
Abstract
Objective
To analyse the differences of outcome between cryostripping and conservative therapy in the treatment of superficial vein thrombosis.
Patients and methods
A retrospective analysis was performed between the October of 2001 and the October of 2014. In all, 246 cases were eligible for the study. High ligation, cryostripping and local thrombectomy was carried out on 94 patients with thrombophlebitis of the proximal part of the great saphenous vein. Thromboembolic events, the presence of residual varices and time for recovery were compared to 152 cases treated conservatively because of superficial vein thrombosis.
Results
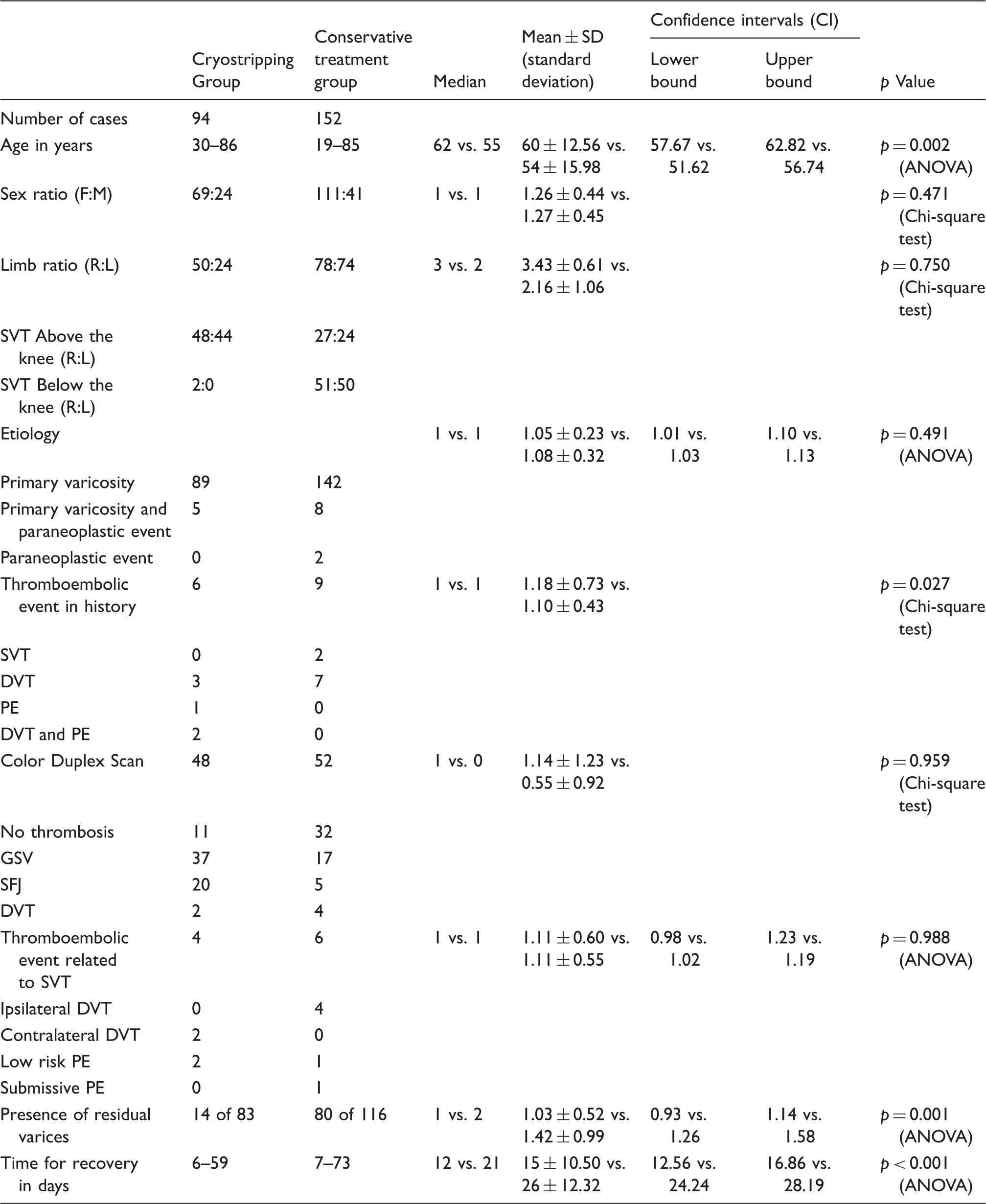
Thromboembolic events were found without significant difference (mean ± SD for surgery: 1.11 ± 0.60 and conservative therapy: 1.11 ± 0.55; p = 0.988) in each group. The presence of residual varices (mean ± SD for surgery: 1.03 ± 0.52 and conservative therapy: 1.42 ± 0.99; p = 0.001) and the time for recovery (mean ± SD for surgery: 15 ± 10.50 and conservative therapy: 26 ± 12.32; p < 0.001) were more favourable in the cryostripping group.
Conclusion
Our analysis confirmed that cryostripping does not result in a lower risk for thromboembolic complications due to superficial vein thrombosis but can be an alternative method to treat the ascending thrombophlebitis of the great saphenous vein because it has some advantages over conservative treatment on the short term.
Introduction
Superficial thrombophlebitis (ST) and superficial vein thrombosis (SVT) are synonyms. SVT is a common complication of varicosity and varies in appearance.1–3 If the GSV is affected, severe complications may occur; however, ipsilateral deep vein thrombosis (DVT) can develop by progression through the perforator veins even without the involvement of the GSV. Contralateral DVT is reported with a high risk, respectively. Pulmonary embolism (PE) is associated to SVT with a low risk.4–10
The treatment of SVT is routinely non-surgical. Low-molecular-weight heparin (LMWH) treatment should be administered regarding the recent evidences in every types of SVT to prevent thromboembolic complications at least 6 weeks long.4–6 On the other hand, if the thrombophlebitis of the GSV or small saphenous vein (SSV) approaches the saphenofemoral or saphenopopliteal junction (SFJ, SPJ) that can be assessed by colour duplex scanning (CDS), an urgent operation should be considered to avoid thromboembolic complications. Routinely, it means high ligation of the GSV or SSV with or without stripping.11–13 Due to lack of adequately designed and long-conducted studies the role of surgical interventions is not clarified. 4
Cryosurgery is feasible to treat the incompetence of the GSV. Cryostripping is an alternate to classical stripping. Cryosclerosis is the endovenous cryoablation of the GSV.14,15 Cryostripping seems to be appropriate to treat the ascending thrombophlebitis of the GSV.
Methods
Study design
A retrospective analysis of our cases was carried out from the available records between October 2001 and the October 2014. Patients treated due to SVT were searched. The records of patients characteristics (age, gender, limb ratio, etiology, history, the records of CDS, DVT/PE in history), thromboembolic events related to SVT, the presence of residual varices and the recovery period (days to regain full physical activity or to disappear the inflammatoric signs) were recorded by collecting the data from the available medical files.
Eligibility criterias
The inclusion criterias were the presence of any type of SVT and no previous surgical intervention on the superficial venous system. Patients who had high ligation with or without GSV stripping in history were excluded from the analysis.
Methodology
The non-surgical approach (Conservative Treatment Group – patients who were not selected for surgery because of less serious disease, symptoms occurred mid-thigh and/or below the knee, denial of surgery) consisted of wearing compression stockings, early mobilisation, venotonic drugs, NSAID, ointment containing heparin or derivates for 6–8 weeks. LMWH was not administered routinely. The Cryostripping Group consisted of patients with ascending thrombophlebitis of the GSV. Each patient had symptoms above the knee and the erythema neared to the groin. We used perioperative prophylactic LMWH shots (4000 NU enoxaparine daily). The patients were advised to wear compression stockings for 8 weeks after surgery. All surgical interventions were performed under spinal anaesthesia on an inpatient basis. The operation for the ascending thrombophlebitis of the GSV was nearly the same as for cases with primary varicose veins. High ligation of the GSV, proximal femoral cryostripping and local thrombectomy through microincisions were performed. We used the Erbokryo CA 300 device for cryostripping. CDS was performed just for 100 patients of the groups. If the ultrasound confirmed thrombus closer than 10 cm to the SFJ, surgical approach was also chosen.
Statistical analysis
Chi square tests were carried out to analyse the categorical variables (sex and limb ratios, DVT/PE in history, the records of CDS) and ANOVA was performed to compare variances between age, etiology, the occurrence of thromboembolic events, residual varices and time for recovery. The significance threshold was set at p < 0.05.
Results
Patients
Characteristics of groups and statistical results.
Thromboembolic events
CDS findings were available for the 34% and 51% of the cases in the conservative treatment and cryostripping groups, respectively. The ultrasound confirmed four ipsilateral DVT (6% of the cases; three of them were reported without the involvement of the GSV, one of these patients underwent surgery due to contralateral SVT previously and had DVT in history) in the conservatively treated group. Two patients suffered from PE in this group, neither ipsi- nor contralateral DVT were identified, one of them underwent surgery due to contralateral SVT several months earlier. Two contralateral DVT (2% of the cases; each was present with the involvement of the GSV, one patient had previous DVT) were reported in the cryostripping group. Two surgically treated patients suffered from PE, neither ipsi- nor contralateral DVT was identified, none of them had previous thromboembolic event, one of them had a cancer in history. During surgery, thrombus was found in the SFJ in 69% of the patients suffering from ascending GSV thrombophlebitis and 33 of them underwent CDS preoperatively, which confirmed 29 clots in the SFJ correctly (88% accuracy).
Residual varices, recovery and complications
A total of 69% of the conservatively treated patients and 15% in the cryostripping group had residual varices at follow up. The mean time for recovery was 26 and 15 days in the conservative treatment and cryostripping groups, respectively. There was no major bleeding observed after surgery. Severe wound healing disorder due to lymphorrhea occurred in two cases that needed additional wound care. Erythema after groin dissection and bruising were frequent.
Statistical analysis
Regarding the sex and limb ratios, etiology and the records of CDS, the groups were similar. The distribution of age (mean ± SD for surgery: 60 ± 12.56 and conservative therapy: 54 ± 15.98; p = 0,002) and thromboembolic events in history (mean ± SD for surgery: 1.18 ± 0.73 and conservative therapy: 1.10 ± 0.43; p = 0.027) were present with significant differences. Thromboembolic events related to SVT occurred with similar incidence in the groups (mean ± SD for surgery: 1.11 ± 0.60 and conservative therapy: 1.11 ± 0.55; p = 0,988). Residual varices were present with a lower rate in the cryostripping group (mean ± SD for surgery: 1.03 ± 0.52 and conservative therapy: 1.42 ± 0.99; p = 0,001). The time for recovery was significantly shorter after the operations than in the conservatively treated group (mean ± SD for surgery: 15 ± 10.50 and conservative therapy: 26 ± 12.32; p < 0.001).
Discussions
In general
A retrospective analysis is capable to collect information about diseases of low incidence; however, it has significant selection biases. Therefore, only two inclusion criteria were chosen for this study as the diagnosis of SVT and the presence of the GSV without previous surgical intervention. The latter was necessary for the comparison of conservative and surgical treatments.
Characteristics of patients
The significant differences regarding DVT/PE in history and the distribution of age may affect the results of this study. Previous DVT was more frequent in the conservatively treated group but there were cases with previous PE only between the patients who underwent surgery. It needs to be mentioned that of the 10 cases with thromboembolic event related to SVT in the whole study, three patients had previous SVT or either DVT or PE in history which indicates a possible correlation between thromboembolic events in history and complicated SVT. The recent publications did not regard the age as a risk factor for SVT.4,5
Thromboembolic events related to SVT
These complications were present with the similar incidence but different pattern in each group. The rate of detected DVT was lower than that presented by the papers of Nicolaides et al. and Hirmerova et al.4,5 PE occurred with similar incidence compared to the previously published by Nicolaides et al. 4 Our results have biases because there was insufficient information of the occurrence of DVT because CDS was performed only for the 41% of the involved patients, therefore, asymptomatic DVT are unrevealed. The latest evidences suggests that anticoagulant therapy for 6 weeks is necessary and the most important factor in the treatment of SVT.4–6 At the same time, it is hard to define the role of surgery. Our results show that 69% of the operated patients had a clot at the saphenofemoral junction. This situation represents an increased risk for thromboembolic complications and for this reason surgery can be justified, especially in case of progression of the symptoms.
Residual varices
Performing high ligation, cryostripping and local thrombectomy as primary surgical intervention seems to result in a reasonably low rate of residual varices compared to the conservatively treated patients. The thrombophlebitis of the tributaries seems to make the similar effect to sclerotherapy. This result does not differ from those observed by Disselhoff et al. 16 (28 of 60 patients who underwent cryostripping needed intervention due to residual varices).
Recovery
The mean time for recovery after surgery was 15 days; however, it took much longer (mean: 26 days) to regain full physical activity or lose symptoms for those patients treated conservatively. When common surgery is performed (high ligation of GSV without stripping) due to SVT, the recovery time is usually about 3–4 weeks or longer, and then the elective operation can be carried out. These patients are not able to go back to work during this period due to their symptoms so the whole recovery time together with the second operation can be around 8–10 weeks. The primary surgical intervention for SVT may give some advantages for the patients over the routine treatment (conservative therapy at the beginning then surgery when the inflammation settled) as the recovery time is significantly shorter. The mean days for convalescence were similar to those observed by Disselhoff et al., 17 however, the presence of SVT in our study should elongate the recovery.
Frequent complications
According to our experience, operating in an inflamed area did not increase the risk of wound infection due to lymphorrhea. The cases occurred with similar incidence compared to those observed by Disselhoff et al. and Menyhei et al.17,18
Conclusion
Primary surgery for GSV thrombophlebitis does not seem to provide a lower risk for further thromboembolic complications. It is hard to define when to decide to perform high ligation with or without cryostripping. The challenge is to specify the risk factors that can increase the chance for thromboembolic events. 5 Performing cryostripping due to the ascending thrombophlebitis of the GSV seems to result in a favourably low recurrence rate and shorter recovery.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.