
Abstract
True arterial aneurysms of the upper extremity are rare. The case described is that of a 48-year-old man presenting with median neuropathy and distal vascular compromise 4 years after ligation of a brachiocephalic arteriovenous fistula. We describe our approach and present a review of the relevant literature.
Introduction
Arterial aneurysms of the upper extremity are rare and are most commonly false aneurysms resulting from blunt trauma, iatrogenic complications, or infection. 1 True aneurysms are even less common and may result from repetitive trauma or atherosclerosis. Brachial artery aneurysms (BAAs) have also been described in the setting of vasculitis and after ligation of an arteriovenous fistula (AVF).2–15 Our case is unique as it presented with median neuropathy and distal vascular compromise 4 years after ligation of a brachiocephalic AVF. We describe our approach and present a review of the relevant literature.
Case report
Our patient is a 48-year-old man with a history of end-stage renal disease on hemodialysis via a left brachiocephalic AVF, which was ligated in 2009 after his cadaveric renal transplant. Four years later, he presented complaining of 2 days of left hand numbness and pain. He denied a history of trauma, atrial fibrillation, or prior clotting disorders. His left hand was cool but pink. Brachial and ulnar pulses were palpable, and a triphasic Doppler signal was present in both palmer arch and digital arteries. Thrombosis of the previously ligated fistula was noted. The left hand had significantly diminished strength relative to the contralateral side, and sensation was blunted in the distribution of the median nerve.
A left upper extremity arterial duplex demonstrated aneurysmal dilatation of the brachial artery measuring approximately 1.9 cm with mural thrombus. Magnetic resonance angiography (MRA) demonstrated a hypertrophied brachial artery with focal aneurysmal dilatation measuring approximately 2.2 cm in diameter and 6 cm in length. The radial artery was found to have multifocal non-occlusive filling defects consistent with thrombus throughout its course, which was presumed to be embolic in nature. The ulnar artery filled briskly and constituted the only runoff to the hand. The deep palmar arch was patent, as were digital arteries.
The patient was started on intravenous heparin and his pain improved; however, he continued to have paresthesias of his left palm and fingertips, weakness, and poikilothermia suggestive of nerve compression. Given the urgent nature of the patient’s presentation, nerve conduction studies were not obtained prior to surgical intervention. Intra-operatively, the median nerve was found to be thickly encased by the aneurysm (Figure 1(a)). The nerve was dissected proximally and then freed distally along the 7 cm course of the aneurysm (Figure 1(b)). The brachial artery was dissected from the level of the junction with the axillary artery to the level of the trifurcation of the artery into the ulnar, radial, and interosseous arteries. The aneurysm was excised, and a 10-cm segment of the previously matured cephalic vein was harvested for use as an interposition graft. Attempts were made to remove the thrombus from the distally occluded radial artery; however, these were unsuccessful, and the vessel was ligated to prevent any propagation of clot into the anastamosis. He tolerated the procedure well and was discharged on postoperative day 2 in stable condition with significant improvement in his symptoms.
(a) Brachial artery aneurysm in situ, encasing the median nerve (arrow); (b) median nerve dissected free from the aneurysm sac (arrow).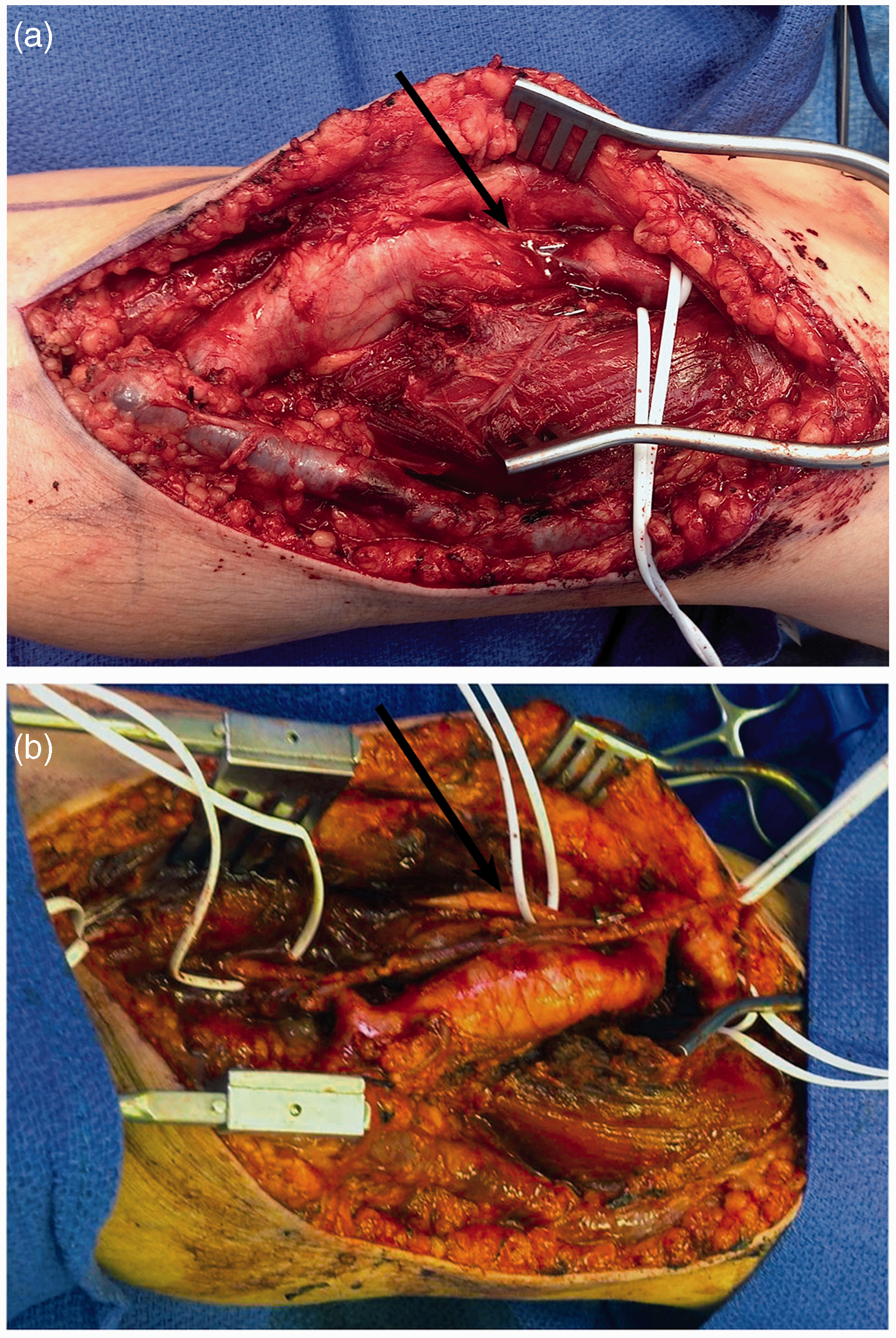
Histopathologic examination of the resected aneurysm revealed calcified atherosclerotic plaque with recent organizing and recanalizing thrombus (Figure 2). At 3 months, the patient had returned to work and continued to endorse complete resolution of his symptoms.
Organizing thrombus with multiple foci of recanalization, consisting of small vessels within the thrombus (100×).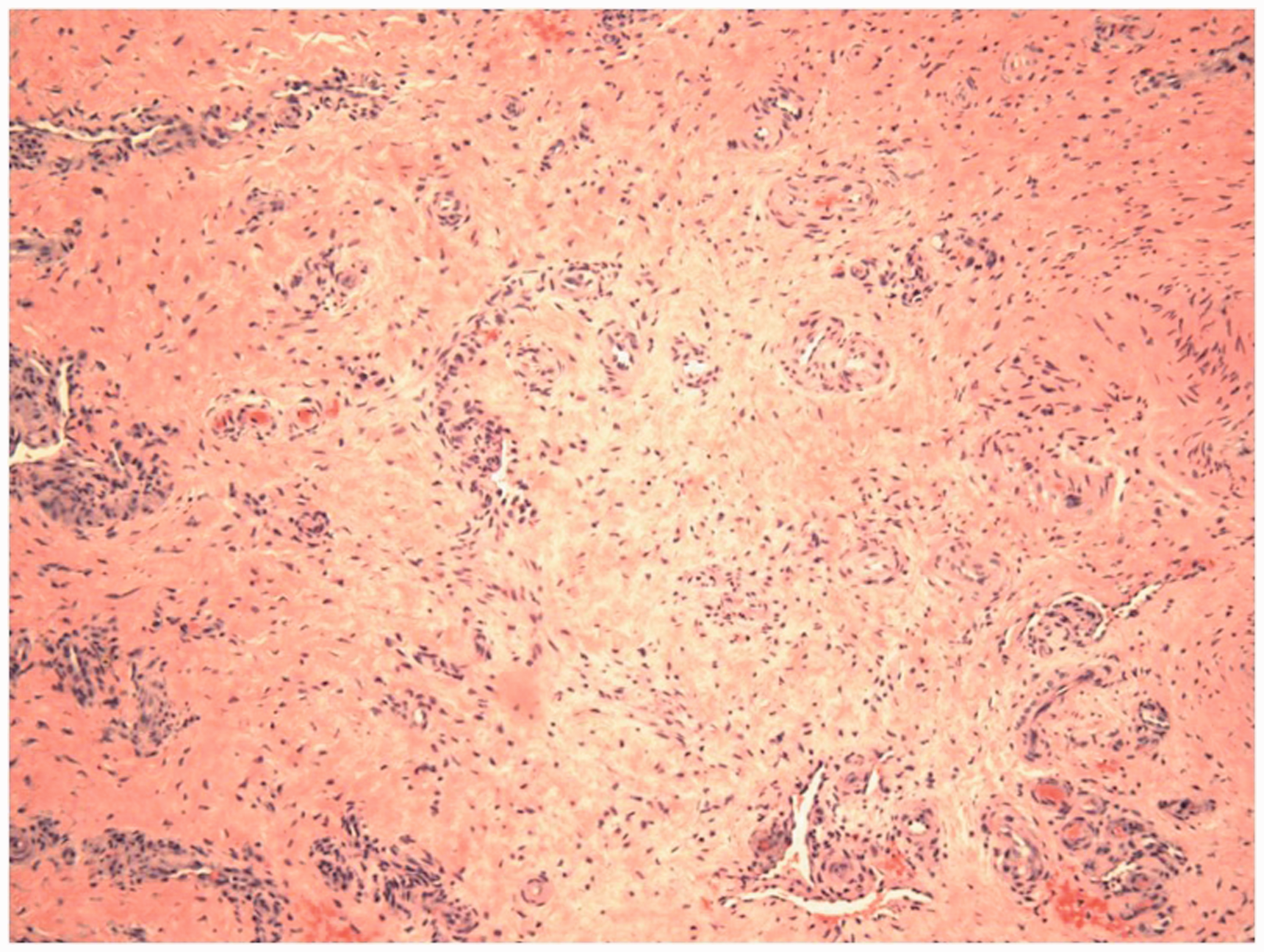
Discussion
Presenting symptoms associated with brachial artery aneurysms development after ligation of arteriovenous fistulae.

Reported cases of true brachial arterial aneurysms developing after ligation of arteriovenous fistulae.
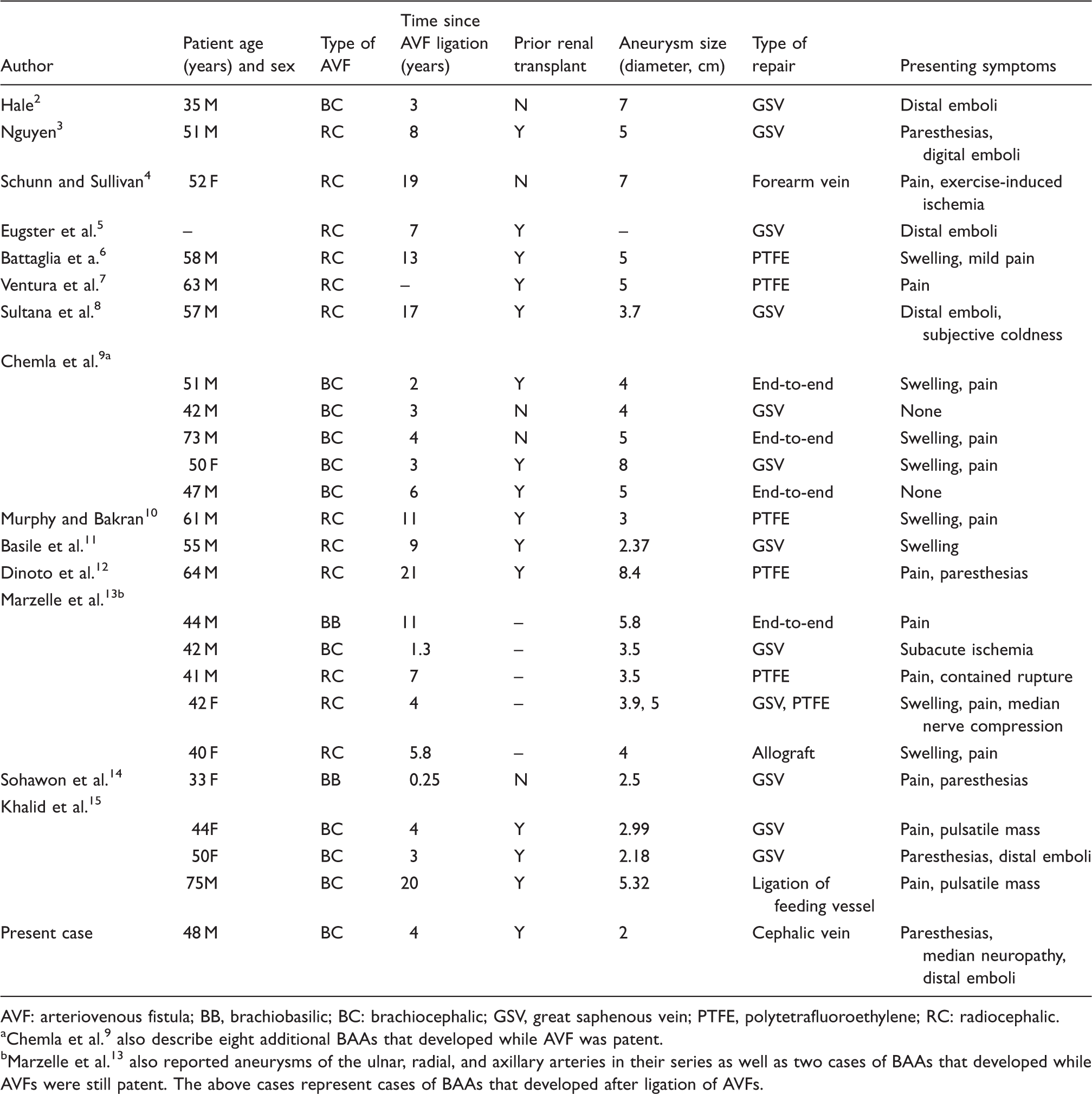
AVF: arteriovenous fistula; BB, brachiobasilic; BC: brachiocephalic; GSV, great saphenous vein; PTFE, polytetrafluoroethylene; RC: radiocephalic.
Chemla et al. 9 also describe eight additional BAAs that developed while AVF was patent.
Marzelle et al. 13 also reported aneurysms of the ulnar, radial, and axillary arteries in their series as well as two cases of BAAs that developed while AVFs were still patent. The above cases represent cases of BAAs that developed after ligation of AVFs.
Peripheral nerve compression at the site of AVF may contribute to distal paresthesias. As in this case, compression may be due to arterial aneurysm, but may also be a result of venous aneurysm, abscess formation, or hematoma. 21 Ultimately, our patient’s aneurysm was found to be compressing the median nerve. The initial differential diagnosis did, however, include ischemic monomelic neuropathy. Given the time course of his presentation and concern for distal ischemia secondary to both thrombosis within the aneurysm and distal thromboembolization, it was felt that immediate operative intervention precluded more invasive diagnostic testing such as nerve conduction studies. The preoperative Doppler and MRA studies did not clearly identify vascular compromise of the median nerve, and the intraoperative identification of the aneurysmal sac encasing the nerve led us to believe that this was a significantly contributing factor in his distal paresthesias.
The treatment of upper extremity aneurysms is often described as similar to that of false aneurysms, which are far more common, given the frequency with which interventions are performed in the upper extremity. Resection of the aneurysm and reconstruction with reversed vein graft (usually saphenous) or prosthetic material is the “gold standard.”4,19 Vascular reconstruction is utilized to avoid later complications associated with brachial aneurysms such as microembolization and occlusion of the distal vasculature of the upper extremity. Endovascular repair can be used if the aneurysm occurs in a straight arterial segment that does not cross the joint. 22 Lifelong surveillance is required with ultrasound, as recurrence has occasionally been reported secondary to disease progression. Immunosuppression may well contribute to weakening of the arterial wall musculature and subsequent aneurysmal degeneration.3,9,12,23
Conclusion
True BAAs are rare, but can develop following ligation of AVF used for hemodialysis access. The risk for complications including neurovascular compromise is significant. Surgeons should therefore maintain a high index of clinical suspicion when evaluating patients with ligated AVFs in long-term follow-up and offer therapy whenever an aneurysm is identified.
Footnotes
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of this consent is available upon request.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.