
Abstract
Background
The aim of the present study was to investigate the role of inflammatory markers to predict amputation following embolectomy in acute arterial occlusion.
Methods
A total of 123 patients operated for arterial thromboembolectomy due to acute embolism were included in the study. The patients without an extremity amputation following thromboembolectomy were classified as Group 1 (n = 91) and the rest were classified as Group 2 (n = 32). These groups were compared in terms of clinical and demographic characteristics, C-reactive protein, complete blood count parameters, neutrophil-lymphocyte ratio, platelet-lymphocyte ratio and red cell distribution width.
Results
The average age was 68.0 ± 11.7 years. The most common thromboembolism localization was femoral artery. When preoperative mean C-reactive protein (p = 0.0001), mean platelet volume (p = 0.0001), platelet-lymphocyte ratio (p = 0.0001), neutrophil-lymphocyte ratio (p = 0.0001) and red cell distribution width (p = 0.0001) were compared, a statistically significant difference was observed between groups. In univariate and multivariate regression analysis, higher levels of preoperative C-reactive protein (p = 0.009) and mean platelet volume (p = 0.04) were detected as independent risk factors of early extremity amputation.
Conclusion
We observed that preoperative mean platelet volume and C-reactive protein were predictors of amputation after thromboembolectomy in acute arterial occlusion.
Introduction
Acute arterial occlusion is a clinical situation caused by embolic or thrombotic occlusion of arteries. Morbidity and mortality associated with acute arterial occlusion is high despite advances in surgical techniques and postoperative care in intensive care units. 1 On the other hand, limb amputation is an important complication of this clinical condition. Therefore, early diagnosis and treatment of acute arterial occlusion is associated with better clinical outcomes. 2 Thrombosis of atherosclerotic plaque is more commonly observed in elderly patients with acute arterial occlusion; in young people, non-atherosclerotic thrombosis and embolism are more frequently observed. 1
Inflammation is one of the key drivers of atherosclerotic plaque development and the interplay between inflammation and lipids constitutes the hallmark of atherosclerotic disease. Inflammatory mediators have been shown to be associated with atherosclerosis, thrombus formation and plaque rupture. 3
Neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) are recently defined inflammatory markers obtained from complete blood count (CBC) parameters, have been shown to be associated with prognosis in acute coronary syndromes. 4 Also the CBC parameters, mean platelet volume (MPV), red blood cell distribution width (RDW) and C-reactive protein (CRP) have been shown to have prognostic value in various vascular diseases.5–8
The main objective of treatment in acute arterial occlusion is to maintain the vitality of the limb and survival of the patient. 9 The first treatment option in acute arterial occlusion is surgical embolectomy. Acute arterial occlusion is associated with amputation rates of 10-30% and the rate of mortality was reported to be 10 to 25% in the early postoperative period (30 days).10,11
In this study, we investigated the association of CBC parameters (MPV, PLR, NLR and RDW) and CRP as predictors of amputation after thromboembolectomy in acute arterial occlusion.
Material and methods
The records of 123 patients who were admitted to emergency unit between January 2010 and May 2015 due to complaints of pain, pulselesness, cyanosis, loss of temperature, pallor, paresthesia and paralysis who were diagnosed as acute arterial occlusion and operated for thromboembolectomy in our clinic were investigated retrospectively. The number of female patients was 48 (39%) and the average age was 68.0 ± 11.7 years (median 69 years, ranging 38–88 years). The patients in whom no extremity amputation was performed after the surgery were classified as Group 1 (n = 91) and those in whom amputation was performed in the early post-operative period (first one month) were classified as Group 2 (n = 32).
Patients with chronic renal failure under hemodialysis treatment, patients who had hematologic proliferative diseases, presence of cancer, hepatic failure, those who had experienced myocardial infarction in the final month, those with a history of cerebrovascular accident in the final year, those who had experienced coronary artery bypass grafting surgery in the final three months, those who had a vascular percutaneous intervention or surgery, those in which sepsis or bacteriemia had developed within the first three days, those who had 38℃ or greater fever or a known active infection, the patients who already developed muscle necrosis, rigidity and other irreversible findings on admission who were directly amputated were excluded from the study.
The patients were initially examined by arterial color Doppler ultrasonography by a radiologist. Distal arterial bed was attempted to be imaged by performing urgent peripheral angiography, if possible, especially in patients for whom acute artery occlusion was suspected to be developed on the atherosclerotic background or who were already known to have peripheral artery disease. Urgent arterial thromboembolectomy was performed in patients for which arterial occlusion was verified. Informed consent was taken from all patients and basic blood examinations (hemogram, whole blood biochemical analysis, CRP) were studied prior to surgery. Telecardiography and electrocardiography were applied. Abdominal ultrasonography and echocardiography were performed in all patients following thromboembolectomy to identify the origin of the acute artery occlusion.
Arterial hypertension was considered in patients with repeated (at least three times) measurement of blood pressure above 140 mmHg systolic and 90 mmHg diastolic or active use of antihypertensive medication. Diabetes mellitus was defined as fasting plasma glucose levels above 126 mg/dl in at least two different measurements or active use of anti-diabetic drugs. Smoking was defined as current smoking or ex-smokers forgave smoking in past six months. Hyperlipidemia was accepted as total cholesterol >220 mg/dl and LDL-cholesterol >130 mg/dl or use of antihyperlipidemic drugs.
All of the operations were done under slight sedation and local anesthesia. Brachial arterial thromboembolectomy was applied from the antecubital region through transverse incision and femoral arterial thromboembolectomy was applied from the groin region through a longitudinal incision. Before arterial clamping, systemic 100 IU/kg intravenous heparin was administrated. Embolectomy was performed from distal and proximal segments by using Fogarty catheter (3–6 F) following arteriotomy. Embolectomy was terminated in cases in which thrombus or embolism material was suggested to be completely cleared (No further thrombus or embolus material obtained) and anterograde and retrograde flow was suggested to be sufficient. Afterwards, the artery was washed with heparinized solution distally to arteriotomy. While arteriotomy was closed primarily in patients with good vessel structure, it was closed with a saphenous patch in patients with poor vessel quality. In patients for whom embolic material was suspected for acute arterial occlusion, heparin infusion was applied in 18 IU/kg/day for three days in a fashion that activated clotting time (ACT) remained between 200 and 250 s. Anticoagulant treatment was initiated in the on the day of operation in these patients. When the prothrombin time of the patients was 1.5 fold of the normal and their international normalization ratio (INR) values reached to 2 and higher, heparin was stopped and oral anticoagulant treatment was continued. In patients for whom arterial occlusion occurred with thrombus material, heparin infusion was applied in 18 IU/kg/day again in a fashion that ACT remained between 200 and 250 s in the first 24 h; 300 mg/day acetylsalicylic acid and clopidogrel in 75 mg/day dose was continued from the first day. Moreover, iloprost infusion was administrated for three days to these patients. Hourly urinary output, electrolyte imbalance and blood gas analysis were closely monitored in all patients to early recognize systemic complications due to reperfusion in the postoperative period and for treatment follow-up.
Fasciotomy was performed by an orthopedist in patients with compartment syndrome due to the reperfusion injury. Amputation was performed by a common decision with the Department of Orthopedics in patients with ongoing ischemia for which demarcation line was developed following re-embolectomy, bypass and/or fasciotomy. Mortality was identified as the deaths with identified causes within the first post-operative month.
This study was established in accordance with Helsinki Declaration and by taking the approval of the Ethical Committee of Clinical Researches of the Medical Faculty of Kocaeli University.
Statistical analysis
Statistical analysis was performed using the SPSS software version 12.0 (SPSS Inc, Chicago, IL, USA). Among the data measured, those showing normal distribution were expressed as mean ± standard deviation; those not showing normal distribution were expressed as median (minimum–maximum). The data obtained by counting were given as percentages (%). Among the data measured, the normality of distribution was evaluated by histogram or Kolmogorov–Smirnov test, the homogeneity of distribution was evaluated by ‘Levene’s test for equality of variance’. Among the data measured, the difference between the groups was evaluated by ‘Student’s t test’ in normal and homogenous distribution and by ‘Mann–Whitney U test’ in distribution which is not normal and homogenous. Among the data obtained by counting, the differences between the groups were evaluated by parametric or non-parametric Pearson Chi-Square test or Fisher’s Exact test according to the distribution being parametric or not. The effects of the risk factors suggested to be influential on the early mortality and morbidity were studies through the univariate logistic regression analysis. The multiple effects of the risk factors which are influential or which are suggested to be influential in predicting the mortality and the morbidity as a result of the univariate statistical analysis were studied through the retrospective selective multivariate logistic regression analysis. The odds ratio, the 95%-confidence interval and the significant level for each of the risk factors were found. The sensitivity and the specificity of risk factors in predicting extremity amputation via receiver operating curve (ROC) were computed and results were found as statistically significant for p < 0.05.
Results
Demographic and clinical properties of the patients.
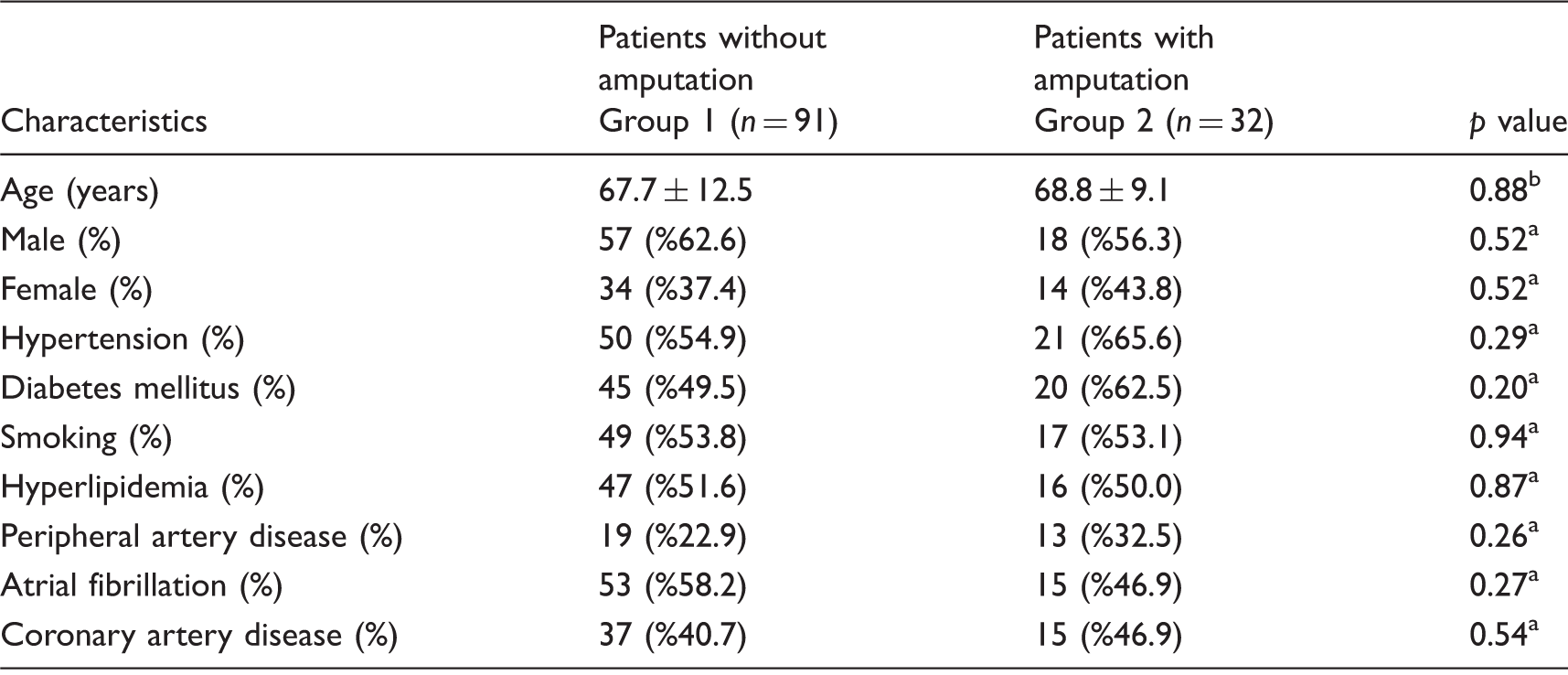
Pearson Chi-Square test or Fisher’s Exact test.
Mann–Whitney U test.
The reason for admittance to hospital were pain in 114 patients (92.7%), loss of temperature in 108 patients (87.8%), pallor in 86 patients (69.9%), cyanosis in 54 patients (43.9%), paresthesia in 68 patients (55.2%) and paralysis in 26 patients (21.1%). Among the cases, 77 of them (62.6%) were admitted to hospital in the first 12 h and 46 of them (37.4%) were admitted exceeding 12 h following the initial complaint. The length of time for the patients from the beginning of initial symptoms to their admission to hospital were 11.2 ± 3.0 (median: 10, range: 6–19) h in Group 1 and 12.4 ± 4.3(median: 11, range: 6–23) hours in Group 2. There was no statistically significant difference between the groups (p = 0.18).
The distribution of location of thrombus or embolus material.
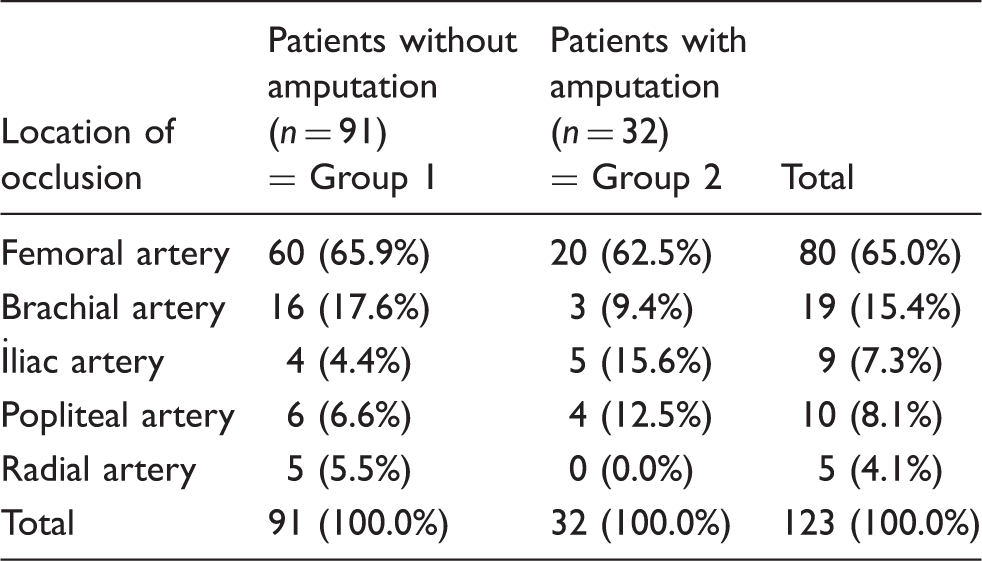
The locations of thromboembolectomy were right femoral artery in 55 (44.7%), left femoral artery in 43 (35%), left popliteal artery in 1 (0.8%), right brachial artery in 10 (8.1%) and left brachial artery in 14 (11.4%) patients.
Preoperative blood results and haematological parameters of patients.
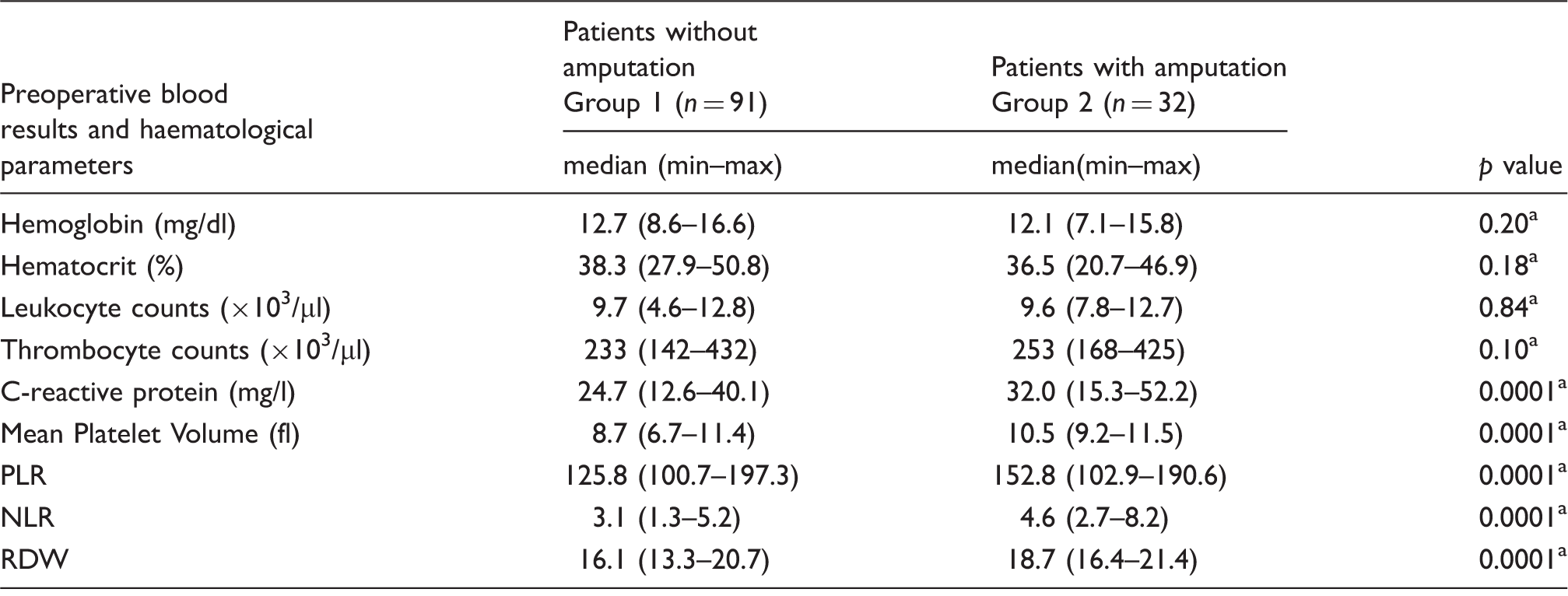
PLR: platelet–lymphocyte ratio; NLR: neutrophil–lymphocyte ratio; RDW: red blood cell distribution width.
Mann–Whitney U test.
The number of patients who were applied thromboembolectomy but taken to repeat thromboembolectomy for ongoing ischemia were 5 (5.5%) in Group 1 and 9 (28.1%) in Group 2. The difference was statistically significant between the groups (p = 0.001).
Amputation was done above the knee in 9 patients (28.1%), below the knee in 20 patients (62.5%) and below the elbow in 3 patients (9.4%) in Group 2. The average length of stay in the intensive care unit was 2.4 ± 0.6 (median: 2, range: 2–4) days in Group 1 and 3.7 ± 1.4 (median: 3.5, range: 2–7) days in Group 2. There was a statistically highly significant difference between the groups (p = 0.0001). The average length of stay in the hospital for the patients who survived were 7.0 ± 1.7 (median: 7, range: 5–12) days in Group 1 and 14.9 ± 2.9 (median: 14, range: 10–21) days in Group 2 which showed a statistically highly significant difference between the groups (p = 0.0001).
Demographic and clinical properties of patients with mortality in both groups.

CAD: coronary artery disease; PAD: peripheral artery disease; DM: diabetes mellitus; AF: atrial fibrillation, HT: hypertension.
Univariate and multivariate regression analysis for risk factors of patients who were applied amputation or not.
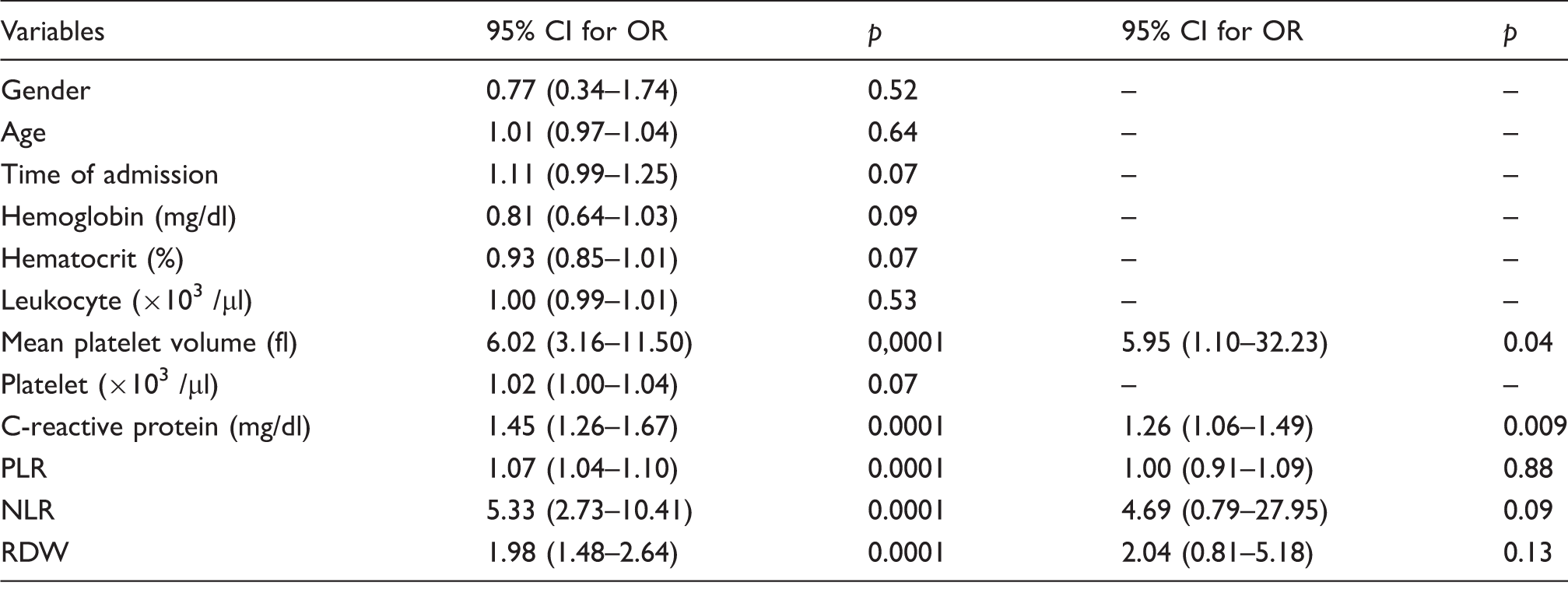
PLR: Platelet to lymphocyte ratio; NLR: Neutrophil to lymphocyte ratio; RDW: Red blood cell distribution width.
The cut-off levels for CRP and MPV which were detected as predictors of extremity amputation with multivariate regression analysis were sought by ROC curve analysis to predict the probability of amputation. These levels, which were automatically calculated by SPSS statistical software by ROC curve analysis, were 12.2 mg/dl for CRP and 9.6 fl for MPV. The ROC curve analysis was shown in Figure 1. The area under curve (AUC) values for CRP and MPV were 0.98 and 0.91, respectively (%95 GA = 0.95–1.00, p = 0.0001 for CRP and %95 GA = 0.86–0.96, p = 0.0001 for MPV). When the cut-off level for CRP was used as 12.2 mg/dl, it was found to predict extremity amputation with 97% sensitivity and 95% specificity. When the cut-off level for MPV was used as 9.6 fl, it was found to predict extremity amputation with 94% sensitivity and 86% specificity.
ROC curve analysis for levels of CRP and MPV to predict early term extremity amputation following thromboembolectomy for acute arterial occlusion.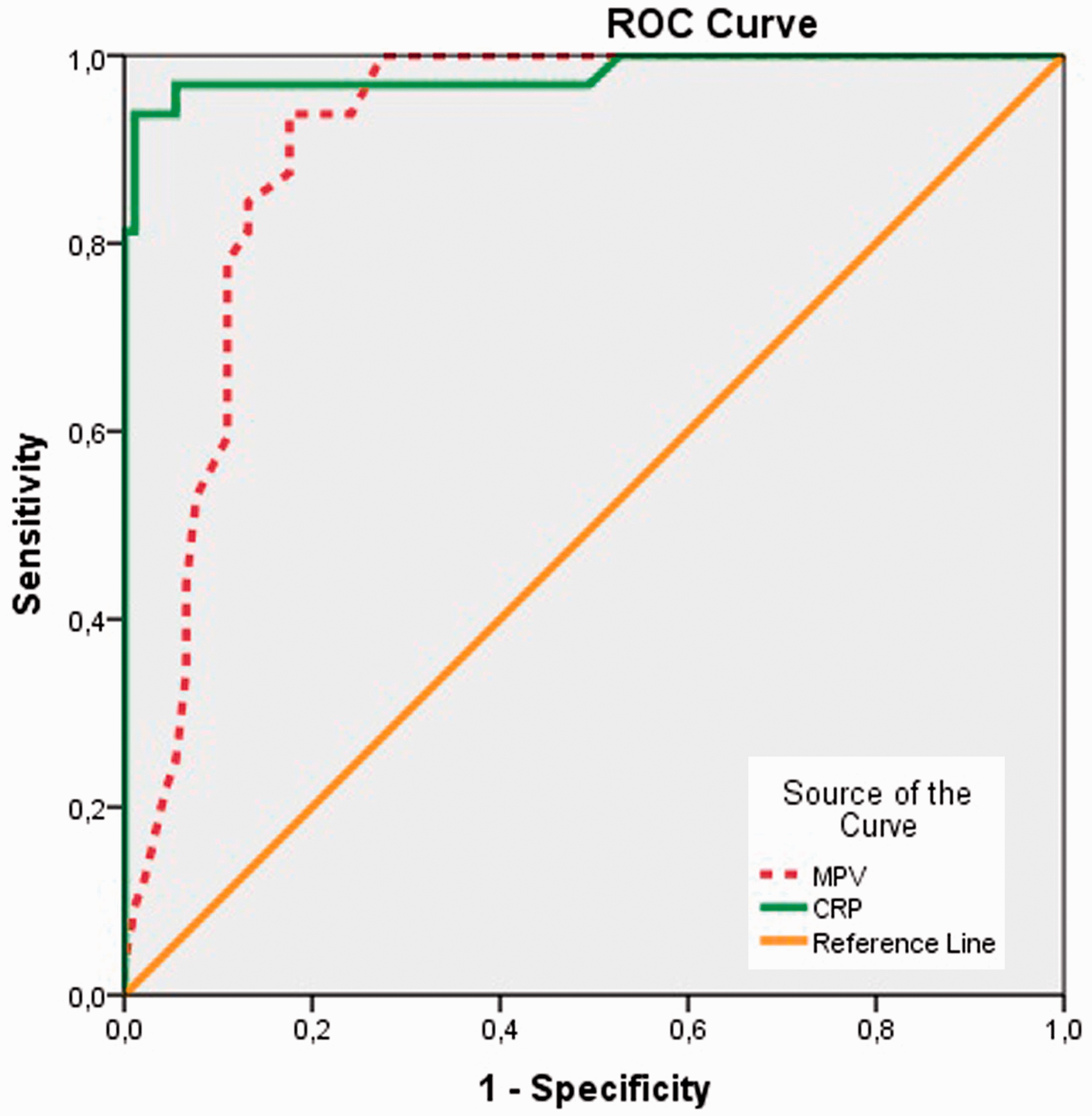
Discussion
The association of inflammatory biomarkers with acute arterial occlusion and postoperative early amputation (first month) has not been fully elucidated in the literature. In this study, we observed significant elevation of preoperative CRP, MPV, NLR, PLR and RDW values in patients who underwent early amputation after arterial embolectomy.
Acute peripheral arterial occlusion is the most common cause of emergent vascular surgery with 16%–33% of all acute limb ischemia patients. 12 It can be associated with thrombosis of pre-existing atherosclerotic plaques or embolism of thrombus from left heart chambers. 13 In our study, the most common etiology was thrombosis in 71.5% of cases and embolism in 28.5% of cases.
Acute arterial embolism is associated with rapid ischemic injury without sufficient collateral circulation; however, in acute arterial thrombosis, ischemic injury occurs gradually due to chronic nature of atherosclerosis and presence of collateral arterial circulation. Therefore, the symptoms gradually increase in thrombosis but occur more rapidly in embolism. 14
Atherosclerosis is closely associated with chronic inflammation, and the risk factors contribute to development of inflammatory process. Inflammation also plays an important role in formation of plaque rupture and thrombosis.3,15
Endothelial dysfunction is accompanied with fibrous plaque formation caused by proliferation of muscle cells in atherosclerotic plaques. This plaque contains leukocyte subtypes (neutrophils and monocytes) and which are activated by cytokines such as interleukin 1 and tumor necrosis factor. Activated leucocytes disrupt microcirculation and are associated with necrotic tissue enlargement. 16 Especially in the plaque rupture stage of atherosclerosis neutrophils, lymphocytes and platelets are involved actively. 17
CRP is an acute phase reactant which is an indicator of systemic inflammatory response. Several epidemiological studies of CRP are closely associated with atherosclerosis and coronary artery disease. 18 CRP is involved in atherosclerotic plaques and contributes to atherogenesis and procoagulant state. 19 Chang et al. 20 have observed that CRP values were elevated in patients with ischemic stroke. It has been observed that vascular inflammation is associated with increased levels of CRP in unstable angina. CRP is associated with morbidity and mortality in atherosclerosis and vascular disease. 21
Vrsalović et al. 22 have observed that increased levels of CRP and renal failure was associated with outcomes in peripheral artery disease. In another trial, Bleda et al. 23 have observed that CRP levels were associated with prognosis in patients who underwent endovascular treatment. Lin et al. 24 have observed that CRP was prognostic in diabetic patients with peripheral arterial disease and infected foot ulcers treated with percutaneous transluminal angioplasty. Concordant with the findings in the literature, we have observed that CRP levels were indepently associated with amputation rates in our trial.
Platelets play an important role in the pathogenesis of atherosclerotic complications by contributing to thrombus formation. 25 Thrombocytosis is commonly associated with a peripheral arterial disease and has been widely reported as an adverse prognostic marker. 26 MPV is a parameter that is routinely measured in complete blood count devices which is an important marker of thrombocyte activation. 27 MPV has been studied as a simple inflammatory marker in several diseases. Some studies have reported that MPV increases in myocardial infarction and cerebrovascular disease.28,29 Some studies have suggested that MPV levels increase as a result of peripheral arterial disease.30,31 In our study, we observed that MPV levels were closely associated with amputation.
Currently, NLR and PLR parameters obtained from CBC have been investigated in several diseases as a marker of inflammation. Due to close association of atherosclerosis with inflammation, these markers have also been investigated in vascular disease.25,32 Also, NLR has been shown to be a prognostic marker in non-cardiac disorders. 33 Kaya et al. 34 observed that NLR was associated with long-term cardiovascular events in four years follow-up. NLR has been found to be an independent predictor of short-term mortality in patients with acute coronary disease. 35 Spark et al. 36 have observed that NLR was associated with mortality in critical limb ischemia. In another study, NLR was detected as a predictor of amputation after embolectomy in acute limb ischemia. 37 Our results were concordant with the previous findings in the literature.
PLR is closely associated with aggregation and inflammation pathways. PLR predicts atherosclerotic burden better than platelet and lymphocyte counts. 38 Although preliminary data have shown that the PLR is associated with major adverse cardiovascular outcomes and some cancers, there are not enough data, especially in cardiovascular disease.39–41 Gary et al. 25 have observed that increased PLR ratio was predictor of critical limb ischemia in peripheral arterial occlusive disease patients. In our study, we have observed that preoperatively increased PLR was associated early amputation rates after embolectomy. According to best of our knowledge, this is the first study with these findings.
RDW, which is the variability of size of erythrocytes, can be easily measured from routine CBC. Inflammation may disrupt erythrocyte membranes, can change erythrocyte maturation and lead to increases in RDW levels. 42 Previous studies have reported RDW to be an independent predictor of mortality in community-dwelling adults and patients with cardiovascular disease.7,43 Ye et al. 44 have observed that RDW levels were associated with outcome in patients with peripheral arterial disease. Concordant with the findings in the literature in our study, we have observed that preoperatively RDW levels were associated early amputation rates after embolectomy. In addition to the inflammation, the presence of neurologic findings (especially paresthesia and paralysis) was an important predictor of amputation in our study.
In conclusion, we found in our study that, markers of inflammation such as CRP, MPV, RDW, NLR and PLR predict amputation in acute arterial thromboembolism. Futher studies with larger sample sizes may be needed to determine the presence and the role of inflammation in acute arterial occlusion.
Limitations
Our study is a retrospective study conducted in a single center with a small number of patients. Despite that we have found some parameters associated with mortality, we could not draw a causal relationship. Due to the retrospective design of the study, we could not screen the patients for the presence of hypercoagulable hereditary disorders.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.