
Abstract
Introduction
To investigate the diagnostic accuracy of an automated toe blood pressure device for detecting peripheral arterial disease in older people.
Methods
Ninety participants underwent toe and brachial blood pressure measurements and colour duplex ultrasonography of the right lower limb. Peripheral arterial disease was diagnosed if > 50% arterial obstruction was identified in any lower limb vessel using colour duplex ultrasonography. A receiver operating characteristic curve was analysed and the sensitivity and specificity of commonly used toe brachial index and toe blood pressure values were determined.
Results
The optimum toe brachial index threshold value for diagnosing peripheral arterial disease was 0.72 (sensitivity 76.2%, specificity 75%). The area under the curve was 0.829 (95% CI 0.743 to 0.915, p < 0.0001) suggesting fair diagnostic accuracy. A toe blood pressure of 70 mmHg was found to have excellent specificity (97.92%) for detecting PAD but poor sensitivity (42.86%).
Conclusions
The accuracy of automated toe blood pressure and TBI measurements was determined to be good when using colour duplex ultrasound as the reference standard for the non-invasive diagnosis of peripheral arterial disease. Results should be interpreted in the context of all clinical signs and symptoms.
Keywords
Introduction
Toe blood pressure and the toe-brachial index (TBI) provide an indication of small artery pulsatile flow at the periphery and are used to screen for lower limb vascular disease. 1 Calculated as the systolic blood pressure at the toe divided by the highest of the bilateral brachial systolic pressures, the TBI can be performed simply, without the need for referral or specialist training. 2 Both toe blood pressure and the TBI are known to have a valuable role in clinical practice. Toe blood pressure has been demonstrated to be predictive of foot wound healing and risk of amputation. 3 In addition, the TBI is recommended as the objective screening method of choice in place of the more widely used and accepted ankle-brachial index (ABI) for people with known or suspected medial arterial calcification – a condition of vascular stiffness that falsely elevates the ABI.1,4
Toe blood pressure and the TBI have been shown to have excellent inter- and intra-clinician reliability in people with and without diabetes.2,5 However, the sensitivity and specificity with which these measures reflect the extent of peripheral arterial disease (PAD) have not been widely investigated. Initial studies have reported excellent diagnostic accuracy in people with diabetes mellitus and the TBI has demonstrated good consistency when compared with the ABI.6–8 A TBI of 0.7 is currently recommended as a diagnostic limit, with ratios below this level indicative of PAD9,10 with normal TBI values estimated at 0.94–0.98. 11 However, values vary significantly in the literature with ratios from 0.55 to 0.75 having been used as the diagnostic indicator of PAD.4,12 A normal systolic toe pressure is generally considered to be 80% of brachial pressure; however, this can be influenced by cuff size, with small cuffs on large limbs resulting in spuriously high pressures. 13 Investigation of the diagnostic accuracy in the general population by comparing the TBI to an alternative reference standard assessing large artery patency is required.
The aim of this study was to determine the diagnostic accuracy of toe blood pressure and the TBI for detecting PAD when measured by automated toe blood pressure devices compared to CDU as a reference standard, in people meeting the criteria for routine PAD screening. Furthermore, the sensitivity and specificity of the TBI for detection of PAD using two commonly recommended threshold values was investigated.
Methods
Participants
The University of Newcastle Human Research Ethics Committee granted ethics approval (H-2010–1230). A sample of volunteers meeting current guidelines for lower extremity vascular screening was recruited from a podiatry clinic and from the local community. 14 All participants gave written informed consent prior to participation. Inclusion criteria were people aged over 50 years with a history of diabetes or smoking, or any person aged over 65 years. 14 Exclusion criteria included inability to give informed consent, contraindications to brachial and toe pressure measurement including history of deep vein thrombosis, lymphoedema of the arms or legs, ulceration, wound, infection or amputation of the hallux, connective tissue diseases such as scleroderma, vasospastic conditions such as Raynaud’s disease, history of mastectomy and inability lie in a supine position for 40 min.
Equipment
Toe systolic pressure was measured using a Systoe® (Atys Medical, Soucieu-en-Jarrest, France) automated toe blood pressure device consisting of a two pressure cuffs (occlusive cuff length 1.20 cm or 2.5 cm) and a photoplethesmography (PPG) probe which has previously been shown to have excellent reliability. 5 The SysToe® system uses an algorithm to allow for measurement of systolic pressures below 20 mmHg, and also contains an exsanguinating cuff along with an occlusive cuff. Brachial systolic pressure was measured using MicroLife BP A100 Plus (Microlife AG, Widnau, Switzerland) automated arm pressure cuff in either medium (22–32 cm) or large size brachial cuff (32–42 cm). Size of the SysToe® and brachial pressure cuffs selected were based on the bladder of the cuff being as close as possible to 80% of the circumference of the arm or digit. 15 The MicroLife automated blood pressure cuff has been validated against mercury sphygmomanometer. 16 CDU was performed with either a Phillips CX-50 (Philips Healthcare, Best, Netherlands) or GE Logiq-I (General Electric Healthcare, Waukesha, WI, USA). Parks Vascular Mini Lab 1050c with 8.2 Mhz CW Doppler was used for CW Doppler tracings (Parks Medical Electronics, Aloha, OR, USA).
Procedure
Participants attended two testing sessions no more than seven days apart. The first was held at one of two podiatry clinics and the second at one of two private vascular clinics, all in the Newcastle and Central Coast regions of New South Wales, Australia. For both testing sessions, participants were asked to avoid alcohol, exercise and caffeine for at least 1 h prior to attending for testing. 17 In the first testing session, toe and brachial measurements were performed with participants in a supine position at 20° from horizontal with room temperature maintained at 24–26℃. Participants rested for 10 min prior to measurement. 18 To measure toe blood pressure, the SysToe® automated device with PPG was attached to the plantar aspect of the right hallux and occluding cuffs placed around the digit. Cuff inflation and deflation were completed using the automatic setting. Only the right hallux toe pressure measurement was taken for each participant to satisfy the assumption of independence of data in statistical testing. 13 Brachial systolic pressure was measured at both arms using the MicroLife device that consists of an occluding cuff and pressure unit. All toe and brachial blood pressure measurements were performed by one of two podiatrists. We have previously demonstrated excellent inter-tester reliability for these devices. 5
Within seven days of toe and brachial pressure measurement, participants underwent CDU which was used as the reference standard. CDU was chosen, as participants in this study met the criteria for being at risk of PAD and were not necessarily exhibiting signs and symptoms or requiring revascularisation, and therefore were not undergoing arteriography. As screening tools such as the TBI are recommended for use on an at-risk population rather than only for those known to have advanced disease, we considered diagnosing by CDU was ethically acceptable and clinically more likely in this population. The CDU assessment was performed with participants in a supine position. CDU was performed from the abdominal aorta to the distal ankle on the right lower extremity following an overnight fast. For calculations relating to diagnostic accuracy, presence of PAD was defined as one or more arteries with > 50% stenosis. 19 Distal disease was defined as disease distal to and including the proximal popliteal artery, and proximal disease was disease from the common iliac artery to the distal superficial femoral artery. Grading of stenosis was conducted in accordance with the following criteria: 50–75% stenosis: focal increase in velocities 250 cm/s–350 cm/s and greater than threefold increase in velocities, 75–99% (>75%) stenosis – focal increase in velocities > 350 cm/s, fourfold increase in velocities, occlusion – vessel well visualised, no colour or Doppler flow seen. Information on the presence and extent of stenosis and medial arterial calcification was collected during CDU imaging. All CDU assessments were performed by one of three vascular sonographers. A subset of 10 randomly selected participants returned within one week of the initial CDU session and the scans were repeated by a different vascular sonographer to establish inter-tester reliability for this measurement.
Statistical analysis
Statistical analysis was performed using SPSS software version 19 (IBM, Chicago, IL, USA). Values from the right limb were used with CDU as the reference standard and a definition of PAD as at least one arterial stenosis of > 50% of the lumen. 19 The sensitivity and specificity of two common TBI threshold values for detecting PAD (<0.70 and < 0.75) were calculated and compared. A receiver operating characteristic (ROC) curve was generated to illustrate the performance of the TBI for the diagnosis of CDU-defined PAD and the area under the curve (AUC) was assessed. A sub-analysis was conducted in the same manner for people with diabetes. Inter-rater reliability of the CDU testing was calculated using the Kappa statistic.
Results
Participant characteristics.

Note: Data presented as mean ± standard deviation (range) or n (%).
TBI: toe brachial index; TBP: toe blood pressure.
Location and severity of arterial occlusion in (a) participants (n = 42) and (b) participants with diabetes (n = 24) with stenosis identified on colour-duplex ultrasonography.
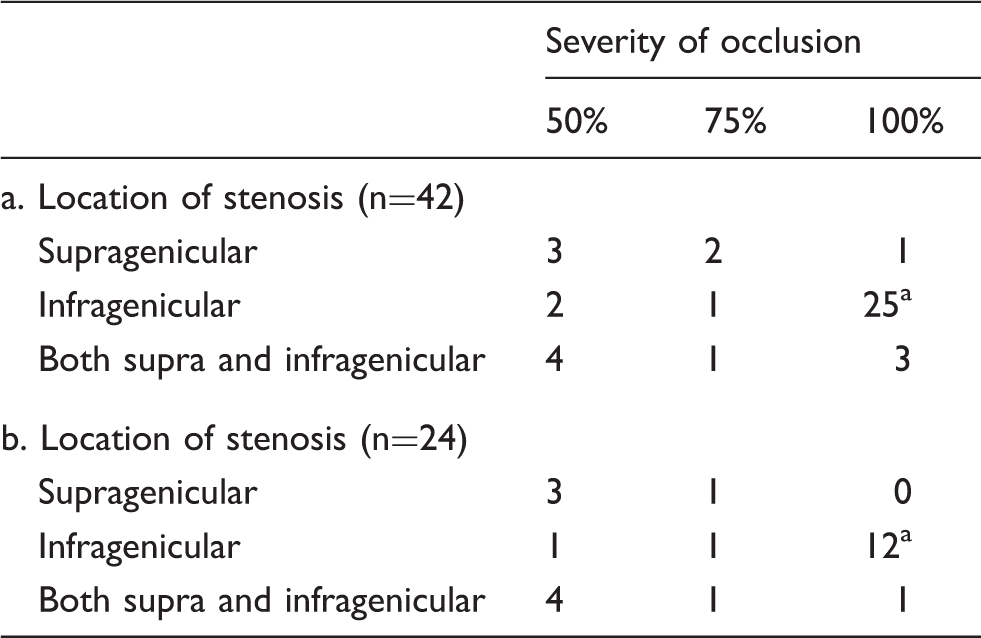
aTwo infragenicular arteries were occluded in four participants.
Diagnostic accuracy of selected toe-brachial index and toe blood pressure values.

95% CI: 95% confidence interval; TBI: toe-brachial index; TBP: toe blood pressure.
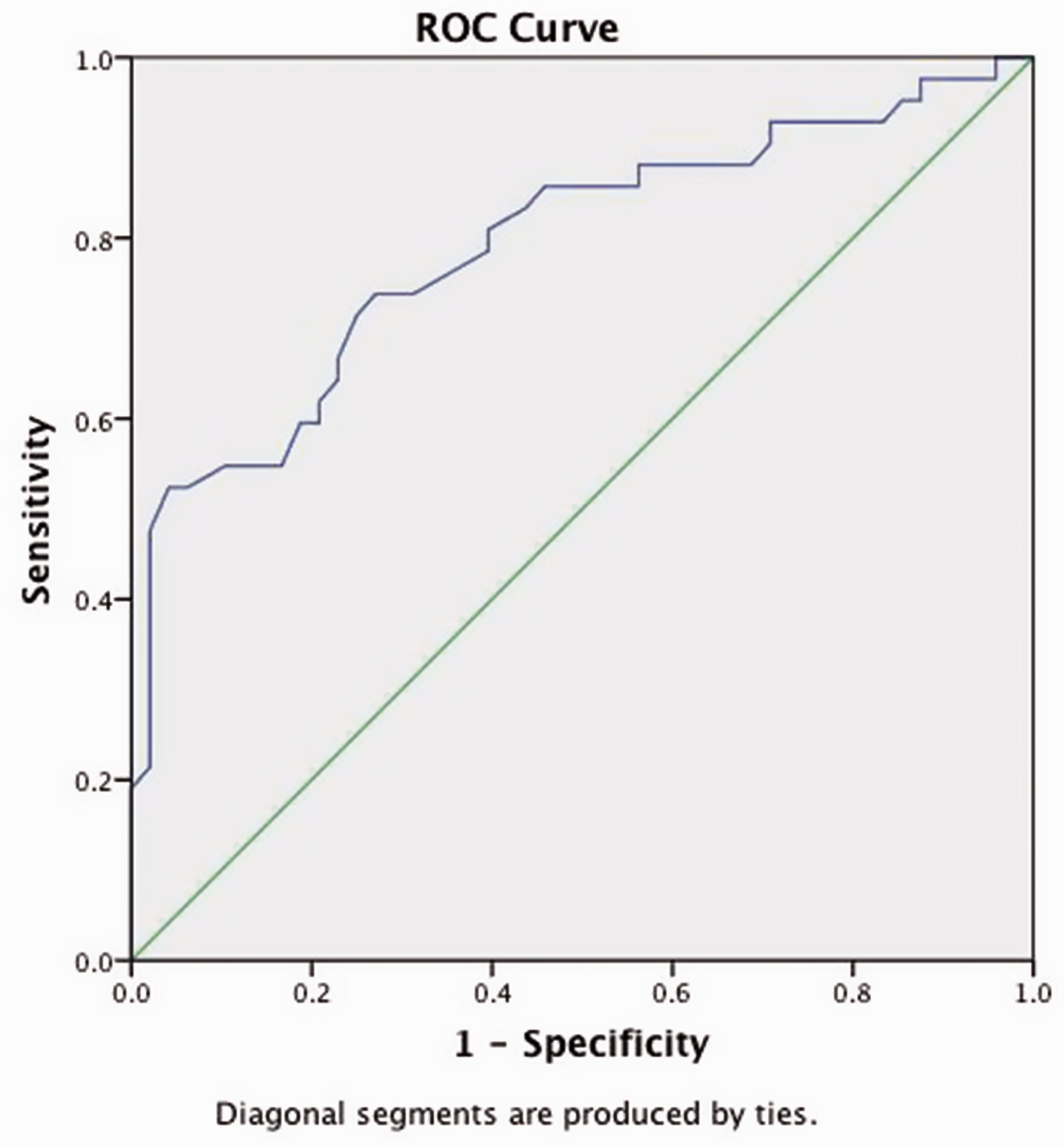
ROC curve for toe brachial index values for the entire population (n = 90).
In the sub analysis of participants with diabetes, sensitivity and specificity were highest using a threshold of < 0.70 (Table 3). Toe pressure had perfect specificity (100%) but poor sensitivity (45.86%).ROC analysis demonstrated the optimum threshold value for detecting > 50% stenosis was 0.73 (Figure 2) with a sensitivity of 66.70% and a specificity of 65.20%. The AUC was 0.74 (0.60 to 0.88) suggesting that the TBI was a fair test in this population.
ROC curve for toe brachial index values for participants with diabetes (n = 50).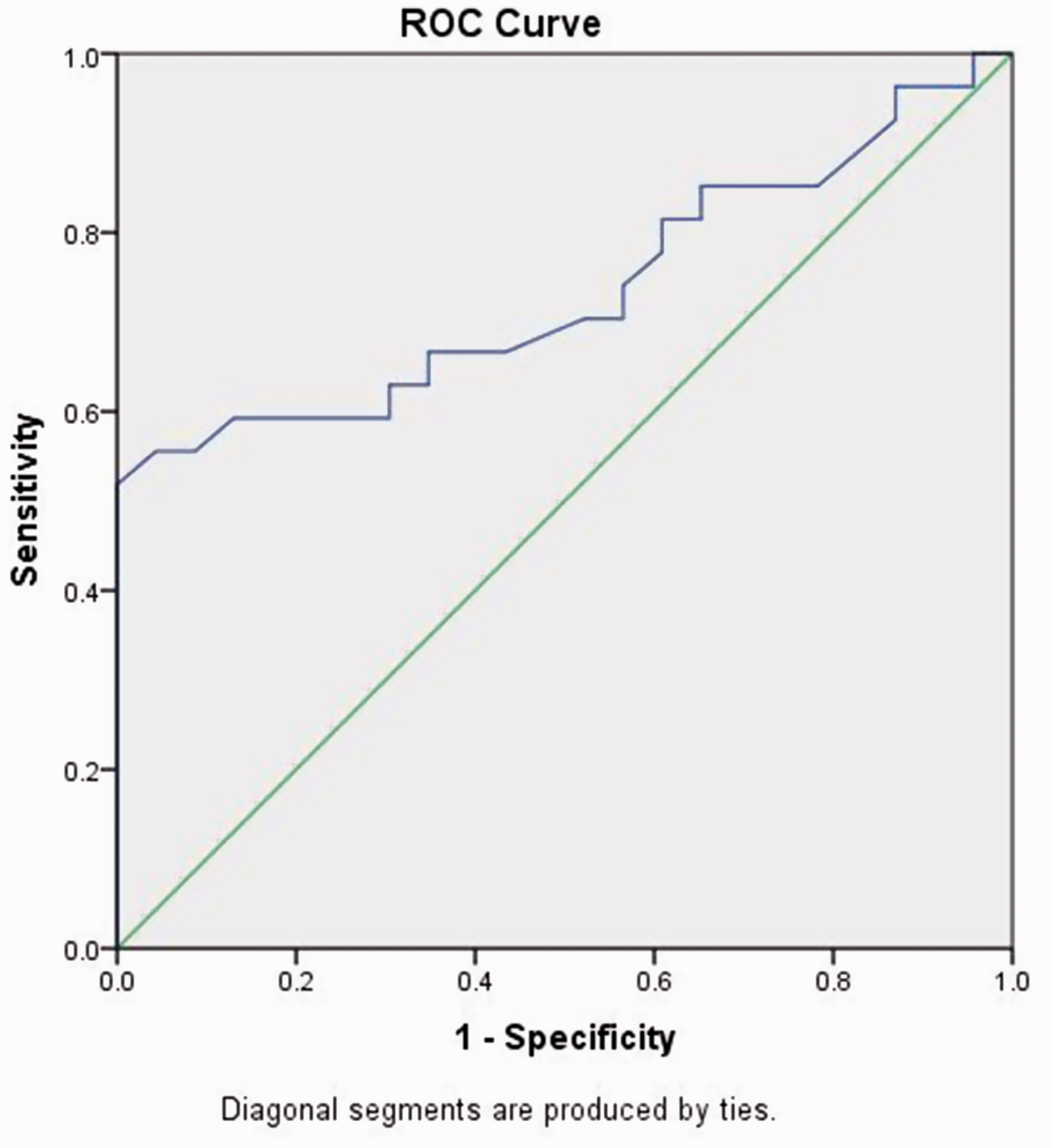
Discussion
The rising incidence and often asymptomatic nature of PAD requires accurate screening methods that can be performed simply by primary care clinicians. 15 As clinicians identify time restraints as a significant barrier to performing routine vascular screening, the use of automated equipment is common. 16 This prospective study of 90 participants is the first to investigate the efficacy of toe blood pressure and the TBI measured using automated devices for the diagnosis of PAD using CDU as the reference standard.
Our comparison of two commonly used threshold values showed a TBI of < 0.70 to be specific for the diagnosis of PAD and < 0.75 to be sensitive for PAD. ROC analysis determined the optimum threshold value to be 0.72. The results were similar in our sub-analysis of people with diabetes (0.73). There is currently a lack of consensus over the most effective threshold value for the TBI for detecting PAD. However, our findings suggest that a threshold of < 0.75 is likely to include people without significant disease and supports use of a threshold of < 0.70 as is currently recommended in international guidelines for PAD management.1,10 As there is not a strong evidence base to support the 0.70 threshold value advised, our present study contributes significantly to this area of literature.
Sub-analysis of the diagnostic accuracy of the TBI in participants with diabetes indicates the test did not perform as well with both sensitivity, specificity at threshold and the AUC was lower (AUC = 0.74) than in the whole study population. The lower AUC in the sub-analysis may in part be explained by the small sample size used in this analysis. This is likely to have contributed to imprecision in the result. 20 Recent evidence has demonstrated the TBI may be a superior test to the ABI in diabetes cohorts and, although likely affected by the sample size, our study demonstrated the TBI to have a greater AUC in people with diabetes than previously has been reported for the ABI (AUC: 0.58). 8 This suggests reassessment of the TBI measured by automated devices in people with diabetes in a larger sample is warranted.
We have also demonstrated that a toe blood pressure threshold value of 70 mmHg has superior specificity for the presence of PAD than the TBI. However, the sensitivity of this measure was poor, meaning it is likely to miss disease when present. The results of the present study reinforce the importance of interpreting these tests in the context of all clinical signs and symptoms. Toe blood pressure is therefore a potentially valuable tool for vascular screening of patients where there is a high degree of suspicion of significant PAD, however, is likely to be less useful at detecting mild disease or for screening at a community level.
A limitation of this research was the use of CDU as the reference standard rather than arteriography. CDU is used clinically to establish the location and extent of arterial stenoses in cases of suspected PAD.6,21–23 While CDU is a valid form of non-invasive assessment, it is heavily dependent on operator skill. An inter-tester reliability study was performed and shown to be adequate, yet the results are still subjective and dependent on clinician skill and experience. The inter-tester reliability testing of CDU was limited to a sample size of 10 due to financial restraints. This is a similar sample size to another study of diagnostic accuracy using CDU as a reference standard. 6 Although distal lesions occurring below the knee are typically hard to diagnose accurately, of the 28 participants in this study with a distal lesion, 25 (89%) had at least one complete occlusion. This makes incorrect diagnosis more unlikely for the majority of cases.
Diagnostic accuracy of the TBI may have been reduced in this cohort due to the high number of participants with a single infragenicular artery occluded which is likely to be well compensated for. In addition, the brachial and toe pressures taken by the automated devices were not validated against waveforms. By taking the pressure readings only from both automated devices, there is the risk that some inaccurate pressure readings were used in the data analysis despite the use of validated equipment. However, it likely that this is reflective of errors that would occur when taking automated pressure measurements in clinical practice. In addition, it should be noted that measurements were taken in a temperature controlled clinical environment to prevent ambient temperature affecting the results. This therefore does not reflect a typical clinical environment and cooler room temperature may reduce the toe pressure results, and affect the diagnostic accuracy of the test. In addition, participants with vasospastic disorders were excluded due to the possible effect of the disorder on toe pressure measurements, preventing these results being generalizable to such populations.
Conclusions
This study demonstrates the automated measurement of the TBI may be clinically applicable for ruling out the presence of PAD and has a role within the context of all signs and symptoms of a vascular assessment. The results support current recommendations for the interpretation of the TBI in the diagnosis of PAD. In addition, it may provide the initial evidence for the development of a system of classifying toe systolic pressure values and TBI. Based on these results, further investigations comparing the TBI to arteriography are warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The financial assistance for this study was provided by a Ramaciotti foundation grant.
Statement of patient consent
All participants provided informed written consent prior to participation in this study.