
Abstract
Objective
This study was planned and implemented to evaluate the effect of socio-demographic characteristics and clinical findings on the quality of life of patients with chronic venous insufficiency.
Methods
The sample of this cross-sectional study consisted of 163 patients that presented with the diagnosis of chronic venous insufficiency to the cardiovascular surgery clinic of an education and research hospital in the west of Turkey. The data were collected during face-to-face interviews using a personal information form, clinical, etiology, anatomy, pathophysiology classification, venous insufficiency epidemiological and economic study-quality of life/symptoms scales and the Short Form-36. Descriptive statistics as well as univariate and multivariate analyses were used to analyze the data.
Results
The chronic venous insufficiency patients were found to have a low quality of life. Advanced age, higher body mass index, longer working times, being on regular medication, hypertension and presence of pigmentation according to the clinical, etiology, anatomy, pathophysiology classification were found to be associated with a reduced physical score in SF-36. Furthermore, longer weekly working hours and presence of pigmentation reduced the Venous Insufficiency Epidemiological and Economic Study-Quality of Life/Symptoms scores. Undertaking physical exercise at twice and more than twice a week increased the overall physical scores in SF-36.
Conclusions
The results of the study showed that the quality of life of chronic venous insufficiency patients are affected by not only physical characteristics, working hours and physical activity but also presence of edema and pigmentation.
Keywords
Introduction
Chronic venous insufficiency (CVI) is a medical condition characterized by the expansion and deformation of veins due to the increase in the pressure within the veins caused by the insufficiency of venous valves. 1 It is estimated that globally 83% of all adults have a chronic venous disorder and 9% have CVI caused by skin changes and healed or active venous ulcers. 2 Venous diseases are seen in 25–33% of women and 10–20% of men within the age range of 30 to 70 years. The annual incidence of the disease has been reported as 2.6% and 1.9% in women and men, respectively.3–5
Chronic venous insufficiency involves high costs in both diagnosis and treatment, and results in a reduced quality of life (QoL) and ability to work and socio-economic losses.1,4–6 It can be asymptomatic or present with severe symptoms including pain resulting from standing for a long time, burning, itchiness, tingling, swelling and night cramps. In chronic cases, skin changes and venous ulcers may be observed. In varicose veins, thrombophlebitis and secondary pulmonary embolism may develop.6–8 Recurrent and untreated ulceration increases treatment cost and the duration of hospital stay.1,9 These symptoms also lead to patients with CVI developing psychological problems. For example, patients with varicose veins may have concerns about the cosmetic appearance of their legs. Furthermore, complications such as ulceration and deep vein thrombosis can develop.10,11 Studies have shown that CVI has a negative effect on the QoL of patients in terms of both physical and social dimensions. It has been reported that the daily activities of these patients are inhibited mostly due to pain, itchiness, swelling and sleeping disorders as well as limitation of movement, anxiety, depression and social isolation.4,11–16
The QoL of patients with CVI can be improved by increasing their comfort and providing them with appropriate nursing care. In Turkey, there is only a limited number of studies evaluating the QoL of these patients; therefore, it is considered that the results of the present study will contribute to future studies and the improvement of patients’ individual health. This study was planned and implemented to evaluate the effect of socio-demographic variables and clinical findings on the QoL of patients with CVI.
Material and method
Research question
What is the effect of socio-demographic characteristics and clinical findings on the QoL of patients with CVI?
Study design
This study is based on a cross-sectional design.
Study population and sample
The population of the study consisted of patients that presented with the diagnosis of monitored CVI to the cardiovascular surgery clinic of an education and research hospital in the west of Turkey between 1 November 2014 and 31 January 2015. The sample size was calculated using the PASS program to perform one-way variance analysis on the scores obtained from the physical subscale of the Short Form-36 (SF-36) according to the clinical, etiology, anatomy, pathophysiology (CEAP) classification described by Kutlu et al. 17 The minimum sample size was calculated as 116 with a 5% deviation of 80% power and 95% confidence interval, α = 0.001 (Bonferroni’s correction applied); therefore, a total of 163 patients were included in the study. Although 207 patients with CVI diagnosis were admitted to outpatient clinic, only 163 met the inclusion criteria of having complete data for the three months.
Inclusion criteria
The criteria for inclusion in the study were voluntary participation in the study, being over 18 years of age, being diagnosed with CVI according to the results of physical examination and tests, being open to communication and cooperation, having no sight or hearing problems, being conscious and able to answer questions and having no disease that could affect the decision-making ability (such as dementia or psychological disorders).
Data collection tools
The following forms were completed for each patient.
Personal information form CEAP classification Venous insufficiency epidemiological and economic study-quality of life/symptoms Scales (VEINES-QOL/Sym) Short Form 36 (SF-36)
The dependent variables of this study were mean VEINES-QOL/Sym scores and physical and mental scores of SF-36. The independent variables consisted of demographic characteristics such as age, gender, BMI, educational level, income, total working time, comorbidity, physical activity, diagnose time etc.
Data collection
The study was approved by the Scientific Ethics Committee (Reference number 24.09.2014/20478486-325). The hospital provided written permission for the implementation of the study. All the volunteer patients gave their written and verbal informed consent. The data were collected from the patients using the above-mentioned tools during face-to-face interviews between October 2014 and January 2015. Each interview lasted approximately 20–25 minutes.
Statistical analysis
The data were analyzed using SPSS 15.0 (SPSS, Chicago, IL, USA). The Kolmogorov Smirnov test was performed to investigate whether the data were normally distributed. The descriptive statistics mean ± standard deviation of the continuous variables was calculated and those of the categorical data were presented in numbers and percentages.
The independent variables were shown demographic characteristics such as age (continuous variable: years), gender (dichotomous variables: male and female), BMI (continuous variable: kg/m2), educational level (dichotomous variables: high school or lower and college or higher), income (dichotomous variable: average or lower and above average), total working time (continuous variable: years), comorbidities (ordinal variables: hypertension, diabetes mellitus, endocrine disorders), physical activity (ordinal variables: never, less than once a week, once a week, twice and four a week, five or more times a week), diagnose time (continuous variable: years) etc.
Univariate and multivariate ordinal logistic regression analyses were performed on the analytical data. In the multivariate analysis, the model was created using the variables that had been found significant in the univariate analysis. The findings were expressed as odds ratio (95% confidence interval). All analyses were performed with Stata 14.0 and used enter method.
Results
Patient demographics.

BMI: body mass index; SD: standard deviation.
Clinical data on the patients.

CEAP: Clinical, etiologic, anatomic, pathophysiologic; PCS: physical component summary; MCS: mental component summary; VEINES-QOL/Sym: venous insufficiency epidemiological and economic study-quality of life/symptoms scales (VEINES-QOL/Sym); SD: Standard deviation.
The results of the univariate analysis on quality of life (QoL) dimensions in relation to socio-demographic characteristics.
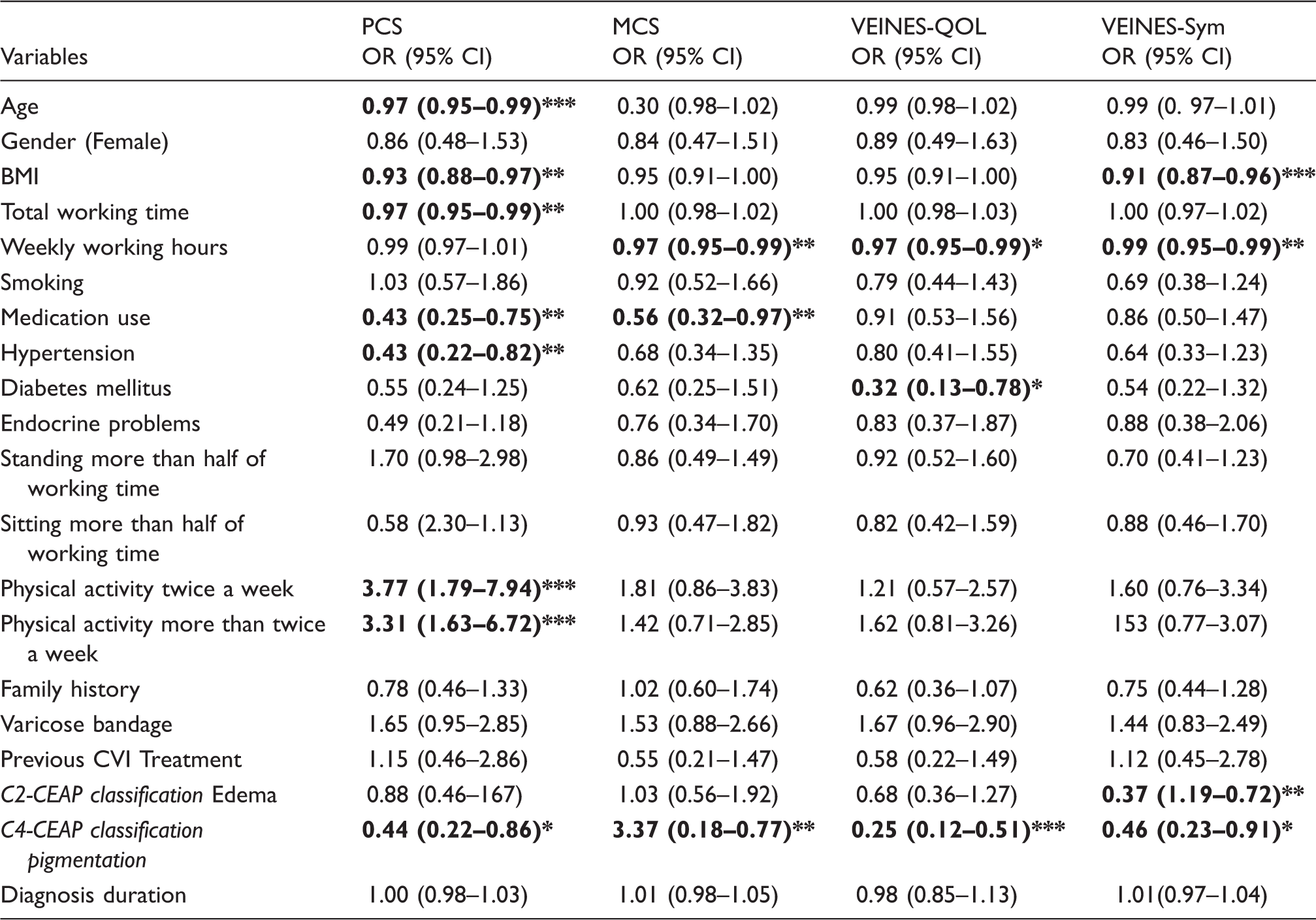
OR (95%CI) = Odds Ratio (95% confidence interval); CEAP: clinical, Etiologic, anatomic, pathophysiologic; PCS: physical component summary; MCS: mental component summary; VEINES-QOL/Sym: venous insufficiency epidemiological and economic study-quality of life/symptoms scales.
The results of the multivariate analyses on the quality of life (QoL) dimensions in relation to socio-demographic characteristics.

OR (95% CI) = Odds Ratio (95% confidence interval); CEAP: clinical, etiologic, anatomic, pathophysiologic; PCS: physical component summary; MCS: mental component summary; VEINES-QOL/Sym: venous insufficiency epidemiological and economic study-quality of life/symptoms scales.
p < 0.05, **p < 0.01, ***p < 0.001.
According to the analysis of the basic socio-demographic and prognostic characteristics of the patients, the QoL PCS score was found to be negatively associated with; increased age (0.97 [0.95–0.99]), higher BMI (0.93 [0.88–0.97]), longer working years (0.97 [0.95–0.99]), using on regular medication (0.43 [0.25–0.75]), presence of hypertension (0.43 [0.22–0.82]) and presence of pigmentation according to the CEAP classification (0.44 [0.22–0.86]). There was a positive significant relation between the PCS scores and undertaking moderate activity for twice a week (3.77 [1.79–7.94]) and for more than twice a week (3.31 [1.63–6.72]). In other words, the PCS scores rose with the increase in the number of activity level of the patients (Table 3).
The MCS score was found to be negatively affected by longer weekly working hours (0.97 [0.95–0.99]), using regular medication (0.56 [0.32–0.97]) and presence of pigmentation according to the CEAP classification (3.37 [0.18–0.77]). A negative relationship was found between VEINES-QOL and longer weekly working hours (0.97 [0.95–0.99]), presence of diabetes (0.32 [0.13–0.78]) and the presence of pigmentation (0.25 [0.12–0.51]). VEINES-Sym was found to be negatively associated with a higher BMI (0.91 [0.87–0.96]), longer weekly working hours (0.99 [0.95–0.99]) and presence of edema (0.37 [1.19–0.72]) and pigmentation (0.46 [0.23–0.91]).
According to the multivariate model of the socio-demographic and prognostic characteristics of the patients in the study, a higher BMI was found to be negatively associated with the QoL PCS score (0.93 [0.88–0.99]) and the VEINES-Sym score (0.93 [0.88–0.98]). Furthermore, longer weekly working hours had a negative relationship with the QoL MCS score (0.97 [0.95–0.99]), VEINES-QOL scores (0.98 [0.96–0.99]) and the VEINES-Sym score (0.97 [0.95–0.99]). A similar negative association was observed between presence of edema according to the CEAP classification and VEINES-Sym score (0.48 [0.24–0.94]). Another negative impact was that of the presence of pigmentation on VEINES-QOL scores (0.29 [0.14–0.59]). On the other hand, undertaking physical activity once a week (2.80 [1.24–6.33]) or more (2.62 [1.16–5.89]) had a positive effect on the PCS scores (Table 4).
Discussion
The present study evaluated the QoL of patients with CVI. The patients were found to score low in SF-36 and VEINES-QOL/Sym and have a poor QoL.
In the study, the older patients had a lower PCS score and poorer QoL. Similarly, other studies have demonstrated that QoL decreases with increased age.22,23 This is attributed to the negative impact of CVI often being accompanied by other diseases in older patients.
The majority of the patients participating in the study (70.6%) were female and there were 2.4 times women than men. It has been reported that venous system diseases affect approximately 25%–33% female and 10%–20% male in Turkey. 9 Several studies have reported that being female constitutes a risk for CVI14,15,17,24,25 and the results of the present study support this finding.
The results of the present study demonstrated that gender did not have a significant effect on the QoL of patients with CVI. Kurz et al. conducted a study with patients with varicose veins and edema and reported that the PCS and MCS scores were higher in men than in women. 26 Similarly, Kaplan et al. 13 found higher PCS and MCS scores in men compared to that in women. However, similar to our study, Çeviker et al. 27 did not find a significant difference between female and male patients with CVI in terms of their QoL.
The mean BMI of the patients was calculated as 27.4 ± 5.58 kg/m2. Various studies have reported that obesity is a risk factor for CVI14,17,23 and a higher BMI also increases the level of CEAP classification.14,25 In addition, the reports show that BMI negatively affects QoL with obesity being among the independent indicators of a poor QoL. 14 In the present study, PCS and VEINES-QOL/Sym scores were found to be lower in patients with a high BMI. It is considered that being overweight increases the severity of the patients’ present symptoms and thus reduces their QoL scores.
In this study, a statistically significant association was found between the CEAP classification and PCS, MCS and -QoL/Sym scores of the patients. The patients’ QoL decreased with the increase in the level of the CEAP classification. As the severity of the disease increases, QoL worsens. Similarly, other studies have reported that a higher classification in CEAP goes parallel with lower QoL.13,14,17,26,28 As the severity of the disease according to the CEAP classification increases, the physical functioning of the patients is reduced, negatively affecting their work, social and economic lives. In addition, increased severity of CVI may result in changes in the skin, resulting in lower self-esteem and emotional reactions. We consider that the patients’ health is further affected by the changes in and effects on their lifestyles caused by the increased complaints such as pain edema and ulcers.
In the current study, more than half the patients (51.5%) reported a complaint of CVI in the family history. In the literature, genetic factors are considered to have a role in this disease.26,29–31 Kutlu et al. 17 reported that 47.8% of the patients had a family history of CVI, of which 34.9% were their parents. Çeviker et al. 27 found that 32.5% of the patients with CVI had a family history of the disease.
In the present study, the VEINES-Sym and VEINES-QOL scores of the patients were determined as 29.23 ±9.12 and 40.29 ± 8.46, respectively. In their study with 236 female and 23 male patients, Kurz et al. only found high VEINES-QOL/Sym mean scores in patients with new varicose veins whereas in patients with an active ulcer in addition to varicose veins, these scores were lower. 26 In another study conducted with 1531 patients living in Belgium, France, Italy and Canada, their mean scores were reported to be 47.4 ±6.4 for VEINES-QOL and 47.9 ± 6.7 for VEINES-Sym. 14 In another study, the mean VEINES-QOL/Sym score was calculated as 50.0 ±10.0. 17 The mean scores in both scales in our study were lower than reported in the literature, which indicates that our patients had a poorer QoL due to CVI.
For the present study, the mean SF-36 PCS and MCS scores were 38.37 ± 8.37 and 43.72 ± 9.07, respectively. Kaplan et al. 13 conducted a population-based study in San Diego with CVI patients and similarly reported a lower PCS than MCS. There are also other reports of PCS scores being lower than that of MCS.14,17,32 CVI affects all aspects of an individual’s life, thus reducing their QoL. The results of the present study support those from the literature.
The working long hours had a negative impact on SF-36 PCS scores. In addition, the SF-36 MCS and VEINES-QOL/Sym scores were found to be low in patients who worked for longer hours in a week and they had a poorer QoL. In the literature, long-term standing is considered to be a secondary risk factor.17,26 Similarly, Duque et al. 33 reported a higher percentage of CVI in nurses that sat for a long time or stood when working. Campbell et al. 34 emphasized that among all the leg positions, the upright position (standing) most increased the complaints related to varicose veins and recommended leg elevation and walking to reduce the development of varicose veins. This is in agreement with the results of our study, in which we found higher SF-36 PCS scores in patients who undertook physical activity once or more times a week.
In this study, the most frequent symptoms were reported to be pain, changes in skin and edema. Previous studies have shown that pain due to CVI negatively affects QoL.33,35 This is considered to result from functional insufficiencies and sleeping disorders caused by pain.
Limitations of the study
The sample of the study consisted of only the patients with a diagnosis of CVI that presented to the polyclinic and were undergoing monitoring. Therefore, the results are limited to this sample group and cannot be generalized to represent the whole population. There are also limitations collecting in a short time as three months of data, not using the control group, the majority of the sample to be women and not following to long-term observation in this study. Another limitation is participants with hypertension, diabetes and endocrine disorders were included to this study.
Conclusion
The results of the study demonstrated that patients with CVI have a low QoL. Advanced age, higher BMI, longer working hours, being on regular medication, hypertension, sitting continuously for long hours when working and presence of pigmentation according to the CEAP classification were found to be associated with a reduced SF-36 PCS score. Furthermore, a higher BMI, longer weekly working hours and presence of pigmentation decreased the VEINES-QOL/Sym scores. Undertaking physical exercise at least once a week increased the PCS scores. Healthy lifestyle behaviors increased the QoL of patients.
Based on the results of the current study, we recommend
informing people in the CVI risk group about the symptoms and findings of the disease and encouraging them to change their lifestyle informing patients with CVI about the treatment methods and planning the required nursing initiatives measuring the QoL of patients with CVI and reducing the effect of factors that have been found to lower the QoL of these patients conducting multi-center trials with a larger series to measure the QoL of patients with CVI.
Footnotes
Acknowledgements
This study was accepted as a Term Project in the Evening Non-Thesis Master’s Program of Celal Bayar University Institute of Health Science, Department of Surgical Nursing. It was also presented as a poster at the 9th Turkish National Congress on Surgery and Operation Room Nursing held on November 12-15, 2015.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.