
Abstract
Whether patients with renal artery stenosis should undergo therapeutic revascularization is controversial. In this retrospective study, we evaluated prognostic intrarenal Doppler ultrasound parameters that might have a predictive value for a beneficial response after renal revascularization. From January 2003 until December 2012, all renovascular interventions for renal artery stenosis were analyzed. The resistive index and the maximal systolic acceleration were determined by Doppler ultrasonography prior to intervention. Thirty-two patients who underwent a renal revascularization procedure were included: 13 combined positive responders and 19 combined non-responders. The combined positive responders had a significant lower resistive index than the combined non-responders (0.5 vs. 0.6, P = 0.001) and a significant lower maximal systolic acceleration (1.0 vs. 3.8, P = 0.001) before revascularization. A prediction model (RI ≤ 0.5 and ACCmax ≤ 1.3 m/s2) was formulated to identify a subgroup that benefits from renal revascularization. This model has an expected sensitivity of 69% and specificity of 89% for improvement in renal function and/or blood pressure after revascularization. The non-invasive intrarenal Doppler ultrasound parameters resistive index and maximal systolic acceleration can be used as tools to predict improvement in renal function and/or blood pressure after revascularization of renal artery stenosis. The clinical value of this prediction model should be evaluated in a prospective trial.
Keywords
Introduction
Renal artery stenosis (RAS) is a common cause of secondary hypertension and ischemic renal failure. 1 The prevalence of RAS is <1% in patients with mild to moderate hypertension. 2 But acute, severe or refractory hypertension and atherosclerosis elsewhere in the body highly increase the risk of RAS.3–5 The primary cause of RAS is atherosclerosis (90%) that is associated with conventional cardiovascular risk factors such as age, diabetes, dyslipidemia and hypertension. Furthermore, atherosclerotic RAS is a progressive disease.1,6 The second common cause of RAS is fibromuscular dysplasia (FMD), especially in young (female) adults.7,8
All patients with symptomatic RAS should receive medical treatment. 7 Whether patients with RAS should undergo therapeutic revascularization is far more controversial. Recent clinical trials such as the ASTRAL study, 9 STAR trial 10 and CORAL trial 11 found no significance difference in outcome (blood pressure, renal function and cardiovascular events) between revascularization plus medical therapy and medical therapy alone in patients with atherosclerotic renovascular disease. However, these studies did not close the debate on the value of revascularization therapy as a consequence of criticism concerning the design of these trials.5,12,13 Furthermore, various observational studies showed beneficial outcome of revascularization compared to medical treatment in selected patients. This applies, for example, to patients presenting with flash pulmonary edema.14–16 In addition, multiple case reports describe beneficial responses after renal revascularization therapy.17–23 One can postulate that there must be a subgroup of patients with a symptomatic RAS who will benefit from revascularization. Therefore, identification of prognostic parameters for a positive response after revascularization might improve patient selection and efficacy of revascularization therapy in patients with RAS.
Currently, various diagnostic strategies are available to detect renovascular disease. 2 The intrarenal Doppler ultrasound parameter maximal systolic acceleration (ACCmax) emerged as a good non-invasive tool for diagnosing RAS with a sensitivity of 83%–94%.24–26 Another ultrasound parameter is the resistive index (RI). The RI is a measure of pulsatile blood flow and is modified by vascular resistance and vascular compliance. 27 Increased RI is correlated with arteriolosclerosis, glomerulosclerosis and tubulointerstitial damage. 28 Previous studies revealed that a high RI correlates with no improvement in renal function and blood pressure after renal revascularization.29–31 However, there is no consensus which patients will have a positive response in renal function and/or blood pressure from revascularization.
The objective of this study was to identify prognostic intrarenal Doppler ultrasonography parameters that might have a predictive value for a positive response from renal revascularization. Therefore, we performed a retrospective study in which we compared patients who had a positive response from revascularization with patients who did not have such a response. We hypothesized that the RI and ACCmax might have prognostic value that could predict a positive response from revascularization in patients with RAS.
Materials and methods
Study population
The institutional review board approved this retrospective study and waived the need for informed consent. Patients with uncontrolled hypertension (e.g., systolic blood pressure >150 mmHg with two or more adequately dosed antihypertensive drugs) or unexplained renal dysfunction suggested a diagnosis of RAS. In these patients, renal arteries were visualized by digital subtraction angiography, magnetic resonance angiography or computed tomography angiography. A diameter stenosis of >70% was defined as a significant RAS. At our institution, the choice of treatment was made in consensus model during multidisciplinary conferences, in which vascular surgeons, nephrologists and interventional radiologists participate. Post-endovascular intervention patency was assessed directly after endovascular renal revascularization by angiography. After open surgery, all patients underwent Doppler ultrasonography and/or computed tomography angiography before discharge. An intraoperative complication and an occlusion or ≥10 mmHg post-stenotic pressure drop measured with a pressure wire in the renal artery directly after percutaneous revascularization were considered as a technically unsuccessful intervention.
All patients with endovascular and open renal revascularization between January 2003 and December 2012 were analyzed. In order to be included in this retrospective study, patients had to meet the following inclusion criteria: a reduction in the diameter of renal arteries of at least 70%, availability of laboratory data on renal function (estimated glomerular filtration rate (eGFR) calculated using the Modification of Diet in Renal Disease formula), mean arterial pressure (MAP) and Doppler ultrasonography parameters before intervention and availability of renal function and MAP six months after intervention. Technically unsuccessful revascularizations were excluded from this study.
Doppler ultrasonography
Since 2003, all intrarenal Doppler ultrasonography investigations were performed and well documented by the same vascular ultrasound specialist. The intrarenal Doppler ultrasonography parameters RI and ACCmax were performed using an Aloka SSD-5500 ultrasound system (Tokyo, Japan) with a 5–7.5 MHz transducer in the period of 2003–2008 and an ACUSON S2000 model (Siemens Medical Solutions Inc., Ultrasound Division, Issaquah, WA) with a 4C1 3–4.5 MHz Convex pro transducer in the period of 2008–2012. The other intrarenal Doppler ultrasound findings were peak systolic velocity (PSV) and end-diastolic velocity (EDV). All the intrarenal Doppler ultrasonography findings were measured distal in the interlobar arteries in the upper, middle and lower renal pole. RI was calculated by the following formula: (PSV–EDV)/PSV. The ACCmax was defined as described by Bardelli et al.
24
and was always performed with angle correction
32
as shown in Figure 1. The extrarenal Doppler ultrasound findings were PSV of the abdominal aorta, and PSV and EDV measured at or directly after the stenosis.
The RI (0.56) and ACCmax (0.46 m/s2) were obtained by intrarenal Doppler ultrasonography. For measuring ACCmax, the angle of insonation will be close to null because the course of the interlobar artery is mostly perpendicular to the surface of the kidney. In this example, the angle of insonation is 12°.
Definition of responses to intervention
To determine the efficacy of revascularization therapy, renal function (eGFR) and MAP were determined before and six months after intervention. Other studies defined positive response in renal function as 20% increase in eGFR after intervention.9,29,33 In our study, we defined an increase of ≥20% in eGFR and a decrease of ≥20% in MAP as positive responses, and these patients were classified as positive eGFR or MAP responders. Conversely, a decrease in eGFR of ≥20% or MAP increase of ≥20% was defined as negative responses.
Composite of the combined responders.
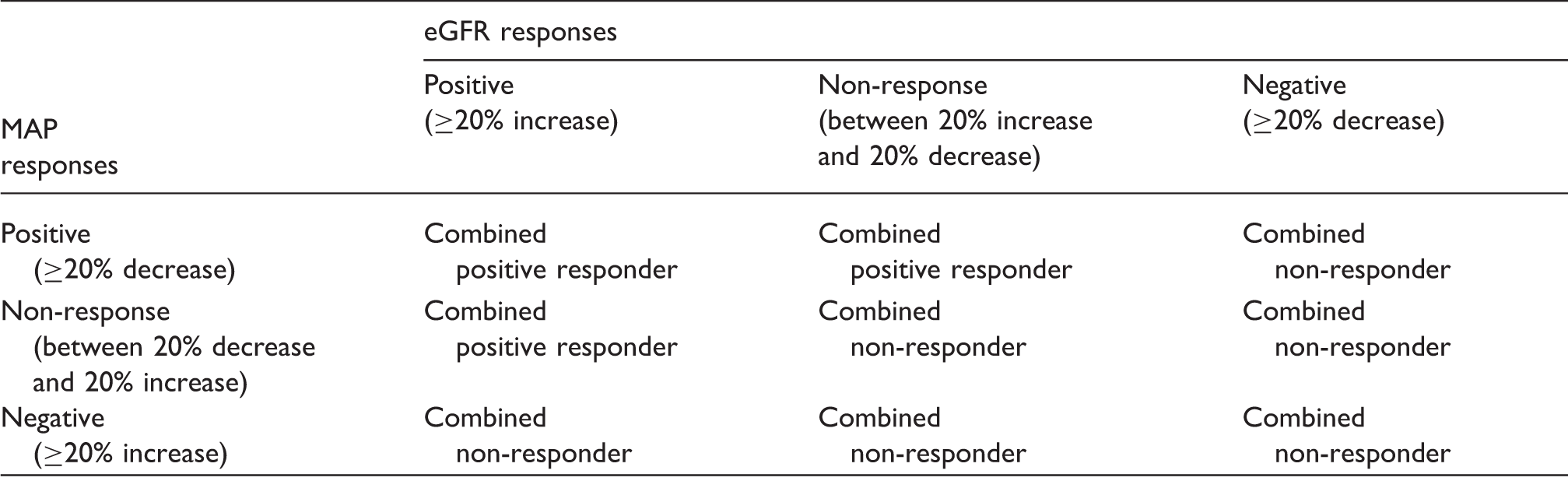
GFR: estimated Glomerular Filtration Rate; MAP: mean arterial pressure.
Statistical analysis
Data were collected into a Microsoft Access database and were analyzed using SPSS statistics 20 and Matlab (R 2014A) for all statistical analysis. The Wilcoxon signed-rank test (Mann–Whitney test) was used as non-parametric test to assess continuous measures differences between groups because the study population is small and not all parameters were normally distributed (ACCmax). To ensure a homogeneous way of statistical analysis, the Wilcoxon signed-rank test (Mann–Whitney test) was used for all statistical analyses where continuous measures differences between groups must be calculated. P values are given with median and interquartile range (IQR); 25th and 75th percentiles. The Chi-square test was used for analyzing two independent groups with categorical data. A P value <0.05 was considered statistically significant.
In this study, a prediction model was constructed, using a single cut-point on each variable (RI and ACCmax). To choose the cut-points, a grid of possible cut-points was defined for each variable by calculating percentiles from the observed values of RI and ACCmax in the data. For each combination of possible cut-points, classification performance was evaluated using a leave-one-out cross-validation procedure. We chose the model with minimal error rate among those models having a specificity of at least 80%. To obtain unbiased estimates of the error rates achievable with this model selection approach, the entire procedure was repeated using double cross-validation.34,35
Results
From January 2003 to December 2012, 104 interventions were indentified for symptomatic RAS at our institution. Of the 104 revascularizations, 5 were excluded due to technically unsuccessful intervention (e.g., occlusion or ≥10 mmHg post-stenotic pressure drop immediately after intervention). Doppler ultrasonography was not routinely performed for diagnosis of RAS, so we missed 54 RI and ACCmax data. Forty-five interventions remained, whereof eGFR and MAP responses were identified. Thirteen eGFR or MAP data were missing, so 32 interventions were included and analyzed in this study (Figure 2).
Flowchart of study selection.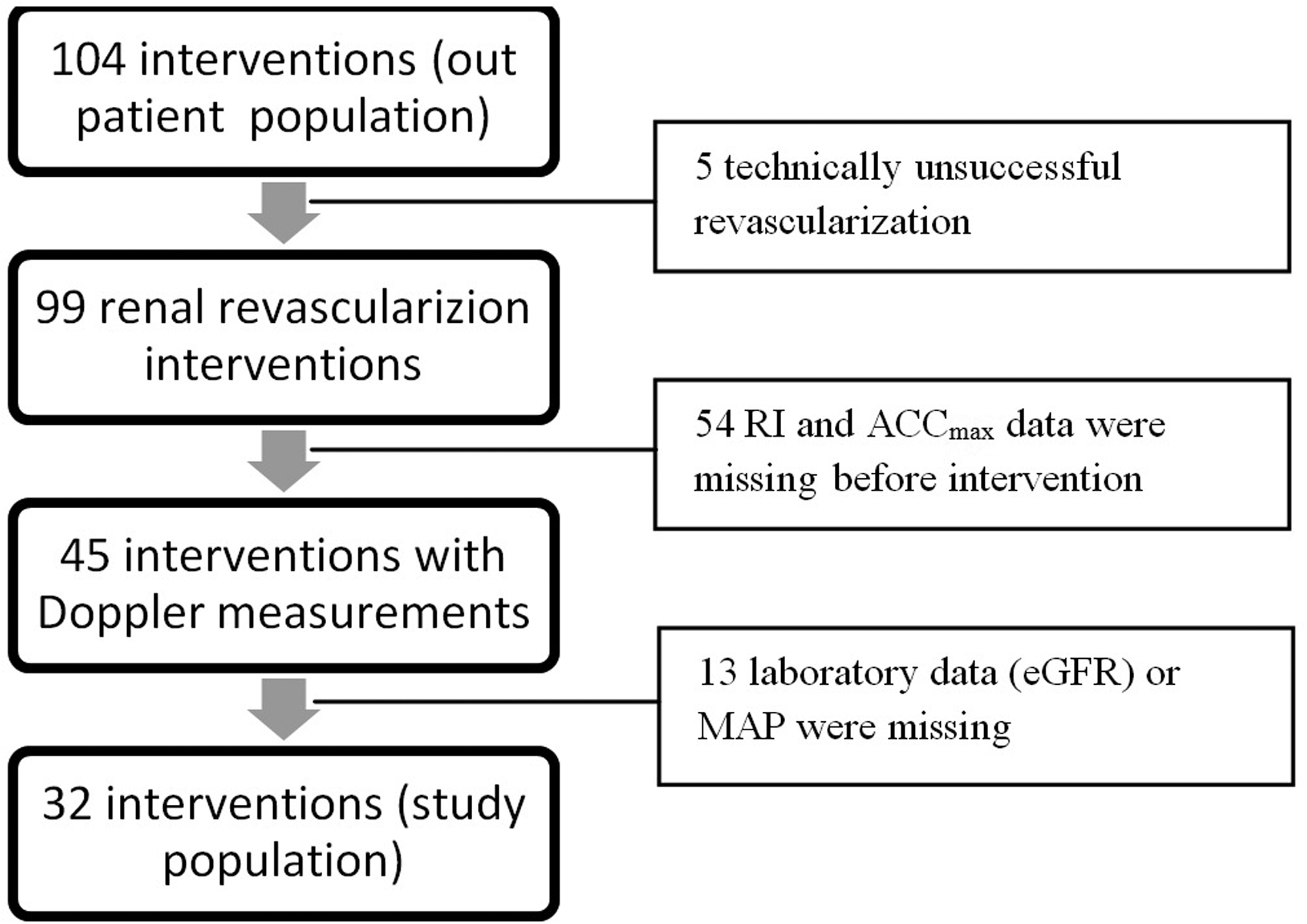
Baseline characteristics
Baseline characteristics.

AIE: external iliac artery; CIA: common iliac artery; eGFR: estimated Glomerular Filtration Rate; FMD: fibromuscular dysplasia; MAP: mean arterial pressure; NTx: renal transplant recipients; PTRA: percutaneous transluminal angioplasty interventions without a stent; PTRAS: percutaneous transluminal angioplasty interventions with a stent.
Iatrogenic stenosis due to a hemorrhaging complication of nephrectomy for Grawitz tumor. P value was calculated with use of the Wilcoxon signed-rank test (Mann–Whitney test) or the Chi-square test. Data are mean ± standard deviation (SD), median (IQR) or n (%). SD or IQR for continuous factors and frequency (%) for dichotomous factors.
We classified 32 interventions in two groups, 13 interventions were included in the combined positive responders group and 19 interventions in the combined non-responders group, based on eGFR and/or MAP response (see “Definition of responses to intervention” section). These groups were compared to find parameters that are characteristic of the combined positive responders. The mean eGFR, serum creatinine, MAP, systolic blood pressure, diastolic blood pressure, RI, ACCmax and number of antihypertensive drugs before and six months after intervention for the two groups are given in Table 2. No significant differences were found in demographic parameters, type of intervention, laboratory measures, blood pressure or number of antihypertensive drugs.
Responses on intervention
The combined positive responders (13/32) had a significant lower median RI than the combined non-responders (0.5, 0.4–0.6 vs. 0.6, 0.6–0.7; P = 0.001) and a significant lower median ACCmax (0.6, 0.5–1.3 vs. 2.1, 1.4–6.8; P = 0.001) before intervention (Figures 3 and 4).
Significant difference in resistive index (RI) before intervention between combined responders (P = 0.001) and eGFR responders (P = 0.002). Median and the highest and the lowest case within the IQR and 1.5 IQR (top and bottom whiskers) are given in the figure. Outliers are identified with an o. Significant difference in maximal systolic acceleration (ACCmax) before intervention between combined responders (P = 0.001) and eGFR responders (P < 0.001). Median and the highest and the lowest case within the IQR and 1.5 IQR (top and bottom whiskers) are given in the figure. Outliers are identified with an o, and extreme values are marked with an asterisk (*).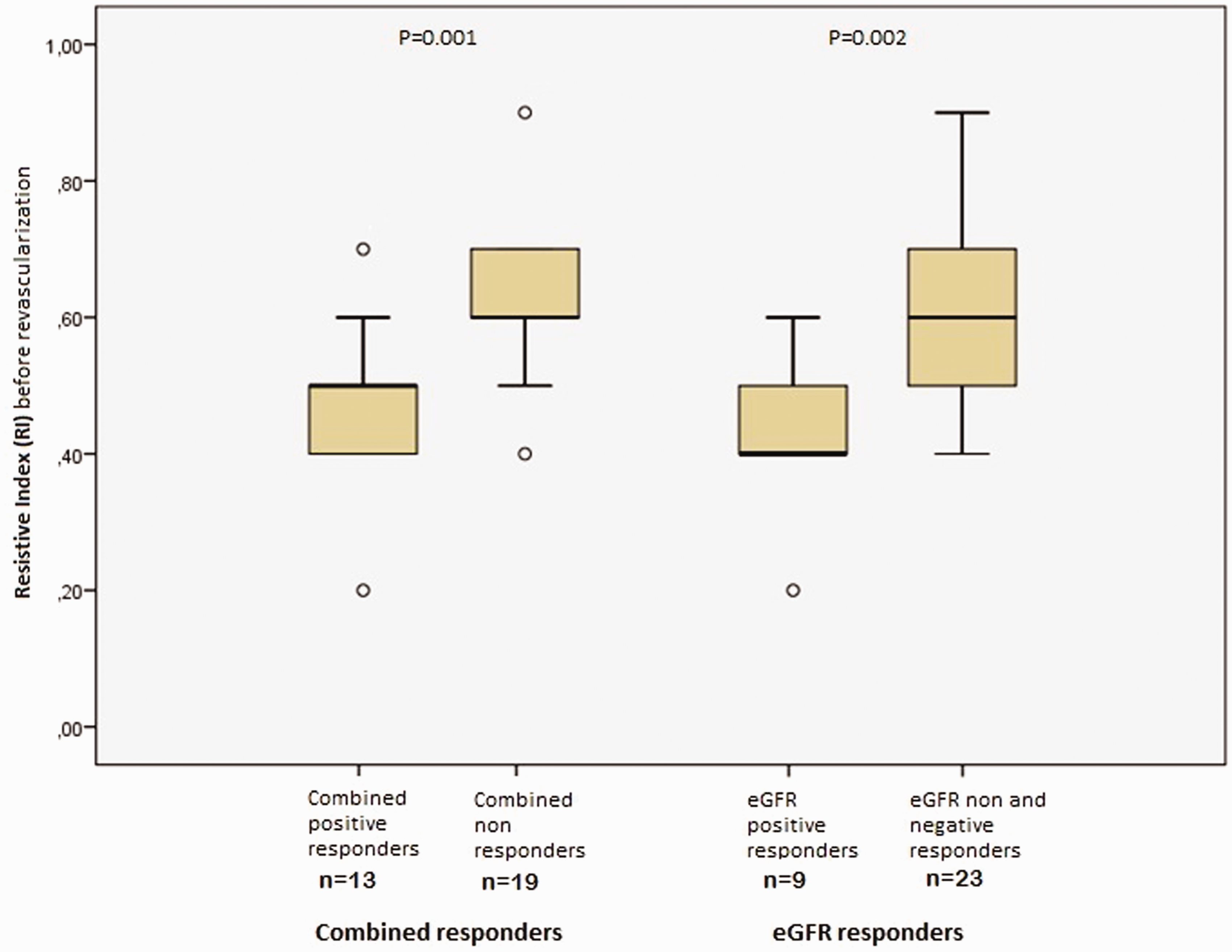
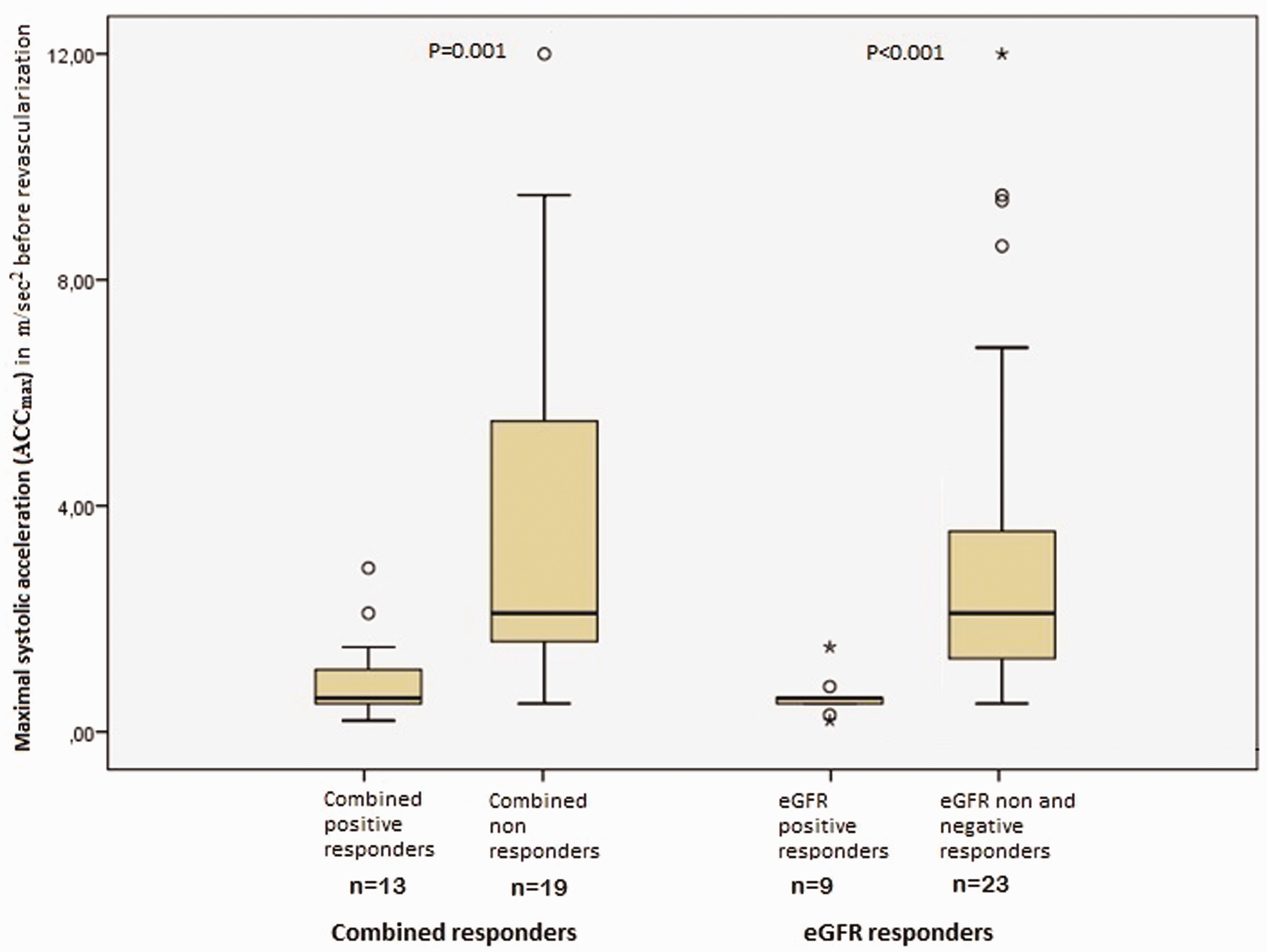
To answer the question of whether the RI and ACCmax were also predictive for renal function response alone, the eGFR responders were compared separately. The non- and negative eGFR responders were considered as one group because they both had no beneficial response in eGFR after revascularization. The positive eGFR responders (9/32) had a mean eGFR increase of 19 mL/min, and the non- and negative eGFR responders (23/32) had a mean decrease of 5 mL/min in eGFR. The positive eGFR responders compared with the non- and negative eGFR responders showed a significant lower median RI (0.4, 0.4–0.6 vs. 0.6, 0.5–0.7; P = 0.002) and a significant lower median ACCmax (0.6, 0.4–0.7 vs. 2.1, 1.2–4.2; P < 0.001) (Figures 3 and 4). A separate comparison between MAP responders was useless because 9 (of the 32) patients had a normal MAP at baseline.
Prediction model based on RI and ACCmax
A prediction model was formulated to identify a subgroup prior to intervention that will have a positive response from renal revascularization. The leave-one-out cross-validation procedure was used to determine the optimal cut-off values of RI and ACCmax, for classification of future patients. The best cut-off values for RI and ACCmax were respectively found at 0.5 and 1.3 m/s2. The prediction model classifies patients as expected positive responders if the patient scored at or below the respective cut-off points on both variables.
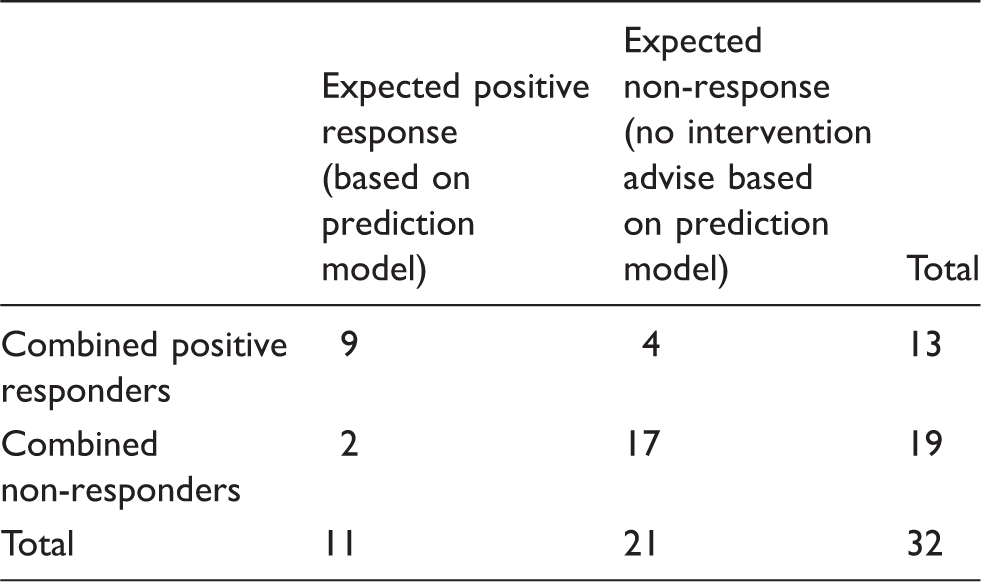
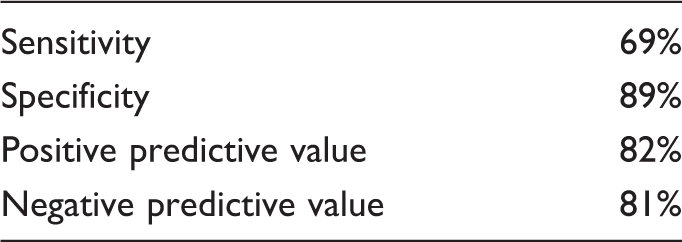
The performance of this prediction model was calculated by double cross-validation (see Tables 3 and 4). This statistical analysis estimates an expected sensitivity of 69% and specificity of 89% for a positive response after renal revascularization for application of the above-described rule on new patient observations (total double-cross-validated error rate was 6/32). The combination of individual intrarenal Doppler ultrasonography data (RI and ACCmax) of our study population and the unbiased calculated cut-off values are demonstrated in Figure 5.
Scatterplot of the RI and ACCmax with the cut-off values, respectively, 0.5 and 1.3 m/s2, from the total study population of 32 patients. Every symbol represents one patient. Readers should beware that the figure shows the observed patient measures with the chosen prediction model superimposed. Hence, the observed spread of observations in the figure is not directly comparable with the unbiased double cross-validatory estimates of classification performance (Tables 3 and 4) on future patients given in the text. A naïve comparison of patients with the thresholds shown would induce an optimistically biased assessment of classification performance. Confusion table: Combined responders and expected outcome. Expected statistical characteristics of the prediction model (based on double-cross-validation computation).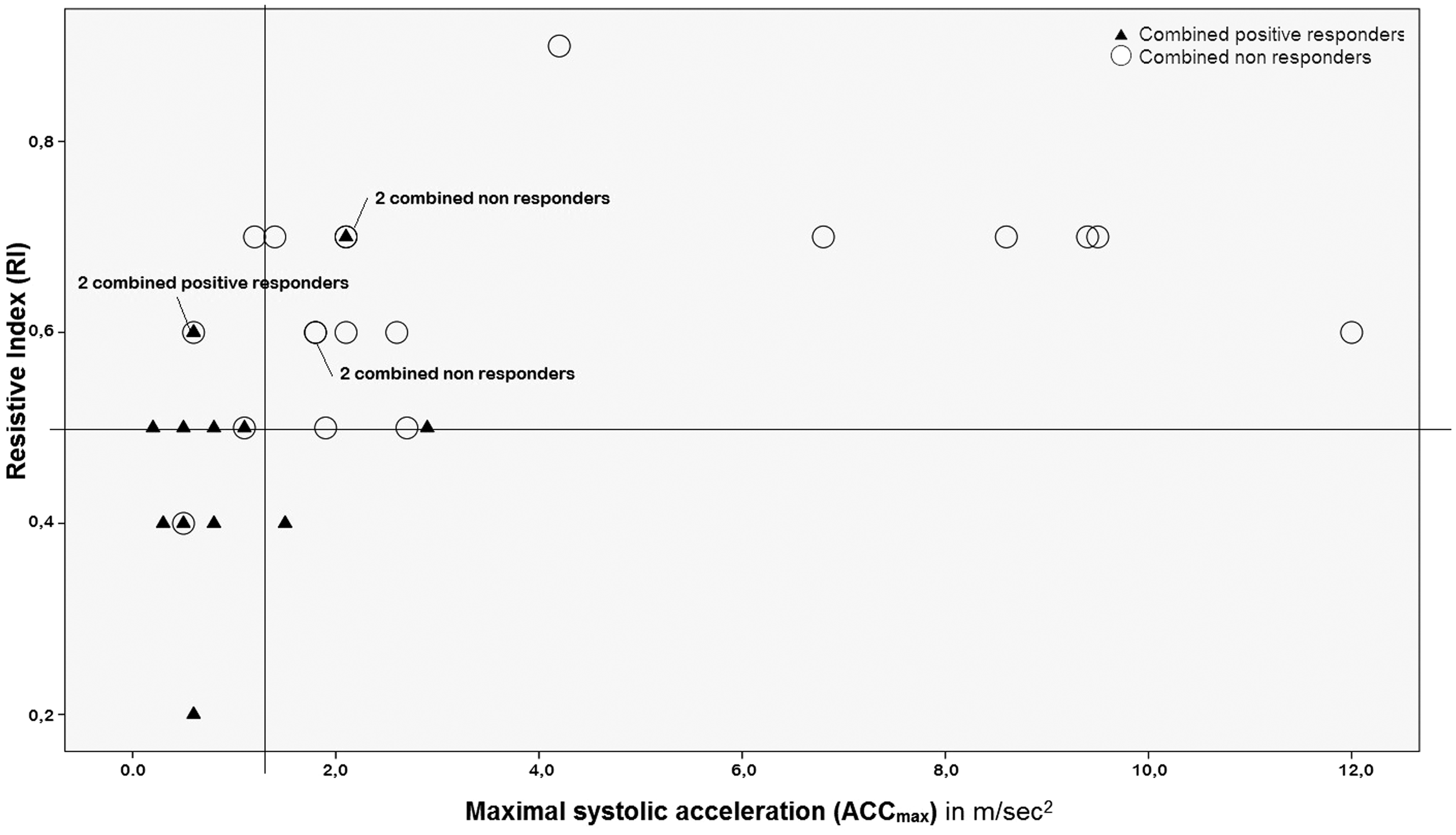
Discussion
Theoretically, renal revascularization might improve renal function and blood pressure control in patients with RAS. However, technically successful renal artery revascularization does not guarantee positive responses in terms of blood pressure regulation, preservation of renal function and reduction of cardiovascular events. Recent clinical trials9–11 showed a limited role for renal revascularization. As a result of criticism5,12,13 concerning the design of these trials and various observational studies14–16 showing beneficial outcome of renal revascularization compared to medical treatment in selected patients, one can postulate that there could be a subgroup of patients with a symptomatic RAS who will benefit from revascularization. The aim of this study is to identify parameters by intrarenal Doppler ultrasonography that is predictive for a positive response from revascularization.
The intrarenal Doppler ultrasonography is not only a tool to diagnose RAS,24–26,36–39 but prior research has shown its usefulness in predicting patients to be excluded from revascularization.29–31,40 To date, no valid and reliable selection methods are available to select patients who will have a positive response from renal revascularization. In our study, we postulate a prediction model (RI ≤ 0.5 and ACCmax ≤ 1.3 m/s2) that enables selection of patients who have the potential to benefits from renal revascularization. For our prediction model, we would expect a sensitivity of 69% and a specificity of 89% for improvement in renal function and/or blood pressure when applied to new patients based on double-cross-validation computation. The prediction model is a new objective instrument which has a contributing role in making a decision in the therapy of RAS. We prioritized the selection of patients who have a very high chance to have a beneficial response after renal revascularization, which limited the sensitivity of our model.
Schwerk et al. 36 introduced the RI as an indirect parameter for diagnosis and grading RAS. But more important is the predictive value of RI. According to Radermacher et al.,30,41 high RI (≥0.8) is a predictor for a response without improvement in renal function, blood pressure or kidney survival after intervention for RAS. A retrospective study showed patients with RAS who underwent percutaneous intervention with RI < 0.8 had a significant better eGFR response than patients with RI ≥ 0.8. 29 Santos et al. 31 found a high RI (≥0.80) as the most powerful predictor for no improvement in blood pressure outcome (OR 99.6). Voiculescu et al. 40 suggested an RI ≥ 0.55 and negative rennin ratio for predicting poor outcome concerning blood pressure response for unilateral RAS with a sensitivity of 88% and specificity of 67%. To date, studies only exclude patients for revascularization; e.g., patients with a high RI. In our study, we observed a significant association between beneficial response and a low RI. A similar result was found in the study of Radermacher et al. 30 We obtained the Doppler signals from interlobar arteries, and only Voiculescu et al. 40 measured the RI at the same position. Investigators in the other studies29–31,36,41 measured the RI from segmental arteries. So measurements from the interlobar artery could be an explanation why Voiculescu et al. 40 and our study had a lower RI cut-off value than the other studies.
Bardelli et al. 24 found the best ACCmax cut off at 4.0 m/s2 for diagnosing RAS with a sensitivity of 94% and negative predictive value (NPV) of 97%. Johansson et al. 26 used an acceleration of the blood flow <2.3 m/s2 as a criterion for RAS with a sensitivity of 83% and NPV of 96%. And Saeed et al. 25 established the best ACCmax cut off at 3.80 m/s2 with a sensitivity of 85% and NPV of 90% to diagnose RAS. To our knowledge, no study published an association between ACCmax and renal revascularization outcome. In our research, a low ACCmax correlates with a positive response in renal function and/or blood pressure after revascularization. The combined positive responders had a mean ACCmax of 1.0 m/s2. The morphology of the Doppler spectrum waveform may result in biasing factors on Doppler measures. It is important to note that the ACCmax occurs at the inflection point where the upstroke changes from concave up to concave down. It is equal to the slope of the tangent line on the curve at the inflection point. This results in less biasing factors caused by morphology of the Doppler spectrum waveform. 24
Due to multiple leading randomized controlled trials,9–11 there are still only a few renal revascularizations performed nowadays. It is important to minimize the number of unnecessary interventions, so the selection criteria must be very strict. Consequently, a minimal expected specificity of 80% was required to calculate the cut-off points of our prediction model. These cut-off points were calculated based on a single-level leave-one-out cross-validatory assessment across a range of potential cut-points. Because the statistical analysis for calculating the cut-off points involves an evaluation across all patients and our total sample size is small, some care must be applied when comparing the observed patient data with the thus chosen cut-off points. This would lead to a biased assessment and statement of predictive ability on future patients. To avoid this problem, the entire classification procedure was repeated using a double-cross-validatory procedure, as described in Mertens et al. 35 See also Figure 5, which shows the raw patient data superimposed on the optimized grid of cut-off points chosen by the single-cross-validation approach. In this figure, there were two patients who undergo revascularization without a combined positive response. If we look at these patients, they did have a decrease of 8% and 18% in MAP; but in our study, they were both MAP non-responders (see “Definition of responses to intervention” section). Additionally, they had respectively a normal and a slightly reduced eGFR at baseline.
De Leeuw et al. 13 described that the selection of patients is not optimal in angioplasty trials, such as in the ASTRAL trial. 9 The poor outcome from angioplasty is explicable by the pathophysiological principles. Generally, patients with already irreversible renal damage from RAS, so with less viable kidney tissue left, were included in the trial. Consequently, these patients have poor chances of beneficial response after intervention. 13 Santos et al. 31 suggested the poor outcome of renal artery revascularization might be explainable with the increased vascular resistance in the renal parenchyma due to glomerulosclerosis from longstanding hypertension. Ikee et al. 28 concluded an increase of RI is associated with renal histopathologic characteristics, particularly arteriolosclerosis. In our study, the non-responders had higher mean RI (0.63) compared to the positive responders (0.48). So there are indications that it is possible to select patients who have potential to improve after revascularization by using the intrarenal Doppler ultrasound. Furthermore, intrarenal Doppler ultrasonography is low cost, widely available, a non-invasive measurement and suitable for patients who cannot undergo angiography. In addition, the Doppler ultrasonography equipment is strongly improved in resolution in course of time. Consequently, the intrarenal RI and ACCmax are now well reproducible and very reliable in contrast to the past.
Limitations
In our study, all patients were treated in the same hospital. Consequently, percutaneous transluminal angioplasty interventions without a stent, percutaneous transluminal angioplasty interventions with a stent and open surgery revascularization were done by a small group of specialists. Although we found interesting findings in this study, there are several limitations. Due to the retrospective design of the study, multiple patients with renal artery revascularization were excluded from the analysis based on missing clinical data. In part, this relates to the absence of the Doppler parameters RI and ACCmax in a proportion of patients, as these parameters were not included in the routine work up during the entire study period. A sample selection-bias might have occurred through the inclusion and exclusion criteria of this study, e.g., all technically unsuccessful interventions (5 of the 104 patients) and patients with missing essential clinical data were excluded. However, we assume that the included patients do represent the total cohort of patients, as missing data were aselectively distributed. In additional, we had a small cohort of mixed composition including FMD and re-stenosis. Re-stenosis is generally known as a complication after revascularization and should therefore be included in the study population.
Conclusion
Technically successful renal artery revascularization does not guarantee positive responses in terms of blood pressure regulation and preservation of renal function. We postulate that our prediction model (RI ≤ 0.5 and ACCmax ≤ 1.3 m/s2), based on intrarenal Doppler ultrasonography, is a non-invasive tool to select RAS patients who have the potential to benefit from renal revascularization. This prediction model might be promising although it should be evaluated in a larger prospective study population to ensure its validity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.