
Abstract
Traditional therapeutic options for complex thoracoabdominal aneurysm include open repair, hybrid repair or endovascular repair (involving fenestrated or branched endografts). The Streamliner Multilayer Flow Modulator has been available for treatment of thoracoabdominal aneurysms since 2010. Its design permits blood flow to perfuse through the mesh in a modus that preserves collateral branch patency, while modulating turbulent to laminar flow within the device. The flow then stagnates over time within the surrounding aneurysm sac. Significant complications, including paraplegia, renal failure and cerebrovascular accident, are much lower with Streamliner Multilayer Flow Modulator treatment. Application of the Streamliner Multilayer Flow Modulator to complex aortic pathologies presents a novel solution to an, as of yet, unmet clinical need, and has resulted in promising clinical outcomes when compared to existing solutions. The Streamliner Multilayer Flow Modulator offers potential for treatment of thoracoabdominal aortic pathologies in patients and is not just confined to those with complexity that dictates no other management options. While current literature illustrates that there is a decreased risk of mortality and associated complications when this new disruptive technology is utilised, there is still a need for prospective, long-term clinical trials, as well as comparative trials to accurately assess outcomes of Streamliner Multilayer Flow Modulator treatment that are both precise and reproducible. This article is a review of current clinical literature regarding contemporary flow modulating technology compared with open, branched and fenestrated managements, presenting early outcomes.
Keywords
Introduction
Open surgical repair (OSR) for complex thoracoabdominal aortic aneurysms (TAAA) has long been the gold standard. Any advancement in vascular technology that can deliver a minimally invasive but superior outcome over OSR is a bonus for the patient, his family and the treating physician. Minimally invasive repair offers less operative burden for the treating physician, as well as reduced incidents of mortality, stroke, paraplegia and in-hospital length of stay for the patient,1–7 all of which reduce the burden to the patient, family and physician. The Streamliner Multilayer Flow Modulator (SMFM; Cardiatis, Isnes, Belgium; Figure 1) has been available for treatment of thoracoabdominal aneurysms since 2010. Despite published studies since its introduction to the market, the technology is still considered tenuous and unpredictable to the majority of vascular surgeons and interventional radiologists. This is due to the unfamiliar mechanism of action of the SMFM when matched to conventional types of aortic repair, i.e. continued inclusion of the aneurysm sac following implantation. In fact, rather than exclude an aneurysm from circulation, the SMFM employs the body’s innate physiological process of remodeling to repair the aneurysm.
The Streamliner Multilayer Flow Modulator (SMFM; Cardiatis, Isnes, Belgium).
The SMFM design permits blood flow to perfuse through the mesh in a modus that preserves collateral branch patency, while modulating the flow from turbulent to laminar within the device.8,9 The flow stagnates over time in the surrounding aneurysm sac.8,9 Modulating flow within the aneurysm sac eases shear stress on the aneurysm wall and encourages the formation of organised thrombus. It is hypothesized that the laying down of an organised thrombus protects the aneurysm sac wall from turbulent shear stress, which could otherwise lead to rupture. Since receiving Conformité Européenne marking, the device has been successfully used to treat renal,8,10,11 peripheral and visceral artery aneurysms;9,12–17 aortic pathologies including ascending aortic, aortic arch, thoracoabdominal and abdominal aortic aneurysms, and aortic type B dissections.18–22 Level one evidence, 23 and the STRATO trial, 18 have affirmed the safety and effectiveness of the SMFM, in certain indications, in patients with complex thoracoabdominal pathologies, provided operators adhere to the strict indications for use. All studies reported successful treatment by reduction of flow velocity within the aneurysm sac leading to the formation of organised thrombus, while enhancing flow through collateral branches, increasing perfusion.
In the current era of continuously evolving endovascular technologies, there is a remaining unmet clinical need for a consistent and all-encompassing treatment alternative in complex aortic pathologies, and in instances where open or endovascular repair using a branched or fenestrated graft are not technically or physically feasible for the patient. The SMFM technology has come to the forefront of aneurysm repair in recent years however, it is still a controversial topic.
State-of-the-art
The first published systematic review, 23 and patient level meta-analysis of the SMFM, included 171 patients with complex aortic pathology. Overall 30-day mortality was 2.3%, with no reports of renal impairment or spinal cord ischaemia. The review included the STRATO trial by Vaislic et al., 18 which represents the most significant prospective trial on the SMFM to date. It assessed the SMFM for treatment of complex thoracoabdominal aortic aneurysms, specifically Crawford type II and Crawford type III TAAA. All-cause and aneurysm-related mortality at 30 days were both zero, with 100% technical success. This level one evidence also highlighted that SMFM use in aortic dissection regardless of chronicity has a favorable outcome, even when performed outside instructions for use (IFU). The MFM Global Registry has recorded 71 patients with Crawford type I–IV TAAA. Thirty-day mortality was 3%, while 30-day morbidity was 3%, with no incidences of aneurysm rupture, paraplegia/paraparesis or renal impairment.
Other studies on the SMFM include Lowe et al., 24 a retrospective observational analysis of the SMFM in the treatment of complex thoracoabdominal aneurysm, which could not be treated by any conventional means. All-cause and aneurysm-related mortality at 30 days were 7% (n = 1) and zero, respectively. However, this publication was perceived as negative and reignited controversy about the device. The authors report that the SMFM devices failed to influence the natural history of TAAA with one-year survival of 79% and aneurysm sac stabilisation in just two patients. The UK study reports outcomes from a single center using the first generation device on just 14 high-risk patients. All the patients were assessed and deemed unsuitable for either open repair or fenestrated/branch endovascular aortic repair (f/bEVAR), the latter being confirmed by the f/bEVAR endograft manufacturers. A lack of clinical understanding and universal experience with the SMFM meant that the employment of the devices was suboptimal. They were placed in aneurysms, which were too large, with 8 (57%) of the 14 patients having an aneurysm diameter greater than 6.5 cm. 25 Furthermore, the devices were undersized with inadequate overlap and were deployed too quickly, thereby inducing iatrogenic foreshortening. From the author’s experience, the SMFM devices should be deployed slowly at a rate of 2 cm per minute, giving a deployment time of up to 10 min for the 20-cm-long SMFM device. This process is known as “endoquilting”, whereby the device is deployed along the aortic arch curve allowing for relatively little splaying of the device interstitials. The device should touch the aortic wall, thereby facilitating early endothelialisation and stabilisation.
Traditional treatment options
Within the context of thoracoabdominal aortic aneurysm treatment, the therapeutic options for complex TAAA include OSR, hybrid repair (HR) or endovascular repair, including fenestrated or branched endografts (TEVAR, f/bEVAR). Depending on the complexity of the pathology, current treatment options can involve extensive aortic replacement and open anastomosis using various managements such as left heart bypass, femoral–femoral bypass with/without hypothermia, cardiopulmonary bypass or passive aortic shunting. Despite these advances in ancillary techniques, OSR remains very high risk and still carries a high associated 30-day mortality of approximately 9–21% (Table 1), despite utilisation of circulatory arrest and cerebral perfusion techniques.1–4 Serious adverse events such as paraplegia/paraparesis, stroke or permanent renal impairment are a reality for these patients, with incidents as high as 4–10%, 1–5% and 7–16%, respectively (Table 1).1–4
Thirty-day outcomes comparing open surgery, hybrid, f/bEVAR and the SMFM.
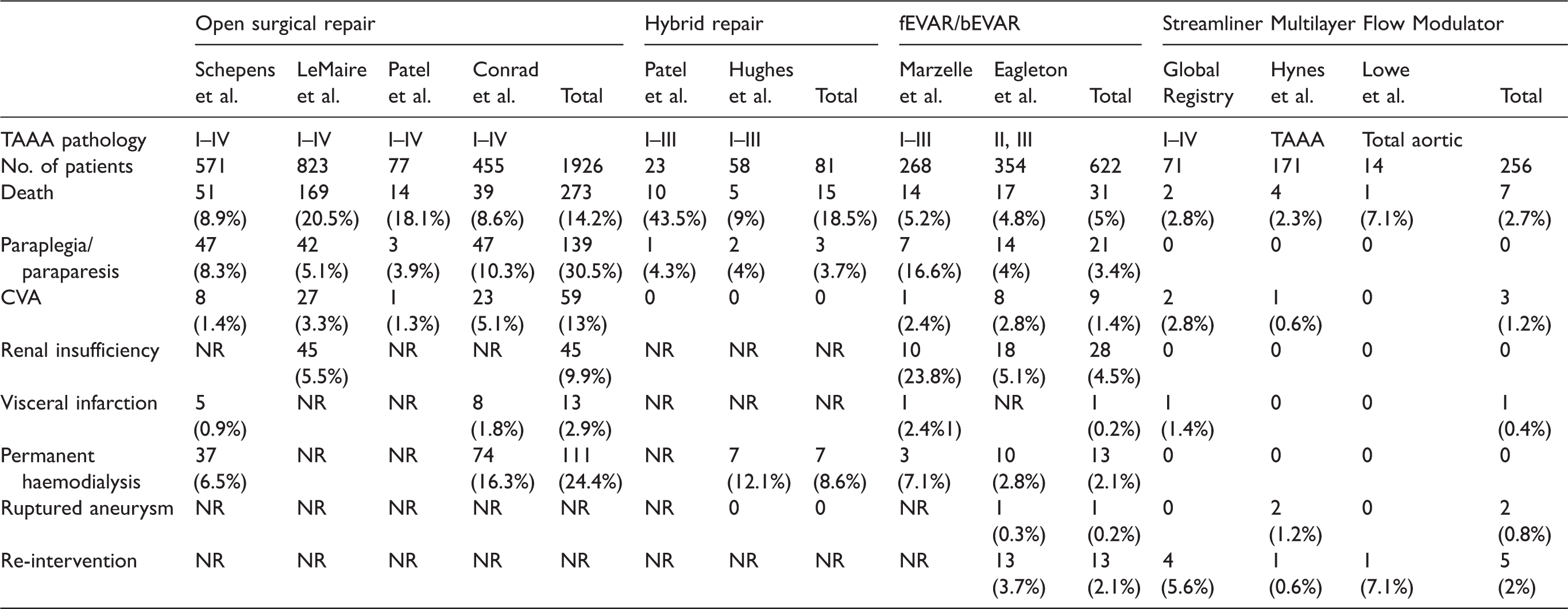
CVA: cerebrovascular event; NR: not reported.
Hybrid techniques, using a combination of endovascular and open surgical approaches to treat aortic pathologies, are considered as a less invasive method. The type of repair chosen depends on the complexity of the pathology to be treated. For this purpose, highly specialised debranching grafts have been developed. Hybrid approaches have demonstrated a significant 30-day mortality of 9–44% (Table 1). 3 Incidents of paraplegia/paraparesis and permanent haemodialysis were 4% and 12.1%, respectively (Table 1).3,5 To date, the superiority of HR when compared to OSR, or vice versa, has not been established. In fact, when used in high-risk patients, significant mortality and morbidity was demonstrated.3,5 However, novel combinations of devices have been utilised successfully in HR, but these remain anecdotal. One such successful case consisted of debranching of the supra-aortic vessels, followed by TEVAR (10 days later) with a custom-made thoracic endoprosthesis and the SMFM. 26 The patient was reported as still surviving 24 months after discharge, with no postoperative complications observed, and all collateral vessels arising from the aneurysm were patent.
Fenestrated and branched technologies are being utilised to exclude aortic aneurysms but allow visceral branch flow. 27 They present considerable difficulty for operator utilisation and require intense pre-operative planning to fit specific complex arterial and aneurysm morphologies. 28 Past studies demonstrate a 30-day mortality of 5% (Table 1), while complications such as paraplegia/paraparesis, stroke and permanent haemodialysis were as high as 4–17%, 2–3% and 3–7%, respectively (Table 1).6,7 Early feasibility studies agree that although f/bEVAR is a promising technique, it carries a significant rate of morbidity and mortality relating to the extent of the aneurysm pathology, and the actual complexity of the procedure itself.6,7 In addition, we must address other complicating factors such as the invasiveness of multiple graft insertions and their implications for aortic branch dissection and/or thrombosis, as well as the overall systemic burden sustained to the patient. Although there are other devices that are currently under investigated in early feasibility clinical trials that are off the shelf, modular, multi-component systems, and do not require pre-operative planning, such as the Gore Excluder, Thoracoabdominal Branch Endoprosthesis (TAMBE; ClinicalTrials.gov Identifier: NCT02528500) and the Medtronic Valiant TAAA stent graft system (ClinicalTrials.gov Identifier: NCT02294435), 29 limitations regarding anatomical morphology do apply, e.g. a high degree of angulation.
The future of TAAA treatment
Disruptive stent technologies are available for clinical use in intracranial aneurysm repair.30–32 Self-expandable intracranial stents are increasingly used to treat complex aneurysms such as wide-necked and fusiform aneurysms.30–32 Literature concerning intracranial flow diverters has yielded positive results, with high aneurysm occlusion rates,33,34 thereby fueling interest in applications of this technology to larger arteries.
Application of the SMFM to complex aortic pathologies presents a novel solution to an, as of yet, unmet clinical need, and has resulted in promising clinical outcomes when compared to existing solutions. Pooling the populations for each intervention type, the SMFM offers a superior 30-day mortality of 3% (Table 1). This is followed by f/bEVAR and OSR, while HR offers patients the worst 30-day survival with a mortality rate of 19% (Table 1). Significant complications, including paraplegia, renal failure and CVA, are much lower with SMFM treatment, when compared to other methods. SMFM late outcomes will need to be studied and weighed against the positive late outcomes that are experienced in OSR, HR and f/bEVAR.
Positive 30-day outcomes illustrate that the SMFM offers potential for treatment of thoracoabdominal aortic pathologies and has the possibility of not just being confined to those with complexity that dictates no other management options. This mode of treatment is minimally invasive and offers less hospital stay when compared to OSR, HR and f/bEVAR. 23 An 18–20 F sheath size used to deliver the SMFM (35–50 mm) to the target vessel is typically smaller than that of many other TEVAR delivery systems, with few exceptions.
Significantly, patients treated with the SMFM are not subjected to bypass methods, which can be fraught with complication, and threaten the otherwise positive outcomes of open interventions. Without the need to selectively cannulate branch vessels, there is much less total fluoroscopy time, less total contrast agent administered and reduced risk of visceral embolisation or branch dissection.25,35–38 The SMFM has shown positive results (Figure 2), but nevertheless there are diverse opinions on its use. Initially, the SMFM was disseminated to the vascular community without the need for ardent operator knowledge, resulting in improper use of the device, and complications have been reported such as device foreshortening upon insertion and subsequent dislocation as a result.24,39,40 Furthermore, the device was almost exclusively used in patients with multiple co-morbidities who ultimately died from a secondary cause.

Successful treatment of a Crawford Type II aneurysm with the SMFM (female, 75 years): (a) pre-operative CTA and (b) postoperative CTA (13 months).
IFU stipulate a landing zone and overlap of approximately 6 cm between devices, and 8 cm in acute angles, with minimum oversizing of 20%. 23 However, user experience now indicates an even greater amount (at least 8 cm in severe tortuosity) to ensure a positive outcome, along with the process of “endoquilting” as mentioned. We also recommend that the SMFM should not be deployed in TAAA diameters greater than 6.5 cm, or greater than 450 cm3 in volume, due to adventitial elastolysis, which occurs in larger diameter aneurysms and has a direct effect on the aneurysms ability to remodel. Inadequate operator knowhow on deployment of the SMFM and improper use of the device outside of IFU have resulted in poor survival for patients.23,35 The authors have made further recommendations for revision of the SMFM’s IFU, which are beyond the scope of this article but have been published by Sultan et al. 25
While current literature illustrates that there is a decreased 30-day risk of mortality and associated complications when this new disruptive technology is utilised, there is still a need for prospective, long-term clinical trials, as well as comparative trials to accurately assess long-term outcomes of SMFM treatment that are both precise and reproducible. Positive animal model results,41–45 in combination with clinical outcomes such as those published recently,23,36–38 will instill confidence in the wider vascular community for this type of disruptive technology. Without this, the opinion on the SMFM will still remain divided.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper/research is supported by the Competitiveness Operational Programme 2014–2020, financed from European Regional Development Fund and by the Romanian Government under the project “Next generation computer aided research in cardiovascular disease management –NextCARDIO”, project code: COP P_37_701.