
Abstract
Objective
Thrombotic disease of the thoracic and abdominal aorta co-existing with aorto-iliac disease is a rare clinical association, which poses a great therapeutic challenge and adds to the complexity of the open surgical repair.
Method
We describe a case of 53-year-old woman with symptomatic thrombus in the thoracic and abdominal aorta down to the aortic bifurcation, which was successfully treated by Thoracic EndoVascular Aortic Repair via the left subclavian artery, open thrombectomy and aorto-iliac bypass.
Result
Completion angiogram performed through the axillary cannula showed good flow in the aorta, visceral vessels and iliac arteries.
Conclusion
This hybrid technical approach was a safe and effective strategy to tackle diffuse aortic thrombus with minimal morbidity and visceral embolization. Simultaneous aorto bi iliac bypass with thoracic endovascular aortic repair is a viable approach that can be undertaken with lesser morbidity and mortality risk as compared to complex and highly stressful total open surgical repair.
Case report
Consent was obtained from the patient to publish this case report along with the images.
A 53-year-old woman presented to our unit with bilateral rest pain and gangrenous toes (Rutherford Grade III). Significant medical history included removal of a pancreatic cyst complicated by a perforated oesophagus needing extensive surgery.
A computed tomography at the time of admission showed diffuse aortic thrombus deposition with bulky thrombus in the mid thoracic aorta and in the visceral segment aorta abutting the superior mesenteric artery (SMA) and both renal arteries (Figure 1).
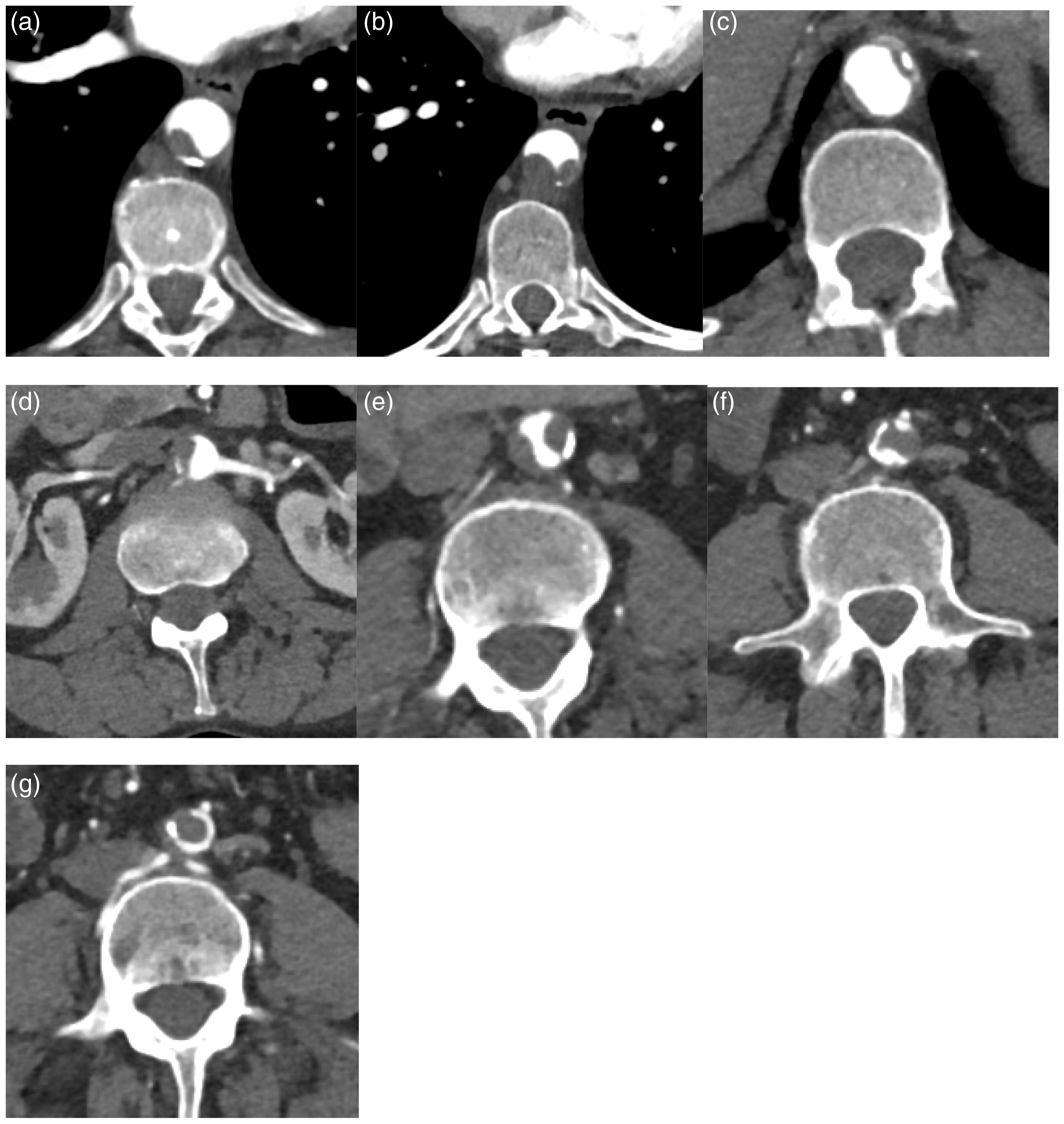
CT angiogram showing tandem lesions in (a) thoracic aorta, (b) lower thoracic aorta, (c) coeliac axis, (d) right renal artery, (e) infra-renal aorta, (f) infra-renal aorta, and (g) aortic bifurcation (axial views).
The distal abdominal aorta was diseased with thrombotic occlusion of the aorto-iliac segment (Figure 2). Both iliac arteries reconstituted with flow into both internal and external iliac arteries. The rest of the lower limb vessels filled normally. There were no overt features of a penetrating aortic ulcer or aortic dissection. A full pro-thrombotic screen was negative.

CT aorta showing tandem thrombotic lesions in the descending and infrarenal aorta (sagittal view).
A total endovascular or open repair posed a significant risk of dislodging the thrombi and causing visceral and/or distal embolization. We decided to use a hybrid technique to minimize this risk.
Procedure
A two-pronged approach was undertaken. Through a midline laparotomy, the visceral vessels were mobilized and controlled. The left axillary artery was exposed and a 22 × 105 mm Thoracic Stent Graft (COOK® Alpha stent graft) was deployed to jail the bulky mid thoracic thrombus. A CODA®−32 mm (Cook Medical) occlusion balloon catheter was used to occlude the distal thoracic aorta for less than 15 min. The abdominal aorta was then opened infrarenally. Thrombus was evacuated with the occlusion of visceral vessels briefly. The balloon was replaced by an infrarenal clamp and a graft was used to replace the aortic bifurcation.
Completion angiogram was performed through the axillary cannula which showed good flow in the aorta, visceral vessels, and iliac arteries (Figure 3). Her post-operative course was unremarkable. She was discharged home three days later with a prescription for oral warfarin. At 26-months follow-up, she was well and had no further embolic episodes.
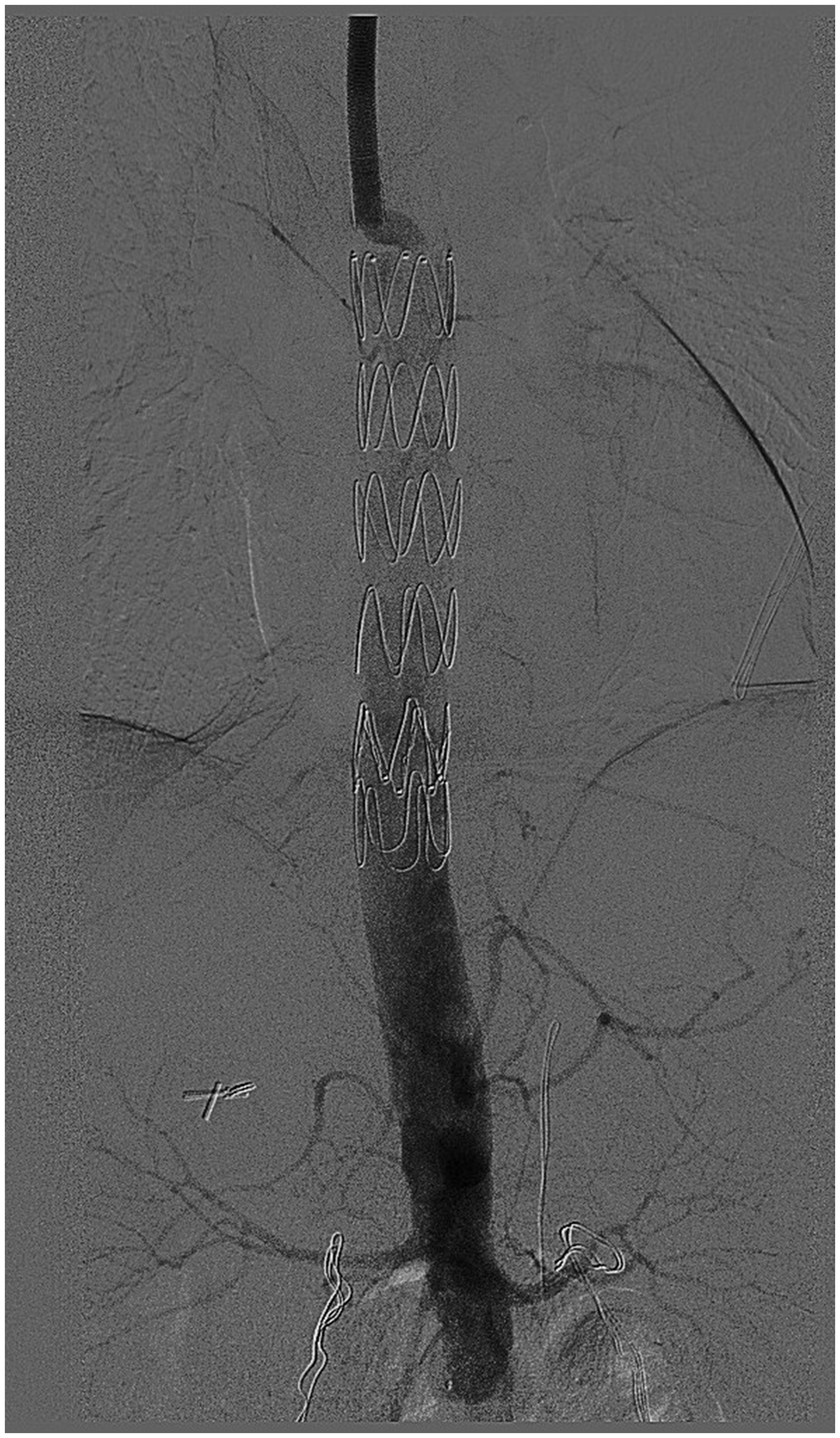
Completion angiogram of the aorta showing exclusion of thrombus and patent visceral vessels.
Discussion
In literature, primary aortic thrombosis is described as a rare entity where clotting occurs in a normal vessel without any obvious atheromatous lesion. Chemotherapy, illicit drug use, thrombocythemia, heparin-induced thrombocytopenia, and acute pancreatitis are some of the other conditions where primary aortic thrombosis may be associated. 1
This condition has been described in the peripheral arteries of the upper and lower extremities and a few authenticated reports of the same affecting the aorta 2 .
Commonly encountered cardio embolic presentations include stroke,3–6 an acutely threatened limb, blue toe syndrome, and abdominal ischaemic syndromes.7,8 Visceral complications include renal or splenic infarcts and mesenteric ischemia.
Contrast-enhanced multislice computed tomography remains the imaging modality of choice for the investigation of primary aortic thrombosis and assessment of potential complications.
The underlying pathogenesis of primary aortic thrombosis has not been well understood. The aim of the therapy is to abolish the thrombus burden and avoiding proximal or distal embolization.
One treatment option is medical therapy alone using therapeutic anticoagulation with or without antiplatelet therapy. 9 The second option is to use adjunctive anticoagulation with either open thrombectomy or thoracic endovascular aortic repair (TEVAR). 9 The third option is a hybrid technique using TEVAR and open thrombectomy for de-bulking of the thrombus in the abdominal aorta.
The Trans-Atlantic Inter-Society Consensus II classification reserved surgical therapy for those patients with complete aortic occlusion and disease involving the femoral bifurcation.
In our case, no underlying cause for thrombosis was found. The authors contemplate that the thrombi might have formed due to a combination of the factors described above. The disease involved the descending thoracic and infrarenal aorta, but spared the visceral aorta. Therefore, simultaneous stent grafting of the descending thoracic aorta (TEVAR) and standard aortobifemoral bypass allowed complete exclusion of all embolic sources.
Conclusion
An antegrade thoracic stent and balloon occlusion of the aorta is a novel technique for proximal control of the aorta. A hybrid technique using TEVAR and an aorto bi iliac bypass is a viable approach for de-bulking of thrombus in complex cases. This technique is associated with less morbidity and mortality risk compared to a complex and highly stressful total open surgical repair.
Footnotes
Acknowledgment
This paper has been presented at the 43rd Annual VEITHsymposium, New York, NY, USA, 18 November 2016.