
Abstract
The treatment of isolated calf vein thrombosis remains widely debated. This study highlights the characteristics of isolated calf vein thrombosis in cancer patients and compares to isolated calf vein thrombosis in patients without history of cancer. Between July 2013 and April 2014, a retrospective chart review of consecutive patients with isolated calf vein thrombosis was performed recording patient risk factors, ultrasound characteristics of the thrombus, treatment modalities, long-term recurrence of venous-thromboembolism, incidence of bleeding, and mortality. Of 131 patients with isolated calf vein thrombosis, 53 (40.1%) had history of cancer. Isolated calf vein thrombosis occurred at an older age in cancer patients (66.7 vs 58.5 years, p = 0.004). The anatomical characteristics of isolated calf vein thrombosis on ultrasound were comparable in both groups. Isolated calf vein thrombosis in cancer patients was less likely to be treated with anticoagulation (60.4% vs 80.8%, p = 0.018). However, a trend towards higher incidence of bleeding after initiation of anticoagulation for isolated calf vein thrombosis in cancer patients (11.3% vs 6.4%, p = 0.351) was noted. Mortality in cancer patients was higher (37.7% vs 9.00%, p < 0.001) but was unrelated to isolated calf vein thrombosis or its treatment. In conclusion, the risks of bleeding seem to exceed the benefits of anticoagulation in approximately 50% of cancer patients with isolated calf vein thrombosis. The management of isolated calf vein thrombosis does not seem to impact the survival of cancer patients.
Introduction
Venous thromboembolism (VTE) is a major medical, public health, and economic concern in the United States. While the exact incidence of these events being unknown, the office of the Surgeon-General estimates that around 350,000 individuals bear the brunt of this disease every year. 1 Based on data from the Worcester deep vein thrombosis (DVT) study, it is believed that most of the cases of DVT may go undiagnosed, thus raising the burden of the disease further.1,2 Whether to anticoagulate or perform serial ultrasound surveillance in patients with isolated calf vein thrombosis (ICVT) remains a widely debated topic, because of the weak evidence (Grade 2 C) supporting the currently available guidelines. 3 The decision is made on an individual basis after weighing the risks of proximal propagation and embolization without anticoagulation against the risk of bleeding with anticoagulation.4–6 Cancer was shown to be associated with propagation and recurrence of ICVT in several studies.7–9 However, the significance of ICVT in cancer patients and the impact of its management on survival in that patient population have not been studied. This study reviews the characteristics of ICVT and its treatment in patients with a diagnosis of cancer in comparison to patients without cancer.
Methods
A retrospective review of all lower extremity venous ultrasounds identifying a new positive DVT at Yale New Haven Hospital was performed between July 2013 and April 2014. The study was approved by the Human Investigation Committee. The electronic medical records of the patients with ICVT were reviewed in detail. ICVT was defined by the involvement of the axial and/or muscular veins of the leg, not extending to involve the popliteal veins or more proximal veins. Patients with concomitant pulmonary embolism (PE) were excluded.
Risk factors
The patients’ demographic information and risk factors were recorded. The risk factors identified were based on the Caprini risk assessment tool and Caprini scores were calculated for all the patients. 10 The patients were divided into two groups: patients with cancer and patients with no history of malignancy. Cancer patients were divided into patients who had a past history of cancer, an active cancer, and a metastatic cancer. The type of cancer was noted. The DVT was considered provoked if the patient had a recent history of major surgery, immobilization, long travel, or initiation of hormonal replacement therapy for female patients.
Ultrasonography
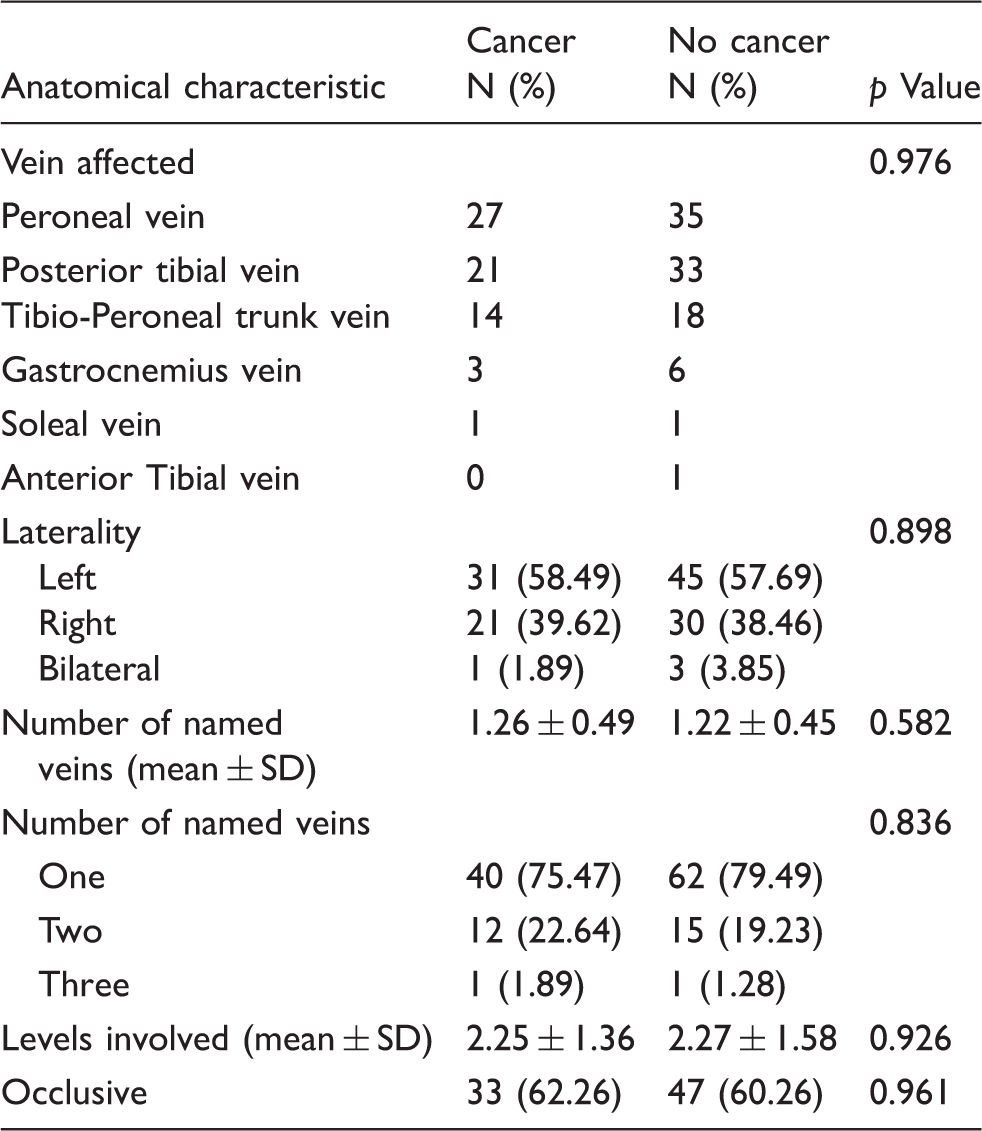
Anatomical data related to the location, laterality and extent of thrombus were recorded based on the ultrasound technologist work sheets. The veins examined were the tibioperoneal (TP) trunk vein, posterior tibial (PT) vein, peroneal vein, anterior tibial (AT) vein, gastrocnemius vein, and soleal vein. The number of named veins involved with DVT was recorded for each case. The PT vein and the peroneal vein were each divided into 3 levels (proximal, mid, and distal). The TP trunk, AT vein, and muscular veins were counted as one level each. The levels of thrombus involvement were recorded for each case as an estimate of thrombus burden. As such, a higher number of levels involved reflects a larger thrombus. ICVT with thrombus obstructing flow at any given level was considered as an occlusive DVT. ICVT without occlusive thrombus at all levels was considered a non-occlusive DVT.
Treatment
The treatment setting was examined. The patients were divided into three treatment groups: outpatient, admitted for diagnosis of VTE, and DVT admitted for unrelated condition and diagnosed with DVT as inpatient. The patients were anticoagulated if they received warfarin treatment with goal INR > 2.0 or any other anticoagulant in therapeutic dosage. The type and duration of anticoagulation were reviewed in patients who received anticoagulation. Treatment with Coumadin aimed at a goal INR <2.0 or the use of other anticoagulants in prophylactic dosage, as well as the use of antiplatelet medications were not considered anticoagulation. Contraindication to anticoagulation was noted for patients who did not receive anticoagulation. It was also recorded if patients underwent serial ultrasounds (repeat ultrasound within 1 month of diagnosis), or had IVC filter placement.
Follow up
The charts were reviewed for recurrence and proximal propagation of ICVT as well as for occurrence of PE during follow-up. Bleeding from anticoagulation was recorded. For patients who expired on follow-up, it was determined whether the management of ICVT or bleeding from anticoagulation contributed to mortality.
Data management and statistical analysis
The data collected was compiled using a Redcap (Research Electronic Data Capture) secure, web-based account. 11 Statistical comparisons between the two groups of patients were conducted using Chi square and Fisher’s exact tests when counts were more or less than five, respectively, or using two-sample t-tests for continuous variables. p Values less than 0.05 were considered statistically significant. A multivariate logistic regression analysis was used to evaluate the associations between demographic, treatment, and risk factors and the odds of recurrent DVT or bleeding complication. A forward selection algorithm based on the Akaike information criterion (AIC) was conducted to determine the most parsimonious model for each outcome. All analyses were conducted using R Statistical Software version 3.0.1.
Results
Incidence and risk factors
Demographics and risk factors of patients with isolated calf vein thrombosis (ICVT).

IBD: inflammatory bowel disease; COPD: chronic obstructive pulmonary disease; MI: myocardial infarction; CHF: congestive heart failure.
Anatomy
Ultrasound characteristics of isolated calf vein thrombosis (ICVT).
Management
Treatment of isolated calf vein thrombosis (ICVT).
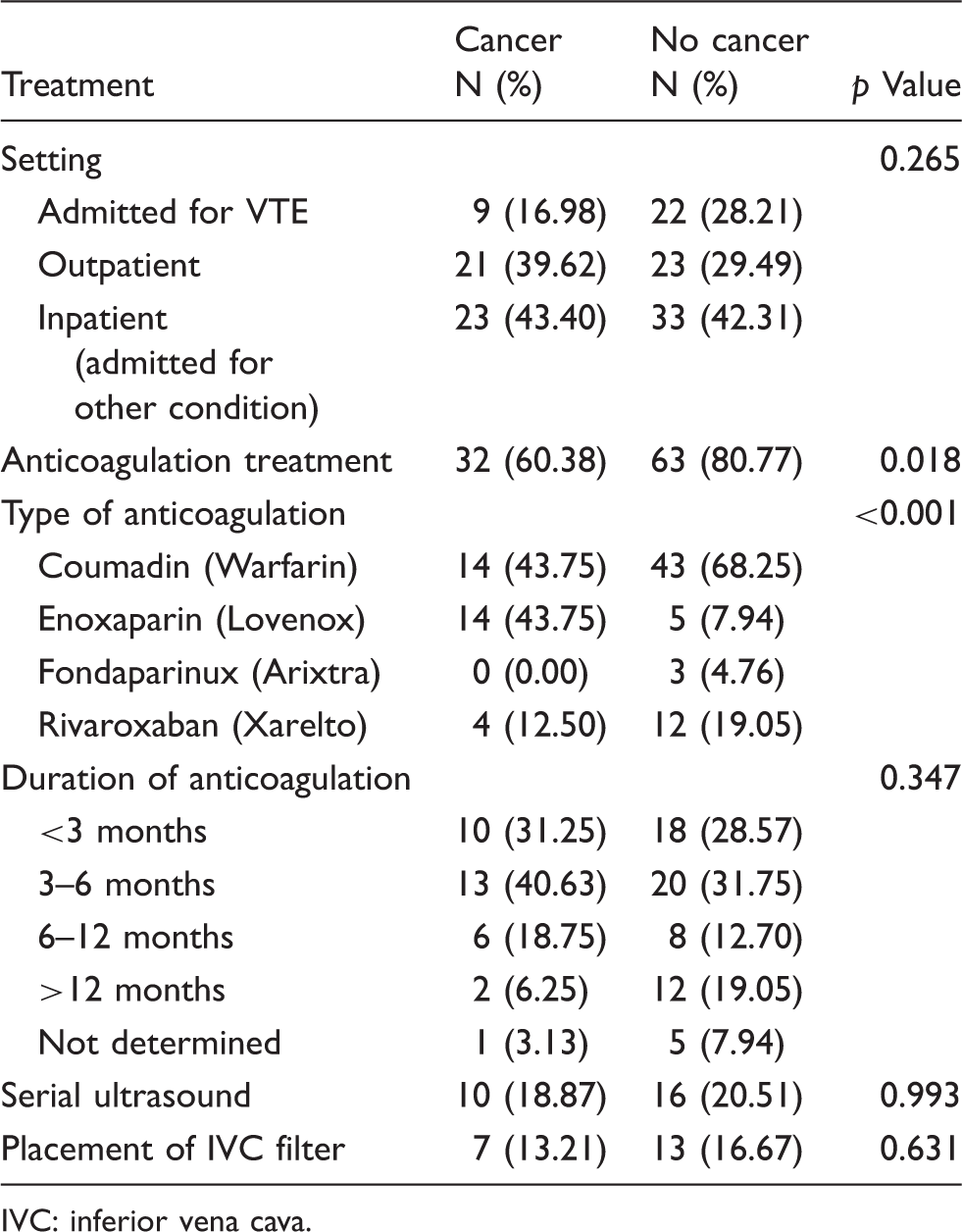
IVC: inferior vena cava.
Long-term follow-up
The mean duration of follow-up was 16.5 months. The recurrence rate of DVT in patients without cancer (14.10%) was no different from the recurrence in patients with cancer (9.43%) (p = 0.588). There was only one PE after ICVT that occurred in a patient without cancer 6 months after developing an unprovoked left peroneal vein thrombosis. The patient developed extensive bilateral iliofemoral DVTs as well as PE. He underwent IVC filter placement as well as catheter-directed thrombolytic therapy of the DVT. His hypercoagulable work-up was negative. There was no difference between the two groups in occurrence of PE during follow-up (p = 0.999). Patients with cancer tended to have more bleeding complications after initiation of anticoagulation (11.32%) compared to patients without cancer (6.41%) but that did not reach statistical significance (p = 0.351). All bleeding episodes required temporary or permanent cessation of anticoagulation and 54.54% (n = 6) of the 11 patients who developed bleeding received IVC filters. The sites of bleeding involved most commonly the soft tissue (n = 6), followed by CNS (n = 2), gastrointestinal tract (n = 2), and genitourinary system (n = 1). Patients with cancer had higher mortality (37.74%) than patients without cancer (9.00%) (p < 0.001). The mortality was mostly related to the malignancy and the high number of patients with metastasis. In fact, 56.52% (n = 13) of the patients who had metastatic cancer at the time of diagnosis with ICVT expired on follow-up. Twelve patients (22.64% of all cancer patients) expired within 6 months of the diagnosis with ICVT. There were no mortalities related to the diagnosis of ICVT, recurrent venous thromboembolism, or to complications emanating from treatment of ICVT.
Multivariate analysis
Covariates included in reduced multivariate logistic regression models for DVT recurrence. a
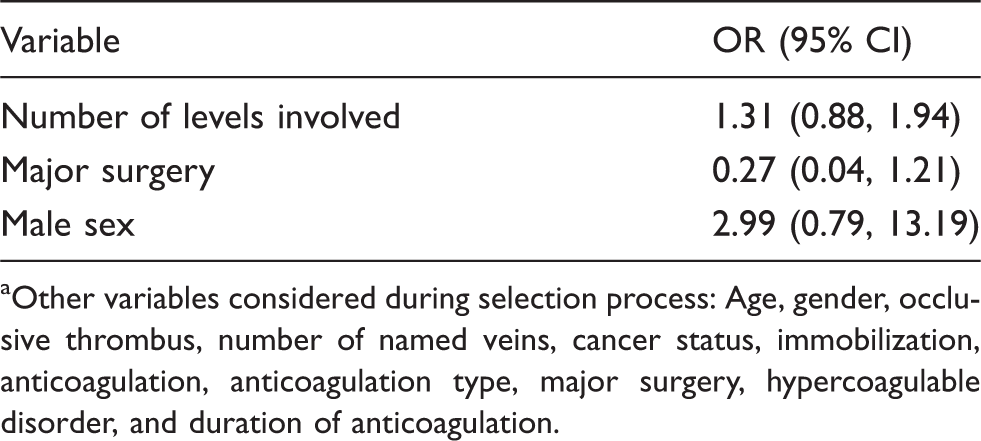
Other variables considered during selection process: Age, gender, occlusive thrombus, number of named veins, cancer status, immobilization, anticoagulation, anticoagulation type, major surgery, hypercoagulable disorder, and duration of anticoagulation.
Discussion
The 9th edition of the American College of Chest Physicians (ACCP) guidelines recommends anticoagulation for at least 3 months for cancer patients diagnosed with ICVT using low-molecular-weight heparin as the agent of choice. 3 Cancer patients who received anticoagulation in the current report were more likely to be treated with enoxaparin for at least 3 months consistent with the guidelines. Still, 43.75% of cancer patients received coumadin despite compelling evidence suggesting superior effectiveness for low-molecular-weight heparin in that patient population. 12 That may be attributed to higher costs of low-molecular-weight heparin. Interestingly, the data suggest that the risk of bleeding precluded 40% of cancer patients with ICVT from receiving full anticoagulation. Moreover, 11.32% developed bleeding that required cessation of anticoagulation at least temporarily. This finding is consistent with a study by Prandoni et al. 13 who reported an elevated bleeding rate of 12.4% per year for cancer patients on anticoagulation as compared to only 4.9% in patients without cancer. The risk of bleeding was higher in patients with metastasis compared to patients with less-advanced cancer stage. The high incidence of bleeding is likely related to primary or metastatic malignant lesions that are susceptible to bleeding in addition to thrombocytopenia that commonly develops with treatment.
Contrary to prior reports, patients with cancer in the current study did not have higher recurrence of DVT compared to patients with no history of cancer. Sartori et al. 9 studied 90 patients with ICVT over a period of 2 years. Cancer, which affected 8.9% of the patients, increased the risk of recurrence and propagation of DVT five-folds. There was one mortality related to cancer. In another study examining gastrocnemius and soleal vein thrombosis, cancer was found to be the only factor associated with thrombus propagation. 8 Singh et al. 14 followed patients with serial ultrasounds after ICVT and suggested that patients with cancer were at increased risk of propagation and recurrence even though a statistical analysis was not performed. Other reports that focus on ICVT treatments and outcomes have excluded patients with cancer.15,16 In fact, most papers suggesting that cancer patients have higher risk of recurrent VTE have studied patients with exclusively proximal DVTs, 17 or a group of patients with predominantly proximal DVTs13,18,19 without a clear distinction of risk of recurrence between proximal and distal DVTs. One possible explanation for the lower recurrence rate of DVT in the group of cancer patients in our study may be related to the very high mortality (37.74%). Most mortalities (22.64%) occurred in the first 6 months after diagnosis of ICVT, as such patients may have expired prior to having recurrence. To account for this, we performed a separate analysis including only patients who survived or had a follow-up of at least 6 months from the initial diagnosis of ICVT. This analysis revealed the same result and there was no significant difference in recurrence of DVT between the two groups (data not shown).
On the other hand, the similarity in the ultrasound characteristics of the thrombus in the two groups was very striking. There was no difference in the type or number of veins involved. There was no difference in thrombus burden neither as assessed by the number of levels or number of veins involved. Recently, the results of a French multicenter study examining 490 patients with ICVT showed that thrombus burden as measured by number of veins affected was a predictor of recurrence of ICVT. The location of the thrombus affecting axial or muscular veins did not affect recurrence. 16 Similarly, in an open randomized controlled trial comparing 6 weeks of anticoagulation to 12 weeks for treatment of surgical patients with ICVT, Ferrara et al. 15 found that patients with more than one vein involved had statistically significantly higher DVT recurrence if treated with 6 weeks only. Based on their findings, the authors recommended 12 weeks of anticoagulation at least for patient with ICVT affecting more than one vein. Interestingly, the results of the multivariate analysis suggest that thrombus burden is potentially a predictor of recurrence with each additional level of thrombus involved increasing the risk of recurrence by 1.48 times. Therefore, a similar thrombus burden in the two groups may explain comparable recurrence rate of DVT. Also, the two groups had identical baseline risk for developing VTE based on the Caprini scoring system. The results of multivariate analysis also suggested a reduced odds of recurrence for ICVT, among patients with major surgery as a transient provoking factor. These results are similar to other larger studies, which support the lower rate of recurrence in provoked ICVT and VTE.16,20,21 Iorio et al. 20 in their systematic review found that in patients with an index VTE provoked by a transient risk factor, the risk of recurrence was much lower (about one third) if VTE was provoked by surgery relative to a non-surgical factor.
The management of ICVT did not seem to affect the mortality of patients with cancer. The RIETE international registry (11,086 patients) for VTE demonstrated that 17.3% of DVTs were ICVT. A significant proportion of the patients in that registry were affected by cancer (20.1%). The mortality from ICVT was determined at 3 months to be 2.7% and was mostly related to the malignancy. Active cancer was the main predictive factor of death in patients with ICVT. 22 The high mortality in the group of patients with cancer in the current study is partly due to the longer follow-up period (16.5 months). In addition, the tertiary care center where the research was conducted has a clinically busy cancer center and is a regional referral center that possibly introduces bias with respect to the selection of the cancer patient population. One limitation of the study is the retrospective nature bounded by the information available that can be derived from electronic charts. Moreover, the follow-up data does not contain autopsy information and it is possible that some of the patients that expired after discharge could have developed a massive PE or a fatal hemorrhage.
In conclusion, ICVT in cancer patients is less likely to be treated with anticoagulation as compared to ICVT in patients without cancer. The risks of bleeding outweigh the benefits of anticoagulation in approximately 50% of cancer patients with ICVT. The diagnosis of ICVT and its management does not seem to affect the mortality of patients with cancer who succumb to their primary disease.
Footnotes
Acknowledgements
The authors thank the Redcap team for the indispensable, efficient, and secure data compilation tool provided for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research ethics
Approval was obtained from the Human Investigations Committee (HIC protocol number: 1404083818) at Yale University, New Haven, CT, USA, prior to initiation of the study.