
Abstract
Vascular injuries after a clavicle fracture are rare. The treatment remains, if possible, conservative. In case of life-threatening bleeding or limb ischemia, endovascular treatment is the treatment of choice. In this case report, we describe a patient who suffered a clavicle fracture five years before and now presented with acute invalidating claudication caused by an acute occlusion superimposed on a brachial artery stenosis. After unsuccessful thrombolytic therapy a surgical exploration of the brachial artery was performed.
Introduction
Complications of clavicle fractures are relatively uncommon and include acute complications such as pneumothorax and late complications with regard to fracture healing and nerve-related problems. Vascular injuries such as arterial and venous laceration, arterial dissection and occlusion are rare. 1
In this case report, we present a patient with an acute symptomatic occlusion of the subclavian and axillary/brachial artery five years after a clavicle fracture.
Case report
A 52-year-old man suffered a left mid-clavicle fracture five years ago after a bicycle accident complicated by a pseudo-arthrosis. After the accident, intermittent complaints of fatigue of his left arm were present.
He now presented himself with acute invalidating claudication and a numb feeling of his left arm. On examination, capillary refill of all fingers of the left hand was disturbed; sensory and motor functions were not impaired. No pulsations were palpable of either the radial and ulnar artery or the brachial artery.
Duplex ultrasonography of the left arm showed an occlusion from the mid-subclavian artery, just distal of the origin of the vertebral artery, to the brachial artery (Figure 1). Thrombolytic therapy with urokinase was started with 250,000 IE injected in bolus followed by 100,000 IE/h. After 24 h of thrombolytic therapy, a control angiography showed no improvement. The catheter was placed more distally into the brachial artery and urokinase therapy was continued.
Angiography showing occlusion of the subclavian artery.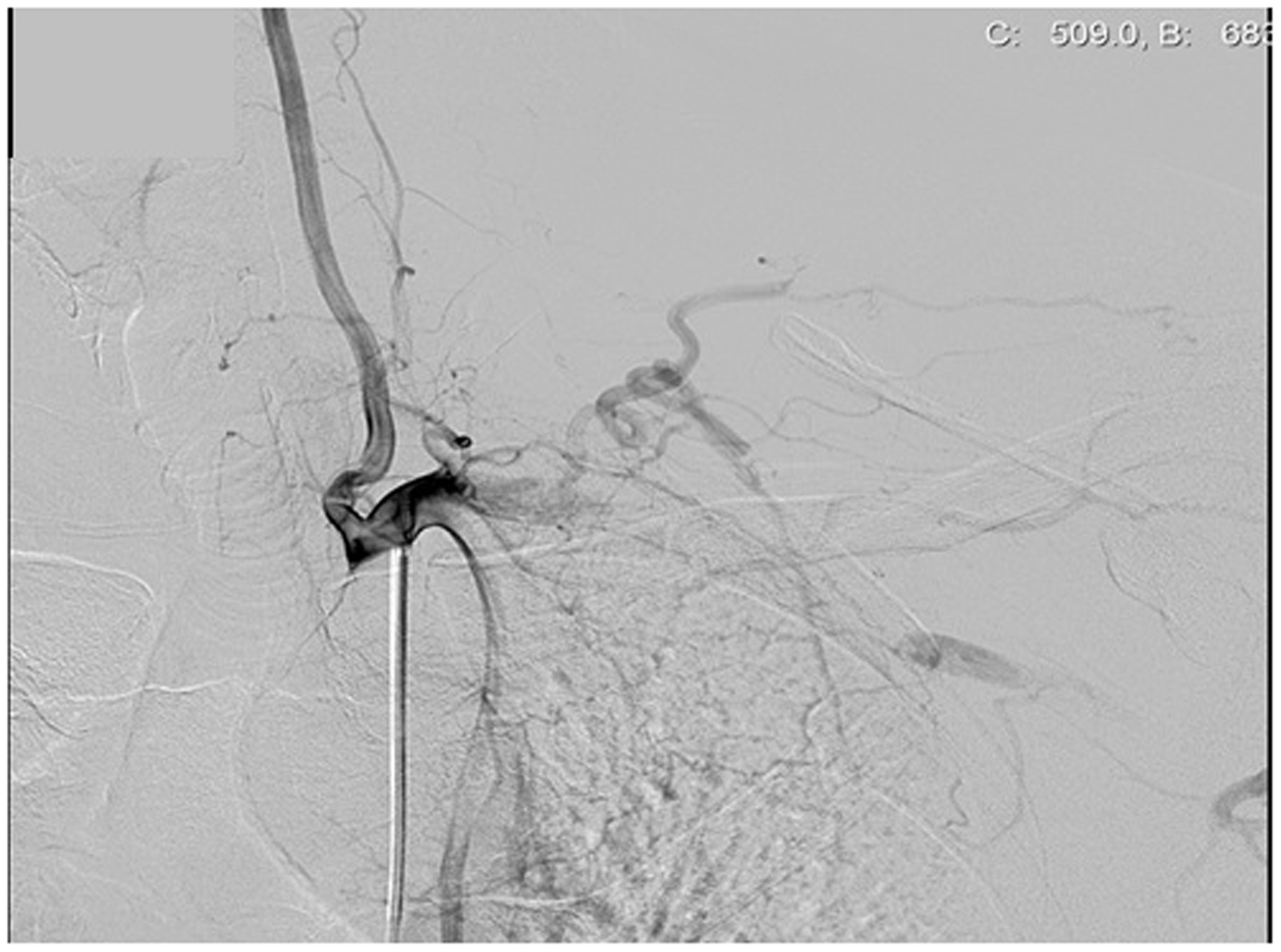
Control angiography after 48 and 72 h still showed a thrombus on a suspected stenosis in the brachial artery, and thrombolytic therapy was stopped (Figure 2). A CTA of the neck and thorax showed a dissection of the mid-subclavian artery and a stenosis of the brachial artery. No external compression by a bony, muscular or ligamentary structure on the artery was present. The next day, a surgical exploration of the brachial artery was performed after the stenosis was marked with duplex ultrasound. An organized thrombus was present on an intimal flap of 2 cm length in the proximal part of the brachial artery. The thrombus and intimal flap were removed and the brachial artery was reconstructed with a venous patch. The patient was heparinized and sintrom was started. The patient’s recovery was uneventful. Three weeks after the operation, the patient was discharged. One month later, the patient was seen in the outpatient department without any complaints. After six months, a duplex ultrasonography was made which showed a normal blood flow without signs of stenosis or occlusion.
Angiography showing a thrombus on a suspected stenosis in the brachial artery.
Discussion
Treatment for acute injury of the subclavian artery ideally remains conservative.
The presence of a large hematoma, a bony fracture, and the close relationship to important surrounding tissues has the potential risk of gross blood loss and injuries to the subclavian vein or the brachial plexus. If an intervention is needed in case of a gross bleeding or limb ischemia, endovascular repair is the treatment of choice. 2
In this case report, we described a patient who had an acute chronic ischemia of his left arm, resulting from a chest trauma five years before. In this specific case, we chose to start first with thrombolytic therapy to restore the vascularization of the left arm. Because of persistent thrombus we decided to perform a surgical exploration of the brachial artery, rather than endovascular treatment with stent placement. The reason for this was that the thrombus was near a large collateral and easily accessed by surgery. The dissection of the subclavian artery was not treated because it was five years old and already organized.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.