
Abstract
Osteoarthritis is one of the most common chronic diseases and associated with increased cardiovascular comorbidity and deaths. Elastic properties of aorta are closely associated with cardiovascular mortality and morbidity. In our study, we aimed to evaluate aortic stiffness in primary osteoarthritis patients. A total of 160 patients including 80 patients with primary knee osteoarthritis and 80 controls without osteoarthritis were included in the study. Additionally, osteoarthritis patients were divided into four subgroups according to the severity of the disease. Aortic parameters were evaluated by using transthoracic echocardiography method. While measurements of aortic stiffness of osteoarthritis group were higher compared to the control group (p < 0.01), aortic strain and aortic distensibility measurements of osteoarthritis group are lower than the control group (p < 0.01). Additionally, it was determined that as the severity of osteoarthritis increased also aortic stiffness increased highly significantly (p = 0.001). Presence and severity of osteoarthritis are closely associated with elastic properties of aorta, which are correlated with cardiovascular mortality and morbidity.
Introduction
Osteoarthritis (OA) is one of the most common chronic diseases in elderly people. Therefore, it is also the most common condition affecting daily activity and it can significantly impair the quality of life. It is estimated that 9.6% of males and 18% of females suffer from symptomatic OA of the hips or knees all around the world. There have been reports associating OA with increased cardiovascular (CV) comorbidity and CV deaths.1,2 The reasons for this are multifactorial and not known exactly. OA results from progressive degeneration of articular cartilage because of wear and tear. Additionally, inflammation and free radical-induced oxidative damage may also play an important role in OA pathogenesis. 3 There are some important evidence about the relationship between the vascular system and the development and progression of OA. 4
Arterial compliance and stiffness of the ascending aorta are important pieces of the elastic nature of the arterial system and elastic properties, the aorta play an important role in sustaining normal CV physiology. 5 Aortic stiffness defines the elastic resistance as the aorta’s strength to its enlargement. Aortic stiffness is one of the most important CV risk factors predicting CV morbidity and mortality. 6 Aortic stiffness has been shown to increase with hypertension, diabetes mellitus, atherosclerosis, Marfan syndrome, smoking and aging in previous studies.7,8 Increase in oxidative stress causes reduction of bioavailability of adenosine triphosphate, arginine and nitric oxide. Consequently, endothelial dysfunction develops due to the chronic inflammation and destructive process in the arterial wall initiates. It is likely to be frequent of coexistence of OA and vascular damage that share a common pathophysiology like oxidative stress and inflammation. Aortic elasticity can be examined by using various parameters noninvasively with echocardiography. 9
Our aim was to investigate the correlation between presence and severity of OA and aortic stiffness for the first time.
Methods
A total of 160 patients including 80 patients with primary knee OA and 80 controls without OA were included in our study. The causes of secondary OA (previous knee surgery, intra-articular fracture and major knee trauma) were excluded from the study. Diagnosis and classification of primary OA was performed by using the following Kellgren-Lawrence classification which was radiological diagnostic criteria;
10
Grade 0 - no radiographic features of OA are present Grade 1 - doubtful joint space narrowing (JSN) and possible osteophytic lipping Grade 2 - the presence of definite osteophytes and possible JSN on anteroposterior weight-bearing radiograph. Grade 3 - multiple osteophytes, definite JSN, sclerosis, possible bony deformity Grade 4 - large osteophytes, marked JSN, severe sclerosis and definitely bony deformity
A second group of age- and sex-matched individuals served as controls, with no history of trauma to the knees or familial predisposition to OA, knee pain or clinical signs of knee OA and grade 0 on the Kellgren-Lawrence scale on the knee and hip X-rays. In addition, they had no history or clinical signs and symptoms of OA in other joints. Patients were excluded from the study if they had coronary artery disease, severe valvular disease, hypertrophic cardiomyopathy, chronic obstructive pulmonary disease, malignancy, congenital heart disease, chronic heart failure, cardiac rhythm other than sinus, uncontrolled hypertension (HT), systemic disease such as diabetes mellitus, collagenases, chronic autoimmune, hemolytic, hepatic and chronic renal disease, history of alcohol abuse, smokers or inadequate transthoracic echocardiographic images. Patients who had smoked at any time of his/her life were not included in the study because aortic parameters may be affected from the early ages. Hypertension was defined as blood pressure >140/90 mm Hg or under current antihypertensive medication and diabetic patients were defined as individuals receiving insulin or oral hypoglycemic agents or those with an HbA1c level of ≥6.5%, fasting plasma glucose level of 126 mg/dL. The estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration equation. Patients with an eGFR <60 mL/min/1.73 m2 were excluded from the study.
The study protocol was approved by the local ethics committee and written informed consent was obtained from each subject.
Clinical and laboratory examinations
All patients underwent clinical and laboratory examinations. Demographic data including classical risk factors of atherosclerosis (HT, dyslipidemia, smoking) were noted. Supine systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured three times in the right arm using an automatic oscillometric device (Dinamap PRO 300; Critikon) according to the recommendations of the American Heart Association. Blood pressure measurements were performed every 5 minutes by the same trained nurse. Blood samples were obtained after overnight fasting. Plasma glucose, high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglyceride (TG) and C-reactive protein (CRP) levels were measured using standard methods.
Transthoracic echocardiography
In order to avoid circadian changes that may affect arterial stiffness measurements, we examined all participants in the morning approximately at the same time of the day. Echocardiographic examinations were performed by the same cardiologist who do not know whether the one belongs to the patient or control group in order to prevent the interobserver variability.
All of the patients underwent transthoracic echocardiography using VIVID 3 (GE Medical Systems, USA). The measurements were obtained using a 1.5–3.3 MHz probe according to the updated ACC/AHA guidelines, while the patient was in the lateral decubitus position. Aortic elasticity was evaluated using a two-dimensional guided M-mode evaluation of systolic aortic diameter (AoS) and diastolic aortic diameter (AoD), 3 cm above the aortic valve.9–11 AoS was measured at the maximal anterior motion of the aorta, while AoD was measured at the peak of the QRS complex on the simultaneously recorded electrocardiogram. Internal aortic diameters were measured by means of a caliper in systole and diastole as the distance between the trailing edge of the anterior aortic wall and the leading edge of the posterior aortic wall. Three consecutive measurements were averaged. Gain controls were adjusted to enhance the tracking of the aortic endothelium-blood interface. The following aortic elasticity indices were calculated: % Aortic strain = 100 × AoS-AoD/AoD, Aortic distensibility = [2 × (AoS-AoD)/AoD (pulse pressure)] (cm2.dyn−1.10−6); and aortic stiffness (AS) = In (SBP/DBP)/[(AoS-AoD)/ AoD]. Pulse pressure was calculated as SBP-DBP, and In (SBP/DBP) refers to the natural logarithm of the relative pressure.9–11
Statistical evaluations
Number Cruncher Statistical System (NCSS) 2007 & Power Analysis and Sample Size (PASS) 2008 Statistical Software (Utah, USA) program was used for the statistical analysis. During the evaluation of the study data, regarding the comparisons of descriptive statistical methods (Mean, Standard Deviation, Median, Frequency, and Ratio) as well as quantitative data, Student t test was used for the intergroup comparisons of parameters with normal distribution and Mann Whitney U test was used for the intergroup comparisons of parameters without normal distribution. One-way ANOVA test was used for the comparisons of the groups three or more with normal distribution, and Tukey’s HSD test was used to determine the group causing the difference. Kruskal Wallis test was used for the comparisons of the groups three or more without normal distribution and Mann Whitney U was used to determine the group causing the difference. Yates Continuity Correction test (Yates Corrected Chi square) was used for the comparison of qualitative data. To determine possible correlations between the variables and the grade of OA, Pearson's correlation coefficient was calculated for parametric data and Spearman's correlation coefficient was calculated for CRP. Multivariance regression analysis was used to investigate the independent factors correlated with OA. Significance was evaluated at the levels of p < 0.01 and p < 0.05.
Results
Evaluation of demographic characteristics, biochemical parameters and aortic parameters according to presence of osteoarthritis.
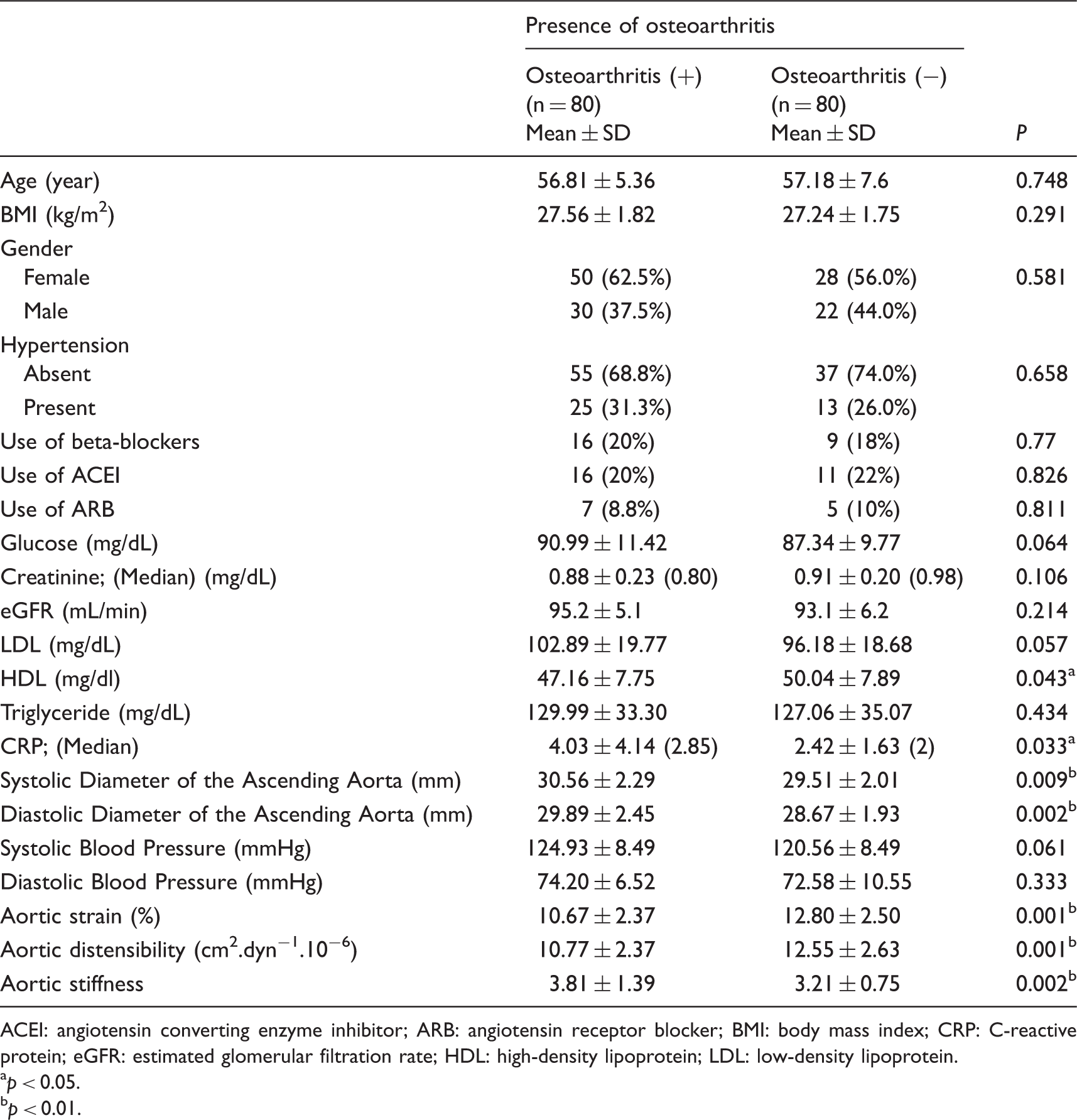
ACEI: angiotensin converting enzyme inhibitor; ARB: angiotensin receptor blocker; BMI: body mass index; CRP: C-reactive protein; eGFR: estimated glomerular filtration rate; HDL: high-density lipoprotein; LDL: low-density lipoprotein.
p < 0.05.
p < 0.01.
High level of intraobserver compliance has been detected in the analysis conducted for the determination of the degree of OA radiographically and echocardiographic measurements of aortic systolic and diastolic diameters (aorta systolic diameter intraclass correlation coefficient (ICC): 0.92 (95% CI: 0.95–0.98), aorta diastolic diameter ICC: 0.90 (95% CI: 0.88–0.91), Kappa coefficient for OA degree:0.89).
When the OA patients are evaluated according to the severity of the disease; 25.0% of them (n = 20) are Grade 1; 25.0% of them (n = 20) are Grade 2; 25.0% of them (n = 20) are Grade 3 and 25.0% of them (n = 20) are Grade 4.
AoS and AoD measurements of the OA patients are significantly higher than the AoS and AoD measurements of the control subjects (p < 0.01) (Table 1).
According to presence and absence of OA, highly statistically significant difference was determined with respect to aortic parameters. The aortic stiffness measurements of OA patients were found to be significantly higher than the aortic stiffness measurements of the control subjects (p < 0.01), but the aortic strain and aortic distensibility measurements of OA patients were significantly lower than the control subjects (p < 0.01) (Table 1; Figure 1).
Distribution of aortic stiffness, aortic strain and aortic distensibility measurements according to presence of osteoarthritis.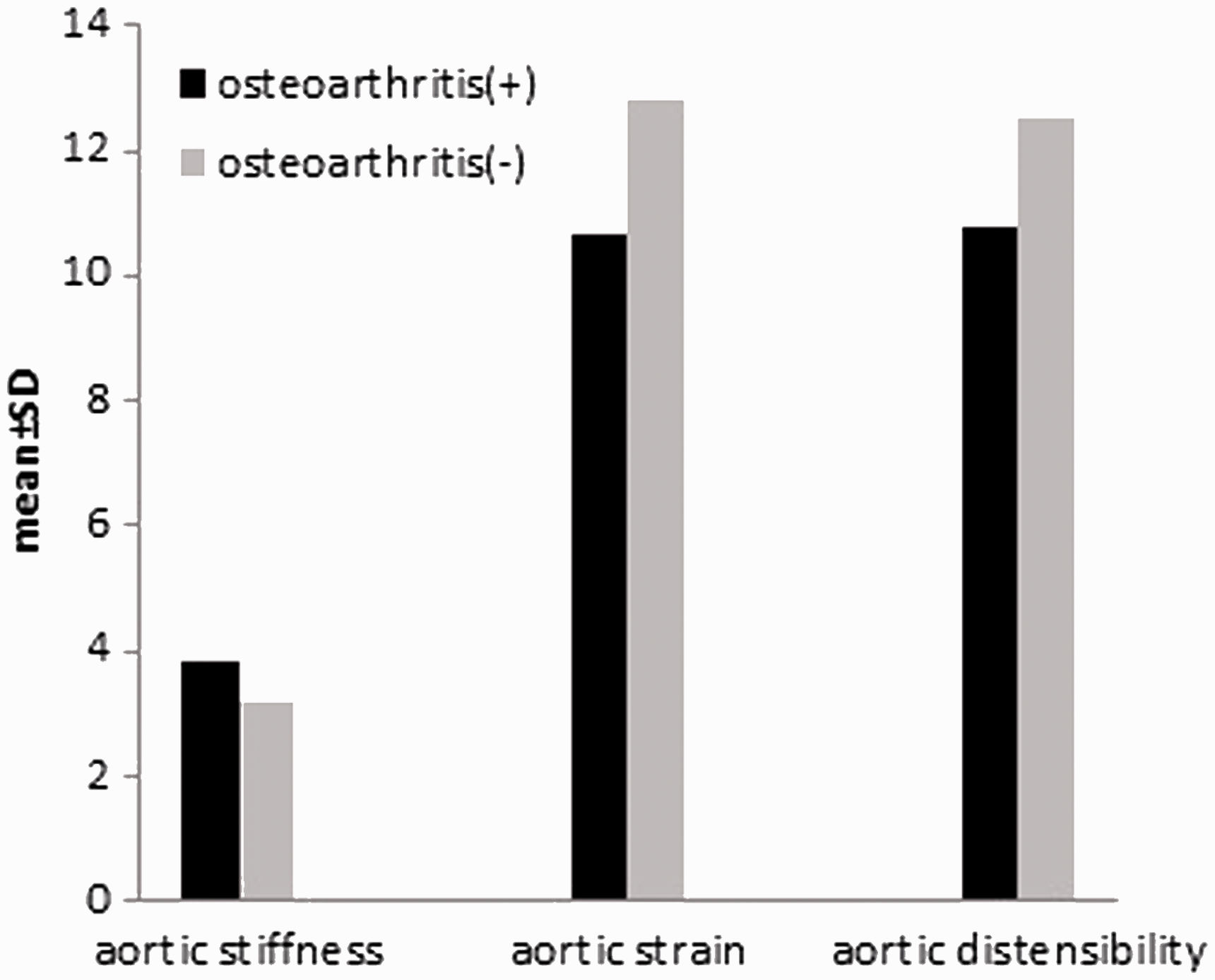
Evaluation of biochemical parameters, average blood pressures and aortic parameters according to osteoarthritis grade.
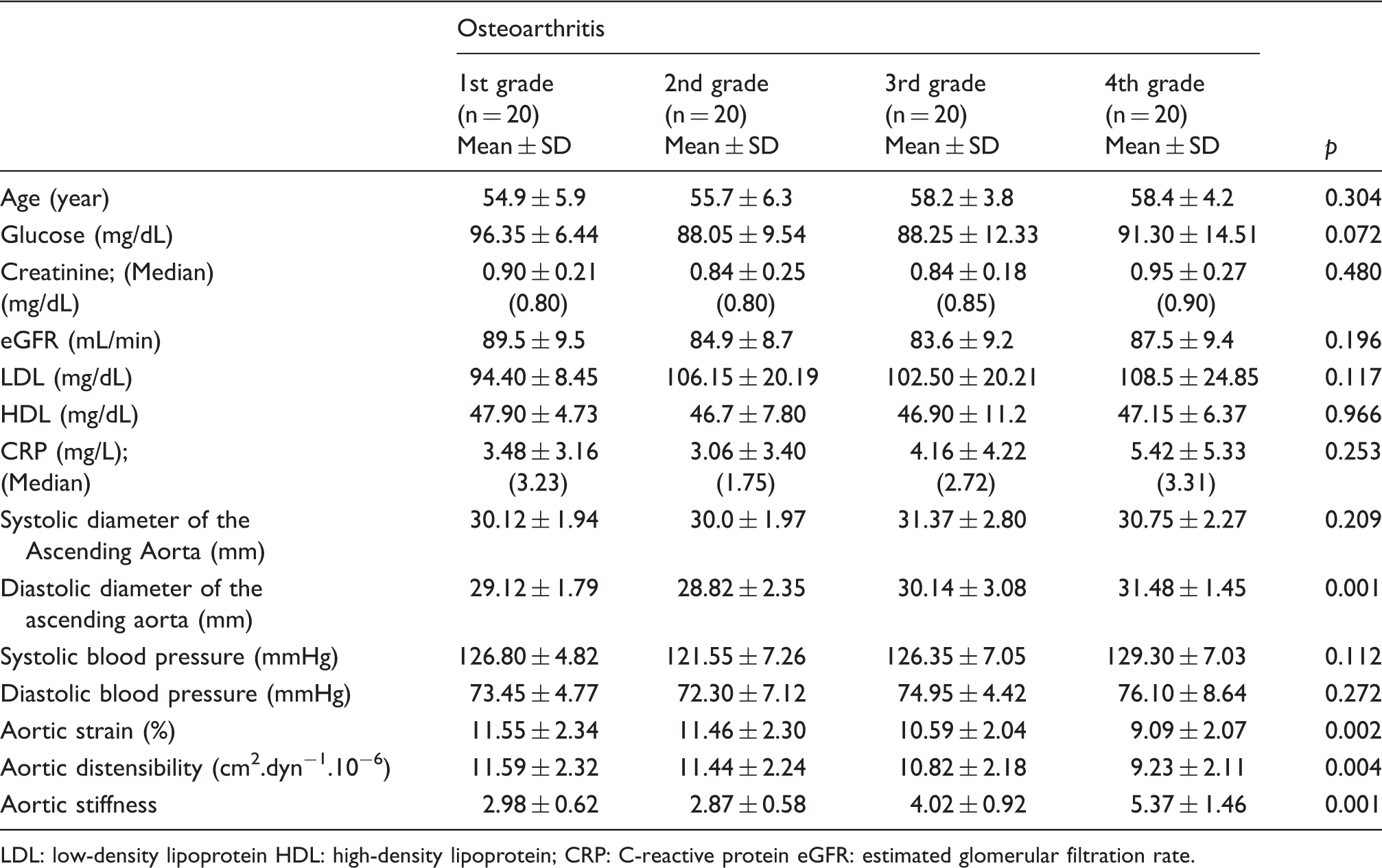
LDL: low-density lipoprotein HDL: high-density lipoprotein; CRP: C-reactive protein eGFR: estimated glomerular filtration rate.
Additionally, a highly statistically significant difference was determined between aortic strain measurements, when the OA patients were analyzed according to OA grades (p = 0.002) (Table 2). As per the dual comparisons performed to determine the group causing difference, it was found that aortic strain measurements of the patients with 4th grade OA were significantly less than the aortic strain measurements of the patients with 1st grade OA and 2nd grade OA, respectively (p = 0.004; p = 0.006).
With further analysis, a highly statistically significant difference was determined between the aortic distensibility measurements according to the degree of OA (p = 0.004) (Table 2). Again, aortic distensibility measurements of the patients with 4th grade OA were found to be significantly less than the aortic distensibility measurements of the patients with 1st grade OA and 2nd grade OA, respectively (p = 0.006; p = 0.012).
Further, a highly statistically significant difference was determined in the aortic stiffness measurements between the degree of OA (p = 0.001) (Table 2). As per the dual comparisons performed to determine the group causing difference, it was found that measurements of the patients with 4th grade OA were significantly higher than the measurements of the patients with 1st grade OA, 2nd grade OA and 3rd grade OA (p = 0.001; p = 0.001; p = 0.001), respectively. Additionally, the aortic stiffness measurements of the patients with 3rd grade OA were significantly higher than the aortic stiffness measurements of the patients with 1st grade OA and 2nd grade OA (p = 0.006; p = 0.002), respectively.
Again, with further analysis, while a highly statistically significant difference between degrees in OA was determined in the AoD measurements (p < 0.01), no statistically significant difference was determined in the AoS measurements (p > 0.05). As per the dual comparisons performed to determine the group causing the difference it was found that AoD measurements of the patients with 4th grade OA were significantly higher than AoD measurements of the patients with 1st grade OA and 2nd grade OA (p = 0.008; p = 0.002), respectively.
There were significant correlation between the grade of OA and aortic stiffness (p < 0.001, r = 0.676), aortic distensibility (p = 0.001, r = –0.367), aortic strain (p < 0.001, r = –0.391), diastolic aortic diameter (p < 0.001, r = 0.386) and age (p = 0.013, r = 0.276).
Multivariate logistic regression analysis.
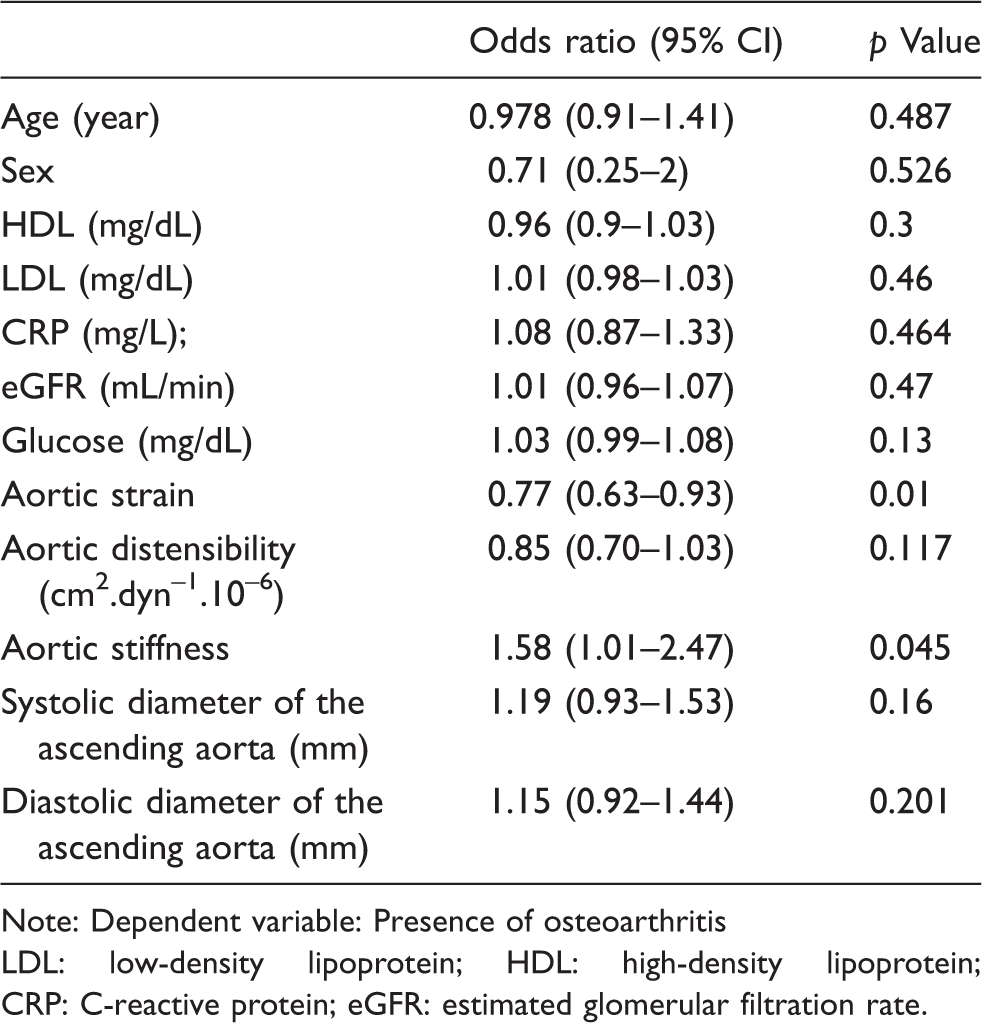
Note: Dependent variable: Presence of osteoarthritis
LDL: low-density lipoprotein; HDL: high-density lipoprotein; CRP: C-reactive protein; eGFR: estimated glomerular filtration rate.
Discussion
In our study, while there was no difference between OA and control group regarding age, gender and BMI, it was observed that aortic stiffness values of the patients with primary OA were significantly higher than the aortic stiffness values of the control group. Again, it was observed that aortic strain and distensibility which were the measurements showing the aortic elasticity were significantly less in OA group. In addition to this, when we classified the OA patients according to the severity of the disease, it was observed that these pathological vascular changes became significantly marked as the severity of OA increased even in the same group.
Reasons of relationship between OA and atherosclerosis are not fully known. Several factors may increase the risk of CV disease in OA: physical inactivity, 12 underlying inflammation 13 and use of non-steroidal anti-inflammatory drugs (NSAIDs). 14
Although OA is generally considered to be a degenerative arthropathy rather than an inflammatory arthropathy, recent findings suggest that inflammatory processes may play a role in its pathogenesis. 3 Synovial inflammation has been frequently described in early and advanced knee or hip OA 15 and systemic low-grade inflammation, as illustrated by elevated serum CRP levels. 16 The inflamed joint leads to increase of CRP synthesis by the liver via cytokines of joint tissue origin. Particularly, tumor necrosis factor-α (TNF-α), interleukin (IL)-6 and IL-1 up-regulated in OA, 17 involved in the pathophysiology of atherosclerosis. 18 Serum high-sensitivity CRP was positively associated with synovial inflammatory infiltrates and synovial fluid IL-6. This hypothesis has been proven in a recent study of knee OA. 19 Also in our study, CRP levels were determined to be significantly higher in the patients with OA compared to the patients without OA. Novel data suggests that inflammation may play a direct role in mediating arterial stiffness. 20 Patients with chronic inflammatory disorders have endothelial dysfunction and atherosclerosis which are more prevalent in these patients compared to age-matched controls. 21 Vascular stiffness has been associated with a number of other rheumatic diseases, including lupus erythematosus 22 and rheumatoid arthritis 23 due to chronic inflammation. CRP is associated with atherosclerosis and it is predictive of future ischemic events. 24 Some other potential mechanisms include the followings: adipokines, 25 cathepsin cysteine proteases 26 and extracellular membrane vesicles 27 and all of them are known to be involved in the pathophysiological processes of OA and atherosclerosis. Additionally, oxidative stress has been shown to promote both vascular disease and OA, 28 and experimental evidence has shown that reducing oxidative stress may decrease aortic stiffness. 29
In a previous 30 controlled study, evidence of subclinical atherosclerosis and endothelial dysfunction has been found in OA of the hand. In two population-based studies (Rotterdam 31 – Iceland 32 ), OA of the hand was found to be associated with carotid and coronary atherosclerosis. In the Framingham Heart study, an association was found between spinal facet joint OA and abdominal aortic calcifications which was a surrogate for CV disease, after adjustment of the traditional CV risk factors. 33 Also in a study conducted with MRI, it has been found that patients with generalized OA had significantly increased popliteal artery wall thickness. 34 However, other studies have found no association between the OA of the hand and arterial stiffness 35 or abdominal aortic calcification. 36 To the best of our knowledge, this is the first study evaluating the relationship between primary knee OA and aortic stiffness and we have determined the relationship between both the presence and degree of OA and aortic stiffness.
At least 40% of adults aged 65 or more are estimated to be physically inactive. The most frequent cause of limited activity in adults is OA. Decreased physical activity has a significant adverse effect on overall CV health. 37 The beneficial effects of physical activity on the CV system are largely related to repetitive episodes of increased laminar shear stress that acts favorably on the vascular endothelial structure and function rather than its effects on traditional CV risk factors. It has also been shown that aerobic physical activity helps to prevent arterial stiffening, 38 and furthermore aerobic training can reduce arterial stiffness. 39
OA is one of groups of diseases with the use of NSAID most commonly. Selective cyclooxygenase-2 (COX-2) inhibitors and most NSAIDs can be associated with increased risk of CV disease. 40 In a previous study, NSAID use was found to be an independent predictor of arterial wall compliance that was adjusted for age, blood pressure and arterial diameter. 41 According to one possible proposed mechanism, COX, in either isoform COX-1 or COX-2, controls synthesis of prostaglandin E2 (PGE2), which regulates expression of matrix metallopeptidase 9 (MMP-9). Miralles et al. 42 have shown that indomethacin decreased PGE2 and MMP-9 synthesis via inhibition of the COX-2 isoform. According to another possible proposed mechanism, the concentration of the aminoterminal propeptide of type III procollagen (PIIINP) was used as an index of type III collagen turnover and it has been detected that PIIINP levels were significantly higher in NSAID users and this suggested an up-regulation of type III collagen synthesis. 41 This result may partly explain the decreased aortic compliance found in the patients taking NSAIDs therapy.
Limitations
We evaluated knee OA and excluded the findings of OA in the other joints with history and clinically. However, it may not be possible to calculate the OA load in all of the body exactly. Additionally, our assessment of vascular stiffening by echocardiography only reflects central arterial stiffness. We did not assess the potential association between OA and properties of more distal arteries, for example, by measuring distal compliance, a correlate of microvascular stiffness that may reflect early vascular disease.
Conclusion
There is a close correlation between presence and severity of OA and aortic stiffness and the other properties of aorta. It was observed that vascular pathology became marked as the severity of OA increased. When these findings are evaluated together with the studies investigating the correlation between hand OA and atherosclerosis, it provides important information regarding the reasons of increased CV mortality in the patients with OA. Chronic low-grade inflammation in OA and additionally physical activity and frequently used NSAIDs may contribute to the development of vascular pathology.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.