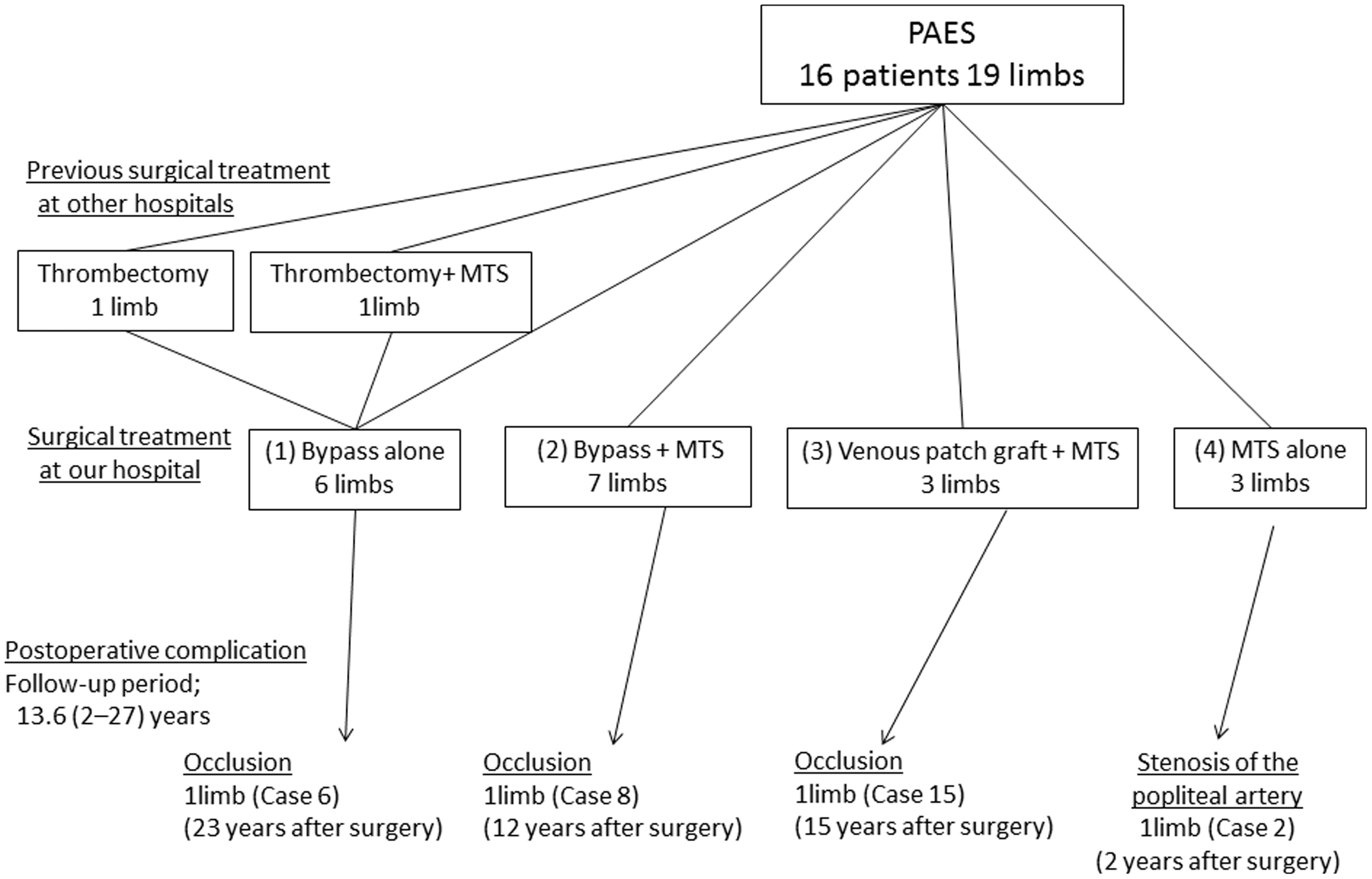
Postoperative surveillance with symptom assessments and ABI measurement was performed several times per year for the first 2 years. CT or MRI was performed annually during the follow-up period. Given the bypass insufficiency was suspected, additional examinations such as IADSA or duplex scan were performed for re-intervention planning.
All values are reported as mean ± standard deviation. Differences between groups were analyzed using Student's t-test. Kaplan–Meier survival curves were used to analyze the patency rate. A p value <0.01 was considered statistically significant.
Results
Patients’ characteristics, surgical treatment and clinical outcomes (n = 16).
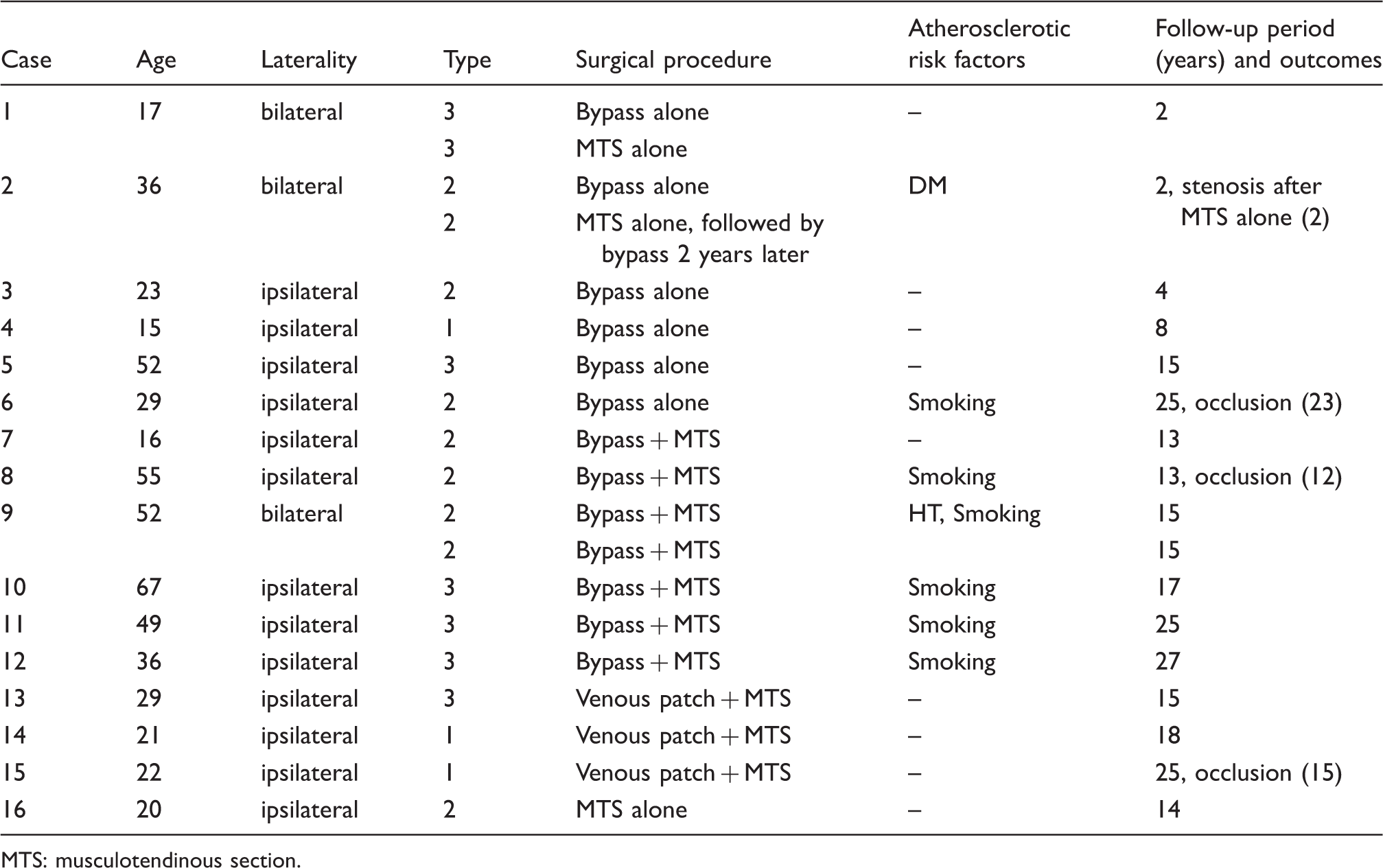
MTS: musculotendinous section.
Figure 1 shows a flow chart of the patients. Three PAES patients were introduced to our hospital and two of these had not been previously diagnosed before admission.
Two thrombectomies were performed in other hospitals, and neither of these was successful. In one case, the procedure itself was unsuccessful and the symptoms worsened. In the other case, re-stenosis of the popliteal artery and development of distal embolization occurred in the short term after thrombectomy and MTS.
The Kaplan-Meier curve of the graft patency revealed a good long-term result (Figure 2). The 10-year cumulative patency rate of 13 vein grafts was 100%. In the long-term follow-up, two bypasses were occluded 23 (case 6) and 12 years (case 8) post-surgery, and one venous patched graft was occluded 15 years after the surgery (case 15). Although intermittent claudication recurred in all these three patients after the occlusions, the symptoms did not worsen and we were able to observe them without any reintervention.
Kaplan-Meier curve of the graft patency.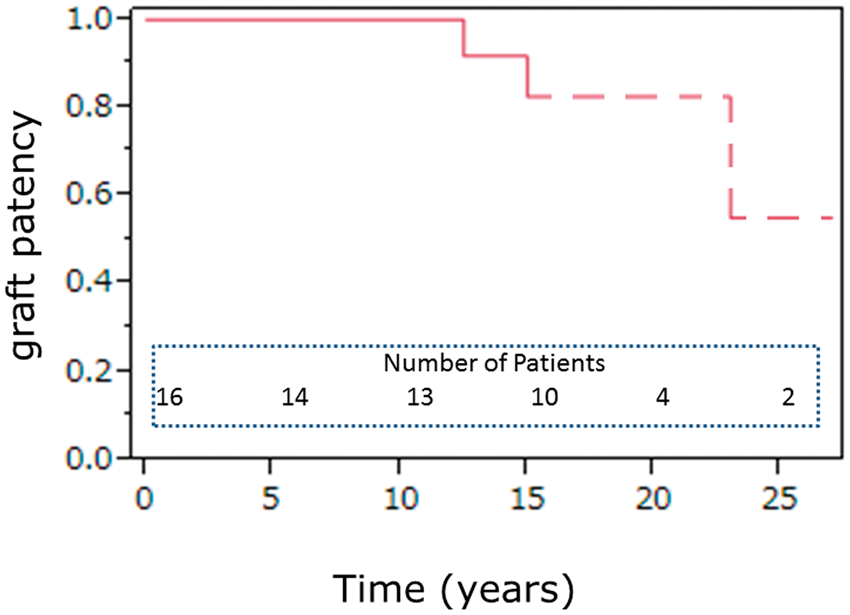
There was one case with stenosis of the popliteal artery in the short-term period after the surgical intervention (case 2). The patient was 36 years old and had been introduced to our hospital for progressive tissue necrosis of the left limb. CT revealed type 2 PAES in both legs. Accordingly, we performed bypass for the left limb, and MTS for the asymptomatic right limb, in which the popliteal artery was compressed and deviated by the gastrocnemius muscle head; however, the luminal surface appeared non-damaged upon CT (Figure 3a). After the MTS, the luminal surface of the popliteal artery was smooth and recovered to the normal shape and diameter (Figure 3b). Although the patient had been free from symptoms for 2 years after the surgery, he subsequently experienced the claudication of the right limb. Imaging modalities revealed stenosis of the right popliteal artery with thrombosis at the distal site from the previous compressed site (Figure 3c). Hence, we successfully performed bypass from the superficial femoral artery to the posterior tibial artery.
An asymptomatic popliteal artery entrapment syndrome case in whom musculotendinous section alone was performed preventively (case 2). (a) Preoperative image. Although the popliteal artery was compressed and deviated, the luminal surface was smooth and there was no intimal thickness. (b) Four days post-surgery. The deviation of the popliteal artery was corrected and the lumen was apparently normal. (c) Two years post-surgery. Computed tomography revealed stenosis of the right popliteal artery at the distal site of the previous compression.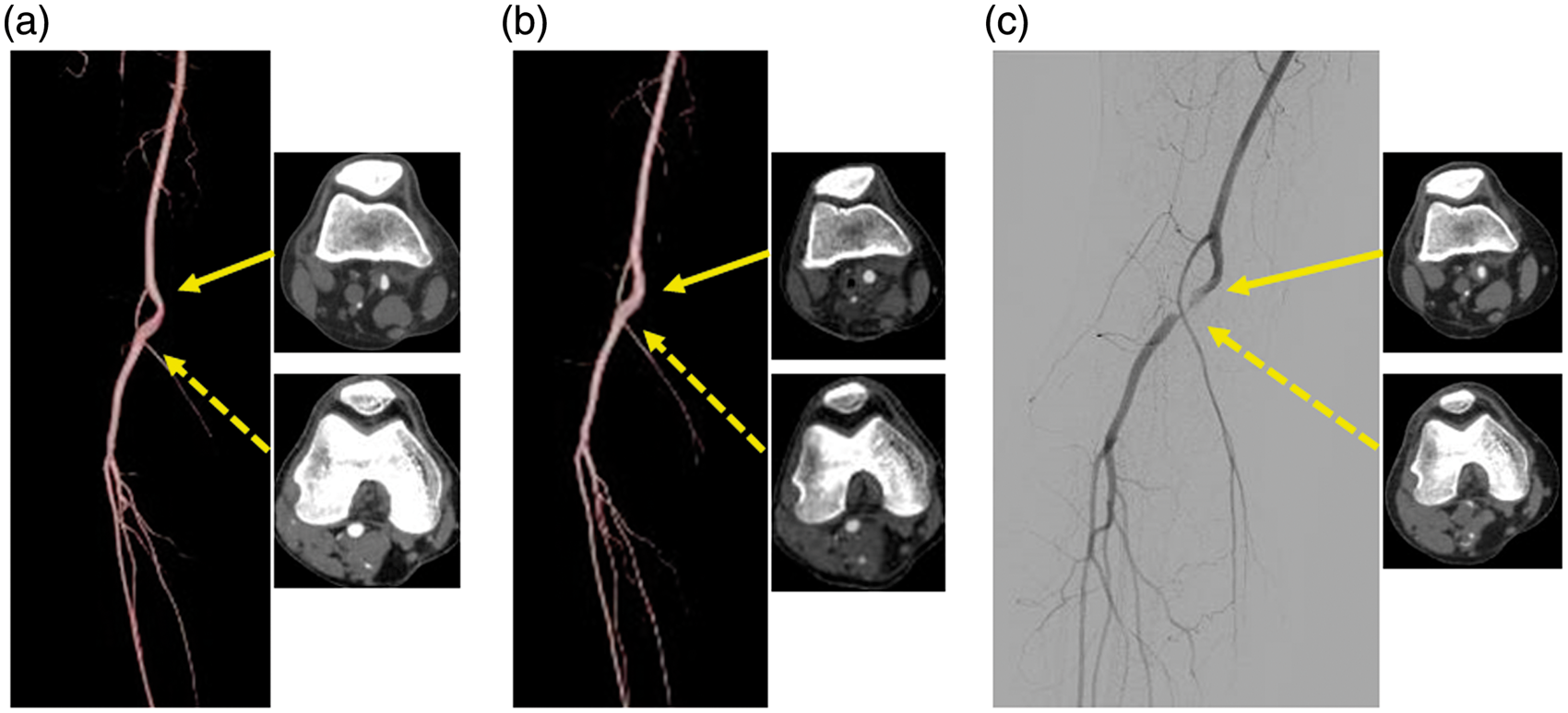
Discussion
There were three cases of bilateral PAES in our series, which is different from the rate in the report by Levien et al. 5 who showed that 40 out of 48 patients showed symptoms and entrapment bilaterally. Because of this discrepancy, we carefully examined and re-checked the imaging data in the present study. Although some cases only had old and low-quality CT images of thick slices taken 20 years ago, which might be insufficient for evaluating muscle or tendon displacement in detail, we could not find any other patients affected bilaterally. We were unable to reveal the cause of the discrepancy; however, it is nonetheless highly important to examine the contralateral site, given that we did find the ipsilateral PAES. Recent improvements of the imaging modalities have enabled us to get detailed anatomical information around the popliteal fossa, and we were able to identify the asymptomatic PAES in the contralateral site in case 2 in this way.
When the luminal surface of the popliteal artery is smooth and intimal thickness is not observed, MTS alone has been assumed to be all that is required.1–6,8 The process of arterial stenosis or occlusion of PAES is different from that of atherosclerosis. Progressive neovascularization, inflammatory cell infiltration, and vessel wall disruption leading to fibrosis and replacement of the wall with collagen tissue were observed histopathologically, and the process occurs from the adventitia, to media, and finally intima, in stages. 9 Therefore, MTS alone for cases with a “normal” luminal surface after the decompression should be a reasonable procedure. In terms of case 2 in the present study, who showed stenosis of the popliteal artery in the short-term period after the surgical intervention, we speculate that there might have been a microscopical intimal change that was undetec with the present imaging modalities. Nevertheless, MTS alone is a simple and less-invasive procedure which should be appropriate for the prevention of limb ischemia, and it should still be considered one of the surgical strategies of PAES. Accordingly, in a similar report by Gourgiotis et al., 4 67.3% of surgical procedures were MTS, and showed favorable operative outcomes. The main lessons learned from our present study are that careful examination and evaluation of the images by using various imaging modalities of the latest model are necessary, and that close follow-up should be performed when MTS alone is selected.
Functional PAES occurs in the apparent absence of anatomical anomalies, and the mechanism of entrapment is still unknown. One hypothesis is that hypertrophy and rapid movement of the anomalous muscle or band should cause arterial injury, consequently leading to degeneration, especially in athletes.7,10 Although there was no functional PAES in this study, the age of the athletes was significantly lower than the others, that indicated that such acquired factors might contribute to the emergence of PAES symptoms. PAES should be the first to be suspected when we see the lower limb ischemia in the athletes, even if we could not find anatomical abnormalities in the popliteal fossa.
We had maximally 27 years of follow-up periods in this study, and our data therefore included relatively old patients whose vessels may have shown degenerative changes. Nevertheless, the long-term outcomes were generally excellent and the 10-year graft patency was 100%. A possible reason for these favorable results is that all patients in the present study enjoyed exercising, hence, they likely had fewer atherosclerotic risk factors. In addition, most patients who were compelled to stop the sporting activities due to PAES were reported to resume normal activity.5,8 Therefore, we assume that surgical procedures for PAES should be safe and beneficial for young athletes. However, the procedure should be selected by careful examination of the images of the popliteal artery and its surrounding anatomies to retain the function as much as possible.
Ten years post-surgery, there were two patients (cases 6 and 8) whose bypass was occluded and one patient (case 15) whose popliteal artery was occluded in the present study. In these cases, ultrasonography examination during the follow-up periods did not show the significant stenosis, and all occlusions occurred suddenly. Although we suspect that smoking habits (for cases 6 and 8) and dehydration due to vigorous track and field exercise (for case 15) might be the contributory factors of the occlusions, the details are unknown.
Endovascular intervention for PAES patients is still controversial.11,12 It is mostly used supportively as thrombectomy of the occluded artery before the surgical correction of the PAES anatomy. However, the catheter intervention itself has the risk of shower atheromatous embolization, as seen in the flow chart which showed worsened symptoms after the interventions in other hospitals (Figure 1). Considering the excellent long-term outcomes of bypass and patients’ population with little surgical risks,7,8 we think that the benefit of endovascular procedure might be limited so far.
In conclusion, the bypass patency was excellent in the long term. However, one asymptomatic case demonstrated an adverse outcome in a relatively short period after preventive MTS. Therefore, careful examination of the images of the popliteal artery and its surrounding anatomies is necessary for selecting the appropriate surgical procedures.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.