
Abstract
Abstract
Background
Asymmetric dimethylarginine is suggested to be a marker of poor prognosis in patients with atherosclerosis. However, the predictive role of circulating asymmetric dimethylarginine for clinical outcome in patients with peripheral arterial disease has not been determined.
Aims
To quantitatively assess the predictive value of circulating asymmetric dimethylarginine for clinical outcome in patients with peripheral arterial disease in a meta-analysis of prospective cohort studies.
Methods
Relevant studies were identified by systematically searching of PubMed and Embase databases. A random-effect model was used to synthesize the results. Sensitivity analyses by omitting one study at a time were performed to evaluate the robustness of the results.
Results
Six studies with 2535 peripheral arterial disease patients were included. Patients with higher circulating asymmetric dimethylarginine at baseline were associated with higher risk of all-cause mortality (adjusted hazard ratio: 1.63, 95% confidence interval: 1.28–2.06, I2 = 16%), and major adverse cardiovascular events (adjusted hazard ratio: 2.01, 95% confidence interval: 1.08–3.73, I2 = 78%) as compared with those with lower circulating asymmetric dimethylarginine at baseline. Specifically, every increment of 0.1 µmol/l of asymmetric dimethylarginine was associated with 18% (adjusted hazard ratio: 1.18, 95% confidence interval: 1.06–1.31) increased risk for all-cause mortality and 14% (adjusted hazard ratio: 1.14, 95% confidence interval: 1.04–1.25) increased risk for major adverse cardiovascular disease. Sensitivity analyses by omitting one study at a time did not significantly change the results.
Conclusion
Higher circulating asymmetric dimethylarginine at baseline may be associated with higher incidence of cardiovascular events and mortality in patients with peripheral arterial disease.
Introduction
Peripheral arterial disease (PAD) is the manifestation of atherosclerosis of the peripheral arteries. 1 The prevalence of PAD in the general population varies between 3 and 10%, depending on age of the populations studied.2,3 Increasing evidence from observational studies suggest that patients with PAD are at higher risk for cardiovascular events, including ischemic heart disease, heart failure, atrial fibrillation, stroke, and cardiovascular deaths, particularly in those of advanced PAD. 4
Many pathophysiological processes have been suggested to be involved in the pathogenesis and progression of PAD, such as inflammation, oxidative stress, and endothelial dysfunction.5–7 As a key maintainer of endothelial function, nitric oxide (NO) is generated by
Methods
This systematic review and meta-analysis was prepared in according with the Meta-analysis of Observational Studies in Epidemiology 21 and the Cochrane’s Handbook 22 guidelines during the study design, implementation, data analysis, and results reporting processes.
Database searching
PubMed and Embase databases were searched for relevant studies using the term “asymmetric dimethylarginine,” or “ADMA,” coupled with “peripheral artery disease,” “peripheral vascular disease,” “critical limb ischemia,” “intermittent claudication,” “peripheral arterial disease,” “peripheral artery obstructive disease,” “Buerger’s disease,” “PAD,” “PAOD,” or “CLI.” We limited the searching to studies in humans and published in English. The reference lists of the related original and review articles were also manually screened for potential relevant studies. The final literature searching was performed on 14 February 2017.
Study selection
Studies were included if they fulfilled all of the following criteria: (1) published as full-length article in English; (2) designed as prospective cohort studies, without limitations of the sample size and follow-up duration; (3) including adult patients of PAD; (4) circulating ADMA was measured at baseline; (5) documented outcomes of all-cause mortality or major adverse cardiovascular event (MACE) during the follow-up; (6) reported multivariable adjusted risks (at least for age) for all-cause mortality or MACE in patients with higher circulating ADMA at baseline as compared those with lower circulating ADMA at baseline. According to the definitions of the original studies, MACE was defined as the incidence of the combined outcome of nonfatal myocardial infarction, nonfatal stroke, coronary revascularization via percutaneous coronary intervention or coronary artery bypass graft, endovascular therapy for PAD, amputation, and cardiovascular death. Letters, editorials, noncohort studies, baseline circulating ADMA not reported or measured, or those did not report outcomes of all-cause mortality or MACE were excluded. When duplications of the data were found, the results of the study with the largest sample size were included in the meta-analysis.
Data extraction and quality evaluation
Two authors independently performed literature searching, data extraction, and quality assessment according to the predefined inclusion criteria. Discrepancies were resolved by consensus and discussion with the third author. The extracted data included the details regarding study and patient characteristics, including the name of the first author, year of publication, total number of PAD patients included, mean age, gender, baseline mean ABI, comorbidities of diabetes mellitus (DM), hypertension, and CAD, current smokers, and proportions of patients taking statins. Follow-up information and the data related to study outcomes were also extracted, including follow-up duration, numbers of patients with interested outcomes, strategy to confirm the outcome incidence, methods of ADMA measurement, and potential confounding factors adjusted when presenting the results. The effect sizes reported including hazard ratio (HR) with their corresponding 95% confidence intervals (CIs) were extracted. When data of various degrees of adjustment were reported, we only extracted the most adequately adjusted data. We evaluated the quality of the include studies using the Newcastle–Ottawa Scale (NOS). 23 This scale judges the quality of each cohort study regarding three aspects: selection of the study groups, the comparability of the groups, and the ascertainment of the outcome of interest.
Statistical analyses
We used HR as the measure for the associations between baseline circulating ADMA and the risk of all-cause mortality or MACE in patients with PAD. Data of HRs and their corresponding stand errors were calculated from 95% CIs or p values, and were logarithmically transformed to stabilize variance and normalized the distribution. The heterogeneity among the included studies was detected by the Cochrane’s Q test 22 and the I2 24 test. If I2 > 50%, a significant heterogeneity was considered. A random-effect model was applied to synthesize the results because it is a more generalized method which incorporates the heterogeneity of the included studies when combing the results. 22 Sensitivity analyses, by removing individual study one at a time, were performed to test the robustness of the results. 25 Potential publication bias was assessed by visual inspection of the funnel plot as well as the Egger regression asymmetry test. 26 Since the results were reported with circulating ADMA presented as different variable types (categorical or continuous) in each study, we summarized the results with two manners: first, circulating ADMA was divided into several levels (categorical variable), and the effect size for those with the highest category as compared with the lowest category was reported; second, the HRs for every 0.1 µmol/l increment of the circulating ADMA (continuous variable) on the incidence of interested outcomes were combined. RevMan (Version 5.1; Cochrane Collaboration, Oxford, UK) and STATA software (Version 12.0; Stata Corporation, College Station, TX) were used for the meta-analysis and statistics.
Results
Searching results
The process of literature searching was shown in Figure 1. Briefly, 116 studies were retrieved by initial database searching and exclusion of the duplications. By screening via title and abstract of the publications, 102 studies were subsequently excluded, mainly because they were irrelevant to the objective of the current study. The remaining 14 studies underwent full-text review, and eight studies were further excluded because two studies were not relevant studies to the current meta-analysis, one was not prospective cohort study, four did not report the outcome of interest, and the other one was not performed in patients with PAD. Finally, six prospective cohort studies9,16–20 were included in the present meta-analysis.
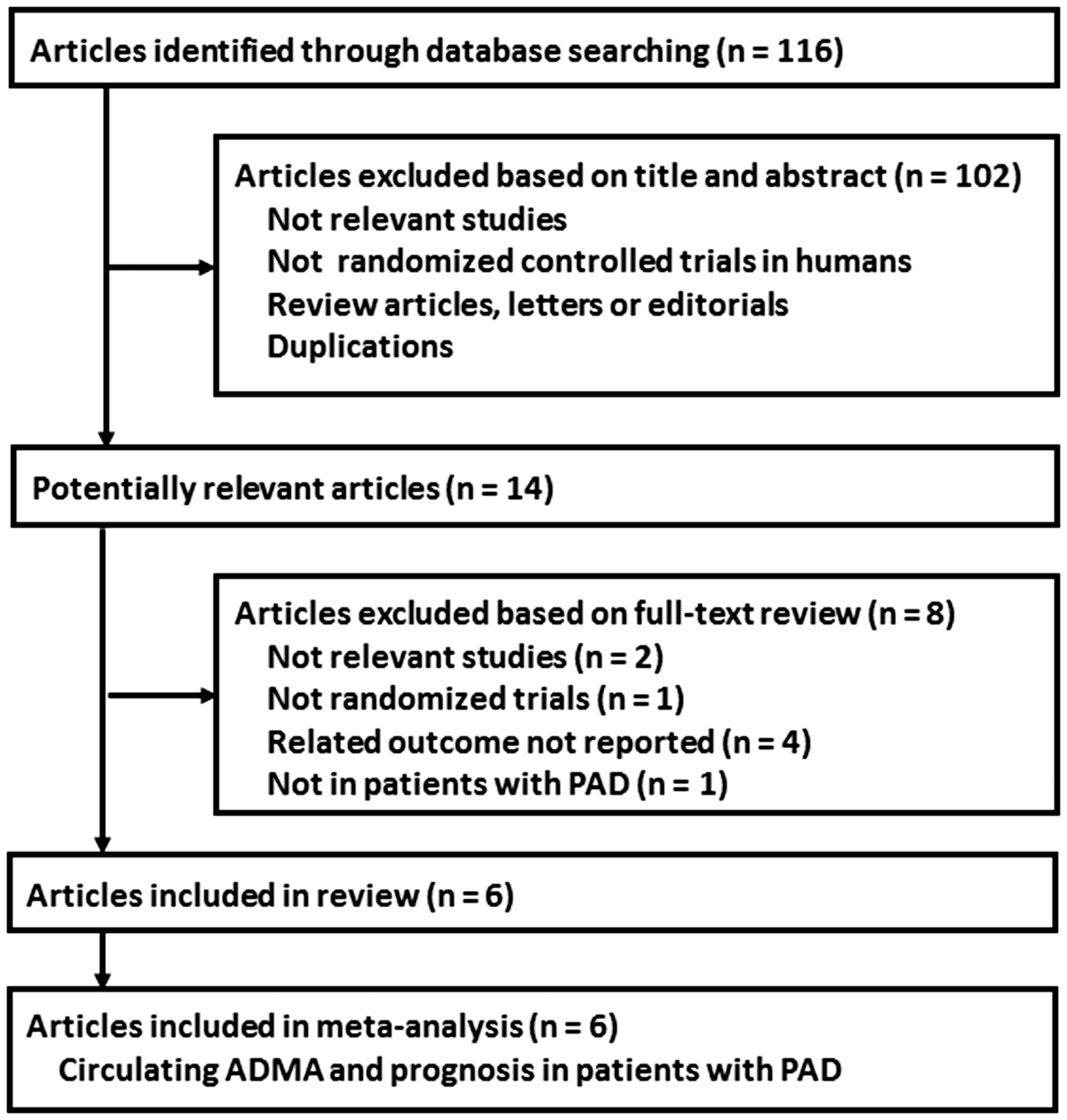
Process of literature searching.
Study characteristics and quality evaluation
The characteristics of the included cohorts were listed in Tables 1 and 2. Overall, our meta-analysis included six cohort9,16–20 studies published after 2016 with a total of 2535 PAD patients. The mean age of the included patients varied between 57.6 and 74.0 years, with the proportions of men ranging between 54.1 and 100%. The mean ABI at baseline varied from 0.56 to 0.72. Substantial patients of the include studies were with hypertension (65.3–86.0%), DM (16.0–36.8%), CAD (21.2–74.0%), current smoking (15.6–35.8%), and taking statins (43.0–64.8%). The measurement of baseline ADMA was performed with a high performance liquid chromatography method in five studies,9,17–20 while with an enzyme linked immunosorbent assay in the other one study. 16 The included studies were generally of good study quality, with the NOS varying between 8 and 9.
Baseline characteristics of the patients included in the randomized controlled trials.

ABI: ankle–brachial index; CAD: coronary artery disease; CLI: critical limb ischemia; DM: diabetes mellitus; HTN: hypertension; IC: intermittent claudication; LLR: lower limb revascularization; NR: not reported.
Study design and outcome characteristics of the included randomized controlled trials.
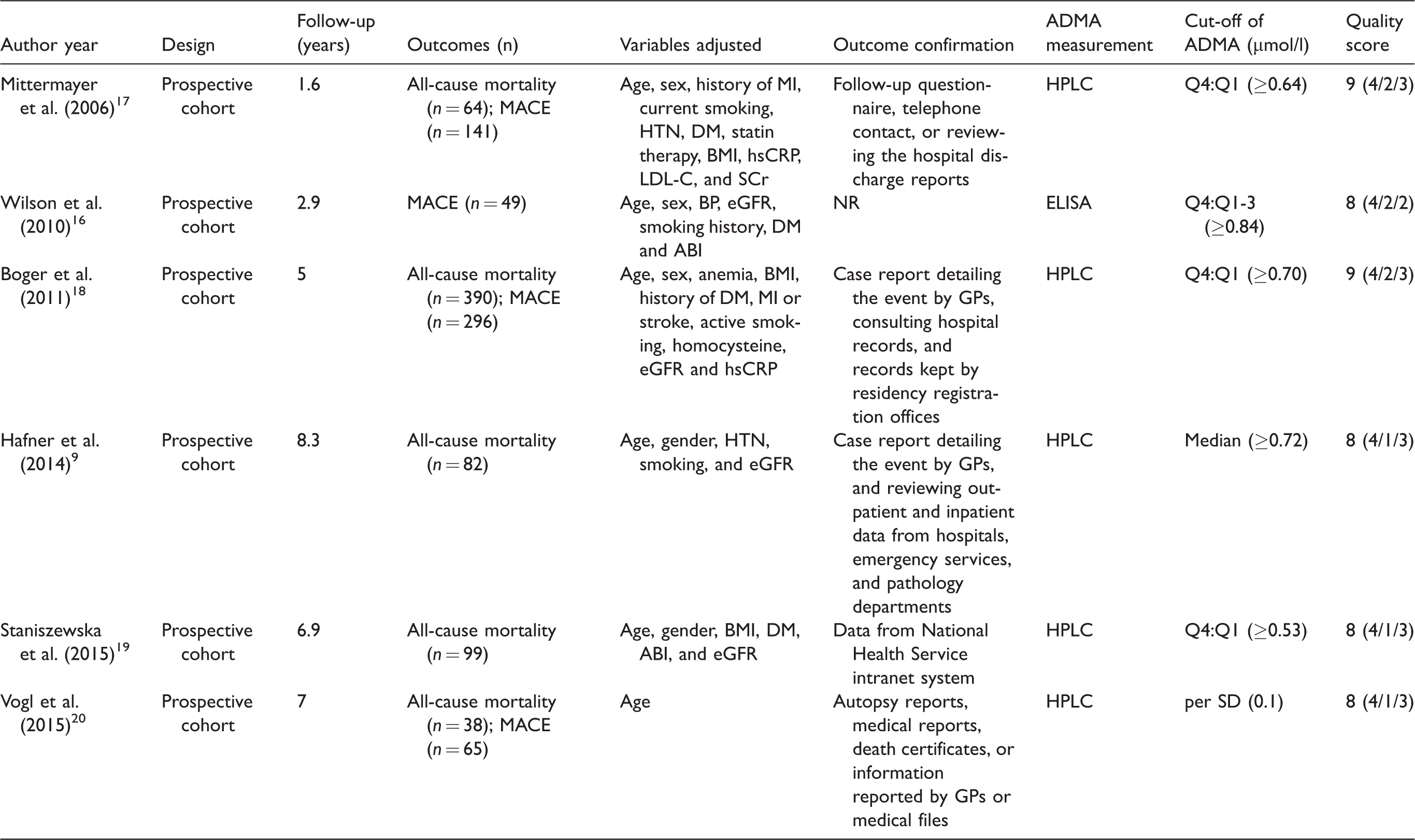
ABI: ankle–brachial index; ADMA: asymmetric dimethylarginine; BMI: body mass index; BP: blood pressure; DM: diabetes mellitus; eGFR: estimated glomerular filtrating rate; ELISA: enzyme linked immunosorbent assay; GP: general practitioner; HPLC: high performance liquid chromatography; hsCRP: high-sensitive C reactive protein; HTN: hypertension; LDL-C: low-density lipoprotein cholesterol; MACE: major adverse cardiovascular events; MI: myocardial infarction; NR: not reported; Q: quartile; SCr: serum creatinine.
Circulating ADMA at baseline and all-cause mortality in PAD patients
Overall, four studies9,17–19 with 2178 patients reported the association between baseline ADMA as a categorized variable and the all-cause mortality in PAD patients. No significant heterogeneity was detected among these studies (p for Cochrane’s Q test = 0.31, I2 = 16%), and the pooled results with random-effect model showed that patients with higher circulating ADMA at baseline were associated with significantly higher risk of all-cause mortality as compared with those with lower circulating ADMA at baseline (adjusted HR: 1.63, 95% CI: 1.28–2.06, p < 0.001; Figure 2(a)). Consistently, by pooling the data of five studies9,17–20 with 2410 patients, results of the meta-analysis with a random-effect model indicated that higher circulating ADMA at baseline was associated with higher mortality risk in patients with PAD (adjusted HR: 1.18 for every increment of 0.1 µmol/l ADMA, 95% CI: 1.06–1.31, p = 0.003; Figure 2(b)) with no evidence of significant heterogeneity (p for Cochrane’s Q test = 0.19, I2 = 35%). Sensitivity analyses by omitting one study a time did not significantly change the overall results, suggesting the robustness of our study (data not shown).

Forest plots for the associations between circulating ADMA and all-cause mortality in patients with PAD. (a) Forest plots with circulating ADMA as categorical variable (higher versus lower circulating ADMA); (b) forest plots with continuous ADMA as categorical variable (every increment of 0.1 µmol/l of ADMA). ADMA: asymmetric dimethylarginine; PAD; peripheral arterial disease.
Circulating ADMA at baseline and incidence of MACE in PAD patients
Meta-analysis based on three prospective cohort studies16–18 (1881 PAD patients) showed that higher circulating ADMA at baseline was associated with significantly higher risk of MACE as compared with those with lower circulating ADMA at baseline (adjusted HR: 2.01, 95% CI: 1.08–3.73, p = 0.03; Figure 3(a)) with significant heterogeneity (p for Cochrane’s Q test = 0.01, I2 = 78%). Subsequent study pooling the data of four studies16–18,20 (2113 patients) showed that higher circulating ADMA at baseline was associated with higher incidence of MACE in PAD (adjusted HR: 1.14 for every increment of 0.1 µmol/l ADMA, 95% CI: 1.04–1.25, p = 0.004; Figure 3(b)) with significant heterogeneity (p for Cochrane’s Q test = 0.06, I2 = 59%). Sensitivity analyses suggested that these results were not driven by either one of the included study (data not shown).

Forest plots for the associations between circulating ADMA and MACE in patients with PAD. (a) Forest plots with circulating ADMA as categorical variable (higher versus lower circulating ADMA); (b) forest plots with continuous ADMA as categorical variable (every increment of 0.1 µmol/l of ADMA). ADMA: asymmetric dimethylarginine; MACE: major adverse cardiovascular event; PAD; peripheral arterial disease.
Publication bias
The publication bias for the current meta-analysis was difficult to estimate because only six studies were included. The funnel plots seemed to be symmetrical on visual inspection for both the meta-analyses with ADMA as a continuous variable and the all-cause mortality (Figure 4(a)) and MACE risks (Figure 4(b)). These were consistent with the results of the Egger’s regression tests which suggested no significant publication bias for the above meta-analyses (p = 0.47 and 0.38, respectively).
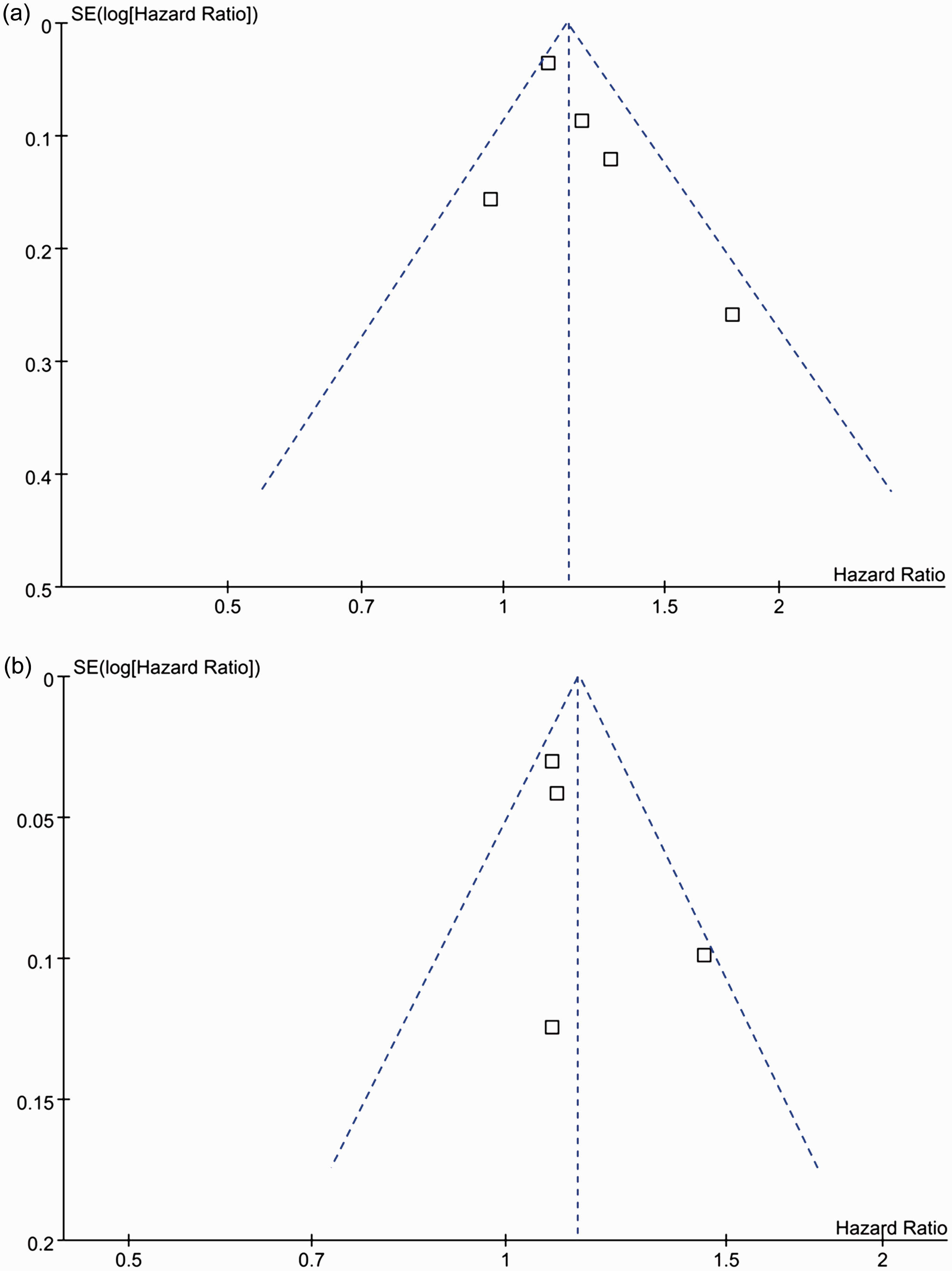
Funnel plots for the associations between every increment of 0.1 µmol/l of ADMA and the risk of all-cause mortality (a) and MACE (b). ADMA: asymmetric dimethylarginine; MACE: major adverse cardiovascular event.
Discussion
In this meta-analysis, by pooling the results of all available prospective cohort studies, results of our meta-analysis suggest that PAD patients with higher circulating ADMA at baseline are associated with significantly higher risk for the incidence of all-cause mortality and MACE. Specifically, an increment of 0.1 µmol/l of ADMA at baseline is related to 18% higher risk for all-cause mortality and 14% higher risk for MACE in PAD patients. These results suggest that circulating ADMA may be an important predictor for the poor clinical outcome in patients with PAD.
Our results were consistent with previous studies which showed a significant correlation between circulating ADMA and the severity and prognosis in patients with atherosclerosis. In a previous meta-analysis of 6168 participants, circulating ADMA was found to be positively correlated with the carotid intima-media thickness, 27 suggesting that ADMA may also be applied as a marker of the extent of subclinical atherosclerosis. Moreover, increased circulating ADMA was found in patients with CAD regardless of their clinical manifestations. 11 Subsequent meta-analyses consistently indicated that higher baseline circulating AMDA is associated with higher risk for cardiovascular events and mortality in patients with or without cardiovascular diseases at baseline.14,15,28 However, to the best of our knowledge, none of the previous studies focused on patients with PAD. Results our study further confirmed the predictive efficacy of circulating ADMA for subsequent cardiovascular events and deaths by combing the evidence from available prospective cohort studies. Results of our study have strengths in that only prospective cohort studies were included. Therefore, a temporal association between increased ADMA and subsequent incidence of cardiovascular events could be established. Moreover, we combined the data of the most adequately adjusted odds, which excluded the potential confounding factors to the most extent. The molecular basis underlying the prognostic role of increased circulating ADMA in patients with PAD may largely be explained by the potentially reduced NO bioavailability in these patients. 29 These results could be also confirmed by previous studies which demonstrated the predictive efficacy of other markers of endothelial function, such as flow-mediated vascular dilation, 30 in patients with PAD.
Our study also has limitations which should be considered when interpreting the results. First, limited numbers of studies were available, and the individual-patient-based data were not available for current analysis. Therefore, we were unable to explore whether the association between higher baseline circulating ADMA and poor prognosis is consistent in PAD patients with different clinical stages, with different comorbidities (such as those with or without DM), or receiving different treatments. Further studies with adequate sample sizes are needed. Second, as inherited with observational studies, we could not exclude the possibility for the existence of residual factors that may confound the association between higher baseline circulating ADMA and poor prognosis in patients with PAD, such as the influence of dietary factors including the intake of omega 3 polyunsaturated fatty acids.
31
Moreover, since our study is a meta-analysis of observational studies, results of our study did not support a causative relationship between increased circulating ADMA and higher incidence of cardiovascular events in these patients. Randomized controlled trials (RCTs) are needed to confirm whether interventions targeting ADMA lowering could improve clinical outcomes in PAD patients, although mixed results were yielded for RCTs with
In conclusion, our meta-analysis indicated that higher circulating ADMA at baseline may be associated with higher incidence of cardiovascular events and mortality in patients with PAD. Whether interventions targeting ADMA lowering in PAD are associated with improved clinical outcome deserve further investigation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.