
Abstract
Objectives
The use of postoperative anticoagulation is not uncommon for patients undergoing lower extremity arterial procedures as adjunctive therapy. Longer postoperative length of stay is necessary to achieve adequate therapeutic international normalized ratio with traditional protocols that call for the use of unfractionated heparin and warfarin therapy. We hypothesized the direct oral anticoagulants are an attractive alternative to provide adequate anticoagulation in patients who undergo lower extremity arterial procedures.
Methods
We retrospectively studied patients who had lower extremity arterial procedures between 2012 and 2015 to examine the safety and efficacy of the direct oral anticoagulants in a single institution. Patency, freedom from re-intervention, and major adverse limb event were evaluated. The direct oral anticoagulant agents used included dabigatran, rivaroxaban, and apixaban. The primary patency, adverse effects and freedom from re-intervention were then compared to a control group of patients who were treated with traditional heparin–warfarin therapy after lower extremity bypass procedures.
Results
Direct oral anticoagulants were utilized in a total of 23 patients (48% men; mean age 69 ± 11 years) during the study period. Indication for use of direct oral anticoagulant after procedure included use of polytetrafluoroethylene (PTFE) bypass graft below the knee joint or after lower extremity angioplasty with disadvantaged runoff. Mean follow-up of the drugs was 23 months (SD ± 16 months). At the end of follow-up, the direct oral anticoagulants have been discontinued in four patients, who are currently only on plavix. Among 82.6% of patients who were given direct oral anticoagulants for PTFE bypasses, graft patency, freedom from re-intervention, and major adverse limb event were 100%, 100%, and 0%, respectively. Patients (17.4%) treated with direct oral anticoagulants for disadvantaged runoff after balloon angioplasty of the lower extremity, patency, freedom from re-intervention, and major adverse limb event were 100%, 100%, and 0%, respectively. For the patients who underwent direct oral anticoagulant administration for disadvantaged runoff primary patency was 100%. One patient developed wound dehiscence which was unrelated to direct oral anticoagulant administration. Our control group consisted of 100 patients who were treated with heparin–warfarin therapy for 30 days after lower extremity bypass procedures. The graft patency, freedom from intervention, and major adverse limb event were 93%, 12%, and 0%, respectively. There was however no statistically significant difference in graft patency rate (P = .34) or freedom from intervention (P = .07) between the two groups.
Conclusions
The preliminary data suggest that there may be a role for using the direct oral anticoagulants with patients who undergo lower extremity arterial procedures for prevention of thrombosis and warrants further investigation.
Introduction
The Society for Vascular Surgery practice guidelines suggest the role of anticoagulants in reducing the risk of limb loss and increased primary patency of below knee PTFE bypass grafts in peripheral artery disease (PAD). 1 The use of postoperative anticoagulation as an adjunctive therapy is indicated in patients with prior revascularization, less than ideal conduit grafts and extremely disadvantaged runoff. There is also Level 2C evidence of the role of anticoagulants such as enoxaparin in patients with lower extremity vein grafts and stents. 1 In addition, patients with a history of atrial fibrillation or valve replacement require appropriate management to resume their pre-operative level of anticoagulation. 2 Traditionally, anticoagulation management postoperatively involves the use of unfractionated heparin with concurrent use of dose-adjusted warfarin. In-hospital intravenous heparin is used as a bridge until an adequate international normalized ratio (INR) is achieved as full anticoagulant effect of warfarin does not occur until two to three days of drug administration. 3 However, this contributes to not only delay in postoperative discharge, which occurs while waiting for the patients INR to become therapeutic but also is expensive when enoxaparin is used to bridge to warfarin.
Despite there being evidence of role of direct oral anticoagulants (DOACs) for venous thromboembolism (VTE), their use remains unexplored with arterial disease process. We decided to review our experience with the use of DOACs in the prevention of restenosis and thrombosis following revascularization procedures in patients with PAD and this remains an area for potential research.
Materials and methods
We retrospectively studied lower extremity arterial procedures performed between 2012 and 2015 to examine the safety and efficacy of the DOACs in a single institution. Patency of the PTFE graft and stents after angioplasty, freedom from re-intervention, and any major adverse limb event for each patient after procedure were evaluated. The DOAC agents we used included dabigatran, rivaroxaban, and apixaban.
Our paper focuses on the potential of use for post-procedural anticoagulation with DOACs after lower extremity bypass and angioplasty in patients with PAD. We used one of the three DOACs – dabigatran, rivaroxaban, and apixaban and analyzed the potential benefit from it with the patency of intervened limb, any reintervention and freedom from a major adverse event. The indications for DOAC in the patients involved in our study included the use of PTFE graft for bypass below the knee joint or after lower extremity angioplasty with disadvantaged runoff and failed medical therapy with aspirin/clopidogrel. The average follow-up duration after starting therapy with a DOAC agent in our study was 23 months (range: 3–53 months, SD ±16 months). The primary patency, adverse effects, and freedom from re-intervention were then compared to a control group of patients who were treated with traditional heparin–warfarin therapy after lower extremity bypass procedure. Postoperative anticoagulation was initiated in all patients with unfractionated heparin for 24 h, which was continued till INR was therapeutic and switched to warfarin.
The data collection and interpretation conformed to the principles set by the Declaration of Helsinki. Institutional Review Board of Vascular Institute of New York granted a waiver for informed consent as the study is of minimal risk and the data is blinded and retrospective.
Results
In our study from 2012 to 2015, DOACs were utilized in a total after 23 lower extremity arterial procedures. The average age of the examined population was 69 years old (range: 43–92 years old, SD ±11 years), and included 12 female and 11 male patients. DOACs were given to 82.6% patients with an indication after using a PTFE bypass. The PTFE grafts included femoro-below knee popliteal bypass (8) and femoro-tibial bypass (11). In these patients, the graft patency rate, freedom from re-intervention, and a major adverse limb event were 100%, 100%, and 0%, respectively. The remaining 17.4% of patients were treated with DOACs for disadvantaged runoff after balloon angioplasty of the lower extremity. These included saphenofemoral (SFA) to popliteal artery stent (3) and status post-thrombolysis of a SFA to below knee popliteal bypass (1). Among them, graft patency, freedom from re-intervention, and major adverse limb event were 100%, 100%, and 0%, respectively. For the patients who underwent DOAC administration for disadvantaged runoff, primary patency at six months was 100%. There was one patient who developed wound dehiscence which was unrelated to DOAC administration. However, there were no bleeding complications or thrombosis observed in all 23 patients. Table 1 reveals patient demographics involved in the study, comorbidities/risk factors for atherosclerosis and peripheral artery disease as well as the indications for DOAC therapy in our patients.
Patient demographics and indications for DOACs.
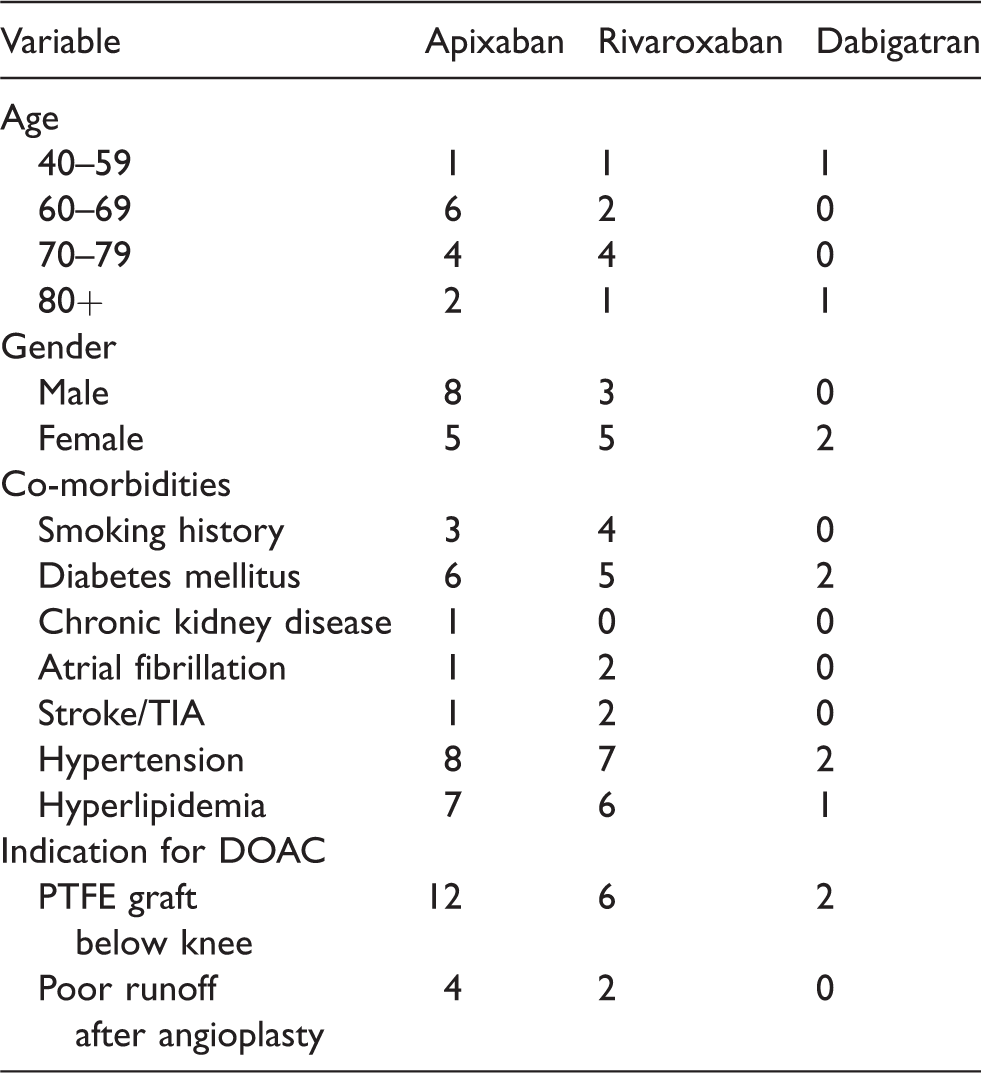
DOAC: direct oral anticoagulant; PTFE: polytetrafluoroethylene.
Note: Some patients had more than one indication for DOAC or more than one comorbidity.
The traditional heparin–warfarin group consisted of 100 patients (mean age: 72, SD ±12 years), among whom 49% were male. Among them, 69% were diabetic and 84% had hypertension as comorbidities. The graft patency, freedom from intervention, and major adverse limb event at six months were 93%, 12%, and 0%, respectively. When compared between the two groups, there was however no statistically significant difference in graft patency rate (P = .34) or freedom from intervention (P = .07) (Table 2).
Comparing efficacy of traditional heparin–warfarin therapy vs. DOACs.
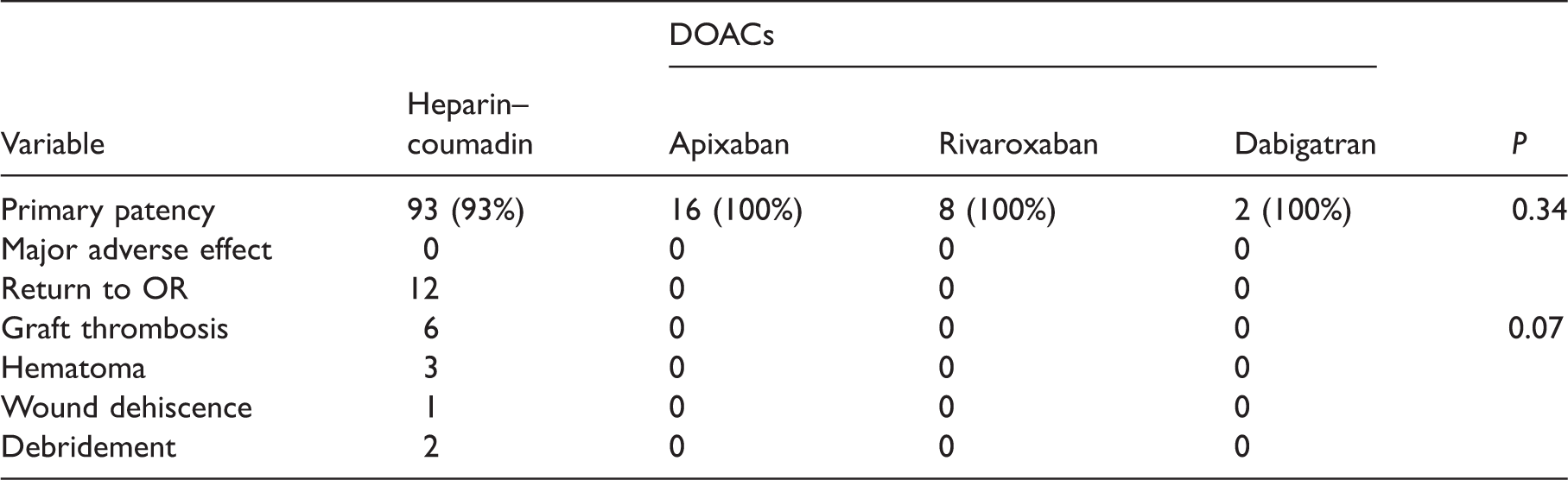
DOACs: direct oral anticoagulants.
Discussion
PAD treated with revascularization using either an autologous or synthetic graft bypass is associated with an occlusion rate between 12% and 60% after one year. 4 Adjuvant therapy with anticoagulants has thus been recommended to improve the patency rate following lower extremity below knee bypass prosthetic grafts. The study focuses on the potential for pharmacological treatment with DOACs after lower extremity arterial revascularization procedures.
DOACs are increasingly being considered in the treatment of VTE as a new standard of care of anticoagulation in the current CHEST recommendations. 5 In the EINSTEIN clinical trial, comparing rivaroxaban with the conventional treatment using enoxaparin/warfarin, it was found that rivaroxaban had similar safety and efficacy as conventional therapy and was associated with a significantly lower rate of major bleeding (Hazard Ratio HR(95% CI): 0.54(0.37–0.79)) and higher net clinical benefit (HR(95% CI): 0.77(0.61–0.97)). 6 In patients treated for VTE, major bleeding was reported in 1% of patients in the form of gastrointestinal (GI) bleeding, intracranial bleeding, or retroperitoneal bleeding; however, the risk was lower compared to conventional therapy. 7 Similarly, in the AMPLIFY clinical trial, comparing apixaban with conventional therapy in 5395 patients with VTE, apixaban was non-inferior to conventional therapy (P < .001). Major bleeding was reported in 0.6% of patients for those receiving apixaban compared to 1.8% for those receiving conventional therapy (Relative Risk RR 0.31(95% CI: 0.17–0.55), P < .001). Other non-fatal bleeding such GI bleeding (0.3%) for those receiving apixaban was lower compared to the conventional group (0.7%). Intracranial bleed and retroperitoneal bleed were also lower compared to the conventional group. 8 Thus, with VTE the DOACs are a considerably safe and effective alternative.
In our previous study, 2 we found that using enoxaparin 1 mg/kg every 12 h subcutaneously and adjusted dose warfarin daily, the mean postoperative length of stay was significantly reduced by two days after the procedure to discharge (P < .0001) in postoperative vascular patients. The enoxaparin self-injections also allow treatment as an outpatient. In addition, it is suspected that patient satisfaction was greater with early discharge, self-injection, and greater independence. However, it had its limitations being a parenteral option with risk of patient non-compliance/anxiety or inability to learn self-injection. 3 For these reasons, DOACS may be a feasible option as they not only allow early return to home but also are administered orally increasing drug adherence. In a study by Bamber et al., rivaroxaban was associated with greater patient satisfaction compared to enoxaparin/warfarin in the EINSTEIN-DVT studies because of its simplified treatment regimen. 6
In addition, the use of DOACs will reduce the number of coagulation laboratory tests required as compared to that for the follow-up of standard heparin–warfarin therapy. 10 In contrast to heparin and warfarin, DOACS do not require frequent monitoring of drug levels or coagulation times. This is not only an advantage for patients for whom frequent monitoring is a burden but also is a very cost-effective approach.
Another advantage with the use of DOACs is because of its pharmacokinetics. Warfarin pharmacokinetics is affected by the level of vitamin K intake, its absorption in the GI tract, as well as by the induction of hepatic cytochromes. Thus, warfarin is associated with a variable response due to its drug and food interactions, GI absorption, and reduced oral intake. These patients will have difficulty controlling their PT/INR and thus may benefit instead with the use of DOACs as they have less variability in drug effects.
There are however a few limitations with use of DOACS. Firstly, patients on DOAC, who do not or cannot take the medication as prescribed, may have a greater amount of time during which they are not therapeutically anticoagulated compared with patients who miss occasional doses of warfarin. The ability to monitor the degree of nonadherence is lost when a DOAC is substituted for warfarin. Secondly, DOACs are contraindicated in pregnant women and patients with prosthetic heart valves. Also renal insufficiency is a common setting in which heparin or warfarin maybe preferable to DOACs. Apixaban, however, is least dependent on renal clearance among the DOACs, and also accomplishes the goal at a substantially lower risk of bleeding compared to warfarin. 8 Dose adjustments however need to be made for use in patients with moderate renal insufficiency. Thirdly, for patients with bleeding disorders, it may be better to avoid DOAC as an antidote for dabigatran, idarucizumab has only recently been introduced and its use in the setting of an increased bleeding risk need to be studied in larger populations. With the development of new reversal agents for the factor Xa inhibitors andexanet alfa (ciraparantag), the issue of reversal may resolve in the near future. 11 Fourthly, vitamin K antagonists are typically much less expensive when compared to DOACs which are quite expensive in the current market. Lastly, our study cohort includes a small series of 23 patients with limited follow-up and hence these agents warrant further investigation in a larger population.
DOACs however present different properties and more options for individualized prophylaxis and treatment of thromboembolic events. These direct agents are certainly more convenient than vitamin K antagonists, and hold a promise of greater safety, improved outcomes, and better quality of life. However, the importance of their role in patients with risk of thrombosis due to PAD still needs to be investigated in larger studies.
Conclusion
The risk of recurrent limb ischemia after revascularization is high, and an ideal pharmacological regimen currently remains undefined. The preliminary data suggests therapy with DOACs has an excellent graft primary patency rate at the end of one year. Thus, there may be a role for using the DOACs with patients who undergo lower extremity arterial procedures and warrant further investigation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.