
Abstract
Objectives
Endovascular procedures are the treatment of choice in cases of intrahepatic fistulas. Arterio-biliary fistulas are the rarest and most difficult to treat, due to high risk of infection.
Methods
Eight cases of persistent hemobilia that developed as a result of arterio-biliary fistulas are presented. Five cases developed as a result of iatrogenic injury, two cases as a result of chronic infection, one case as a consequence of trauma.
Results
Patients were treated using endovascular embolization or combined endovascular and endoscopic biliary tract revision. The results were monitored after six to seven days and one month after embolization. The embolizations were considered effective in all cases. One patient had four asynchronous fistulas requiring separate treatments sessions. Four patients required a revision of their biliary ducts after embolization and restoration of patency. In one patient, a migration of the coil to biliary ducts occurred.
Conclusion
Endovascular treatment of arterio-biliary fistulas is safe and effective. The use of embolization with soft and biodegradable materials like histoacrylic glue or thrombin may be the optimal method of treatment in comparison with coils which have a risk of migration or chronic infection.
Introduction
Arterio-biliary fistulas are very rare complications of surgery, trauma, and inflammation of biliary tract. 1 Because of extreme rareness, the basic principle in diagnosing this pathology is remember about hemobilia.
An endovascular procedure is the treatment of choice in cases of intrahepatic, arteriovenous, portosystemic, and arterio-biliary fistulas.1,2 However, such procedures have a risk of emboli and/or infection, especially in the case of biliary tract fistulas with concomitant inflammation.3–5 Eight cases, collected during nine years, of arterio-biliary fistulas treated with endovascular embolization are presented. The aim of the study was to evaluate the effectiveness and safety of endovascular treatment based on the materials used and etiology of the fistula (inflammatory/traumatic).
Methods
Material consists of eight patients (14–75 years) who underwent endovascular treatment due to arterio-biliary fistulas in two academic hospitals in the years 2005–2014. In one patient, four metasynchronous fistulas were observed. The most common cause of fistula (5/8 cases) was iatrogenic trauma (cholecystectomy, liver biopsy, or percutaneous biliary drainage), in one case the fistula was observed following a traffic accident complicated with a liver rupture. In two cases, the cause was infection of the liver (result of cholangitis, and as hematogenous spread of endocarditis-case for recurrent of four different supply metasynchronous fistulas). The diagnosis of bleeding into the biliary tract based on endoscopy was then evaluated by USG and/or angio-CT. The right branch of the hepatic artery (7/8 cases) was most often involved. Radiological findings include the presence of a small aneurysm on the course of the vessel with a diameter of 3–35 mm with a small mural thrombus, widening of the biliary tracts with swelling of the hilum structures, and soft tissue deposits in the lumen of the biliary tracts (Table 1).
Materials.
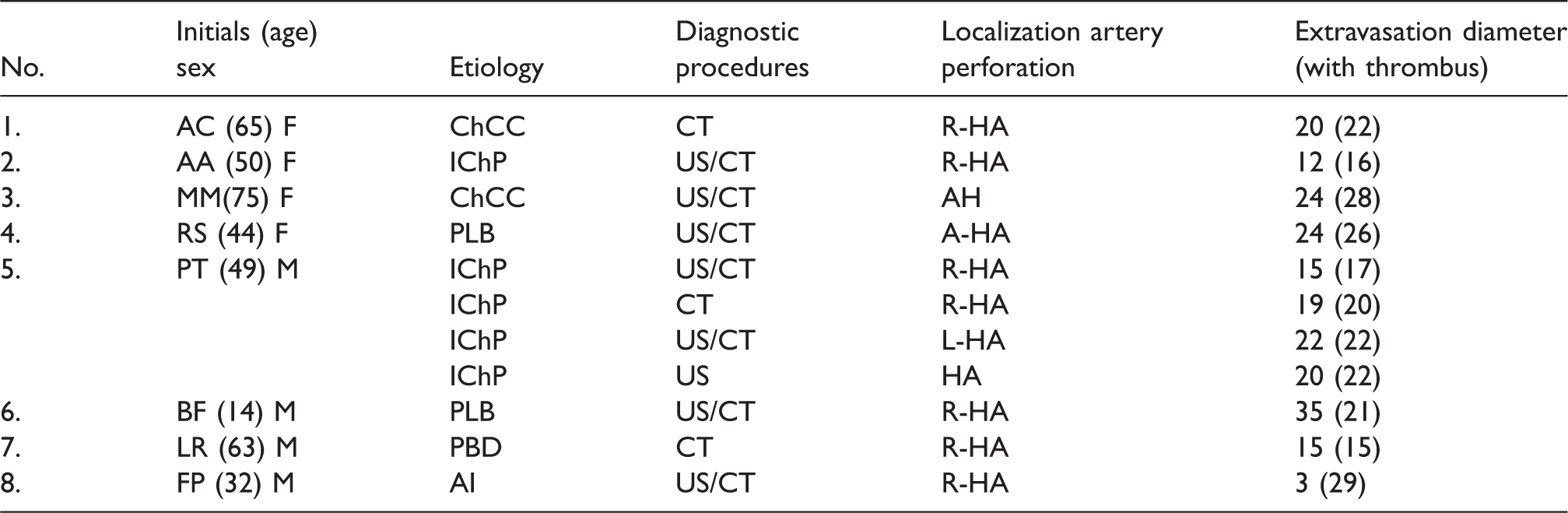
ChCC: cholecystectomy; IChP: infectious cholangiopathy; PLB: percutaneous liver biopsy; PBD: percutaneous biliary drainage; AI: accidental injury; HA: main trunk proper hepatic artery; R-HA: right branch of the hepatic artery; L-HA: left branch of the hepatic artery; AHA: additional hepatic artery.
The results of treatment were monitored six to seven days after embolization, and one month after the procedure with an ultrasound examination (Vivid 7, Logiq 5 or 7, GE, Waukesha, USA) and/or CT (LightSpeed 64 VCT or LightSpeed 16, GE). Intravenous contrast agent in a volume of 1.5 ml/kg, bolus 4 ml/s was administered (Ultravist 370 mg I/ml, Bayer AG, Leverkusen, Germany, or Yomeron 400 mg I/ml, BRACCO, Milan, Italy). The effectiveness of the embolization was evaluated by the lack of extravasation from the operated artery and the bile duct condition (presence of widening). Embolization material selection was dependent on the material availability and the operator’s assessment. Various detachable coils were used: MDSH 5 × 5, 5 × 10, 5 × 15 MDSJ 4 × 20, 6 × 40 (BALT, Montmorency, France), Tornado 18S-5 × 2, 18S-6 × 2 (Cook Medical, Bloomington, IN, USA). Microplex 18 6 × 12 (Microvention, Tustin, CA, USA). Other embolization materials were used off-label. Embolization was performed using polyvinyl alcohol (PVA, Cook Medical) and other (Histoacryl B Braun, Bethlehem, PA, USA) and Trombin 400 (Biomed, Lublin, Poland).
Results
A total of 8 patients underwent 11 embolization procedures (patient with endocarditis had 4 therapeutic sessions for recurrent fistulas). In three out of the eight procedures, endovascular embolizations were performed using three to six coils. In five out of the eight procedures, embolization was performed using PVA and embolization coils (from one to two) which were implanted in the final phase. In remaining three procedures, only soft material was used (two histoacrylic glue and one thrombin) (Table 2). Endovascular embolizations in three cases with coils have been proved to be technically effective in all cases (confirmation of cessation of the pseudoaneurysm on the final angiogram, as well as on proposed follow-up). In five patients where embolization was performed using PVA and coils, treatments have proved to be effective also in all cases.
Results.
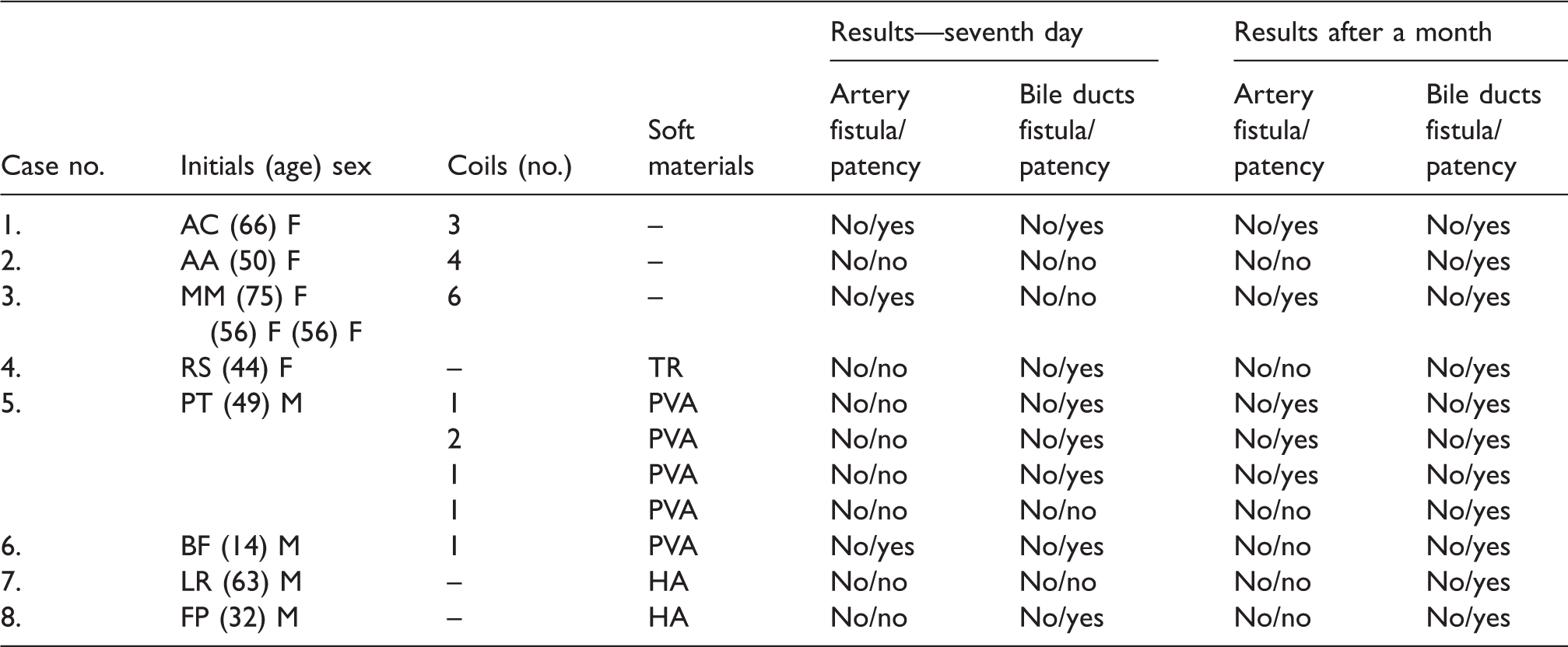
TR: thrombin; PVA: polyvinyl alcohol 7500–1000 μg; HA: histoacryl glue.
Endovascular treatment was performed by injection of PVA and coils and subsequent relapse after eight weeks was treated with endovascular re-injection of PVA and coils (case 5). It must be emphasized that every time the source of the fistula’s vasculature was different (Figure 1a to c). Therefore the embolizations have to be considered effective due to the established assessment protocol (seven days and a month after the procedure). In the remaining three cases only non-mechanical embolizations were performed: one patient was treated with thrombin, and two patients with histoacrylic glue (all procedures were also effective). At follow-up, four patients after embolization with coil and histoacrylic glue (cases 2, 3, 5, and 7), required a revision of their biliary ducts and restoration of patency by rinsing and/or papillotomy for surging clots caused the occurrence of clinically significant cholestasis (Table 2).
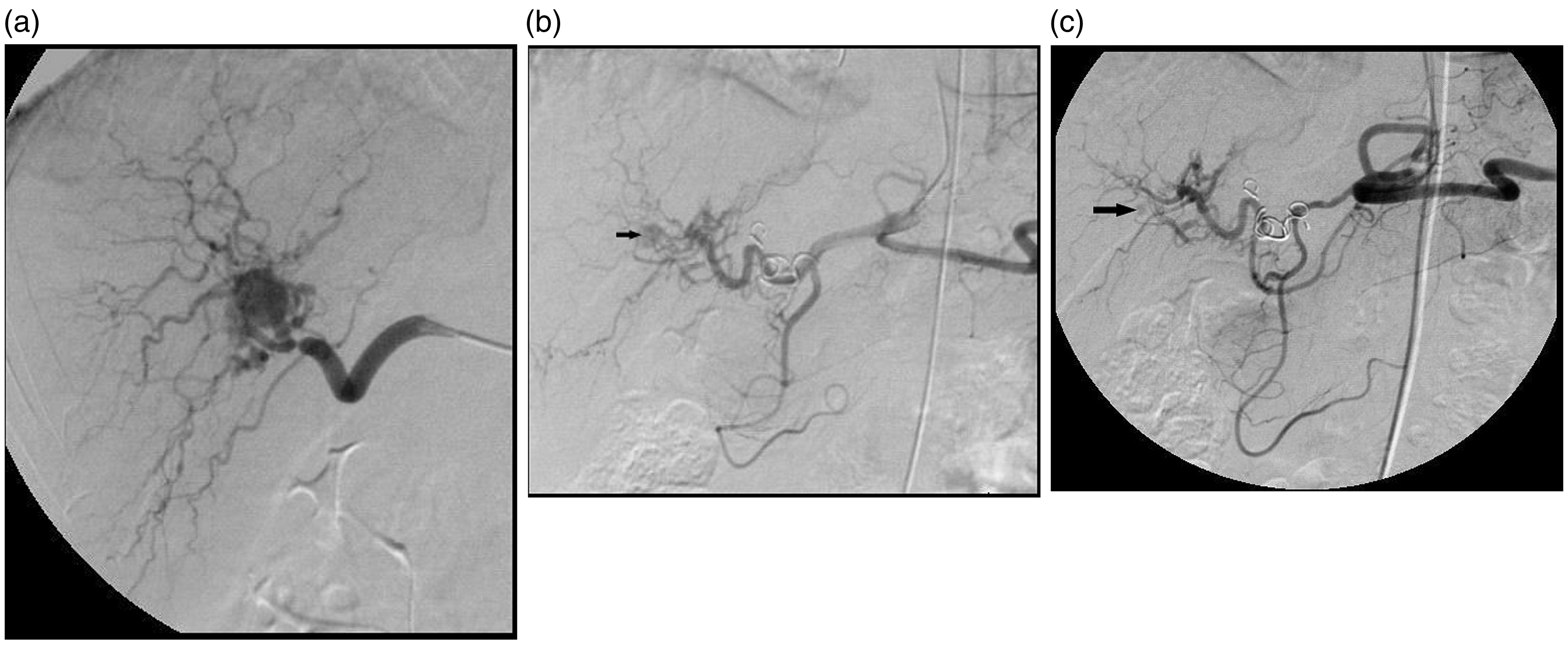
(a) Male patient, P.T., diagnosed for stenosis of aortic valve with the bacterial endocarditis. Loss of appetite, fever as well as bloody vomiting were observed. Arteriography demonstrated in the right lobe of the liver an 15-mm aneurysm within the right hepatic artery, with the rich sinuous vessels surrounding the lesion (inflammatory reaction?). The selective embolization of the supplying vessel was carried out with the use of polyvinyl alcohol (PVA) of 1500 gradation and it was ended in the implantation of two coils. (b) After five weeks a relapse of symptoms occurred (pain sensations, bloody vomiting, and diarrhea) that required blood transfusion. Arteriography demonstrated occlusion of the right hepatic artery by metal coils. The developed collateral circulation to the vessels of the right lobe and filling up of the aneurysm lumen (arrow). The second embolization was performed, similarly to the previous one with the use of PVA-1500 which ended in the implantation of the coil into the left hepatic artery, distal to the origin of gastroduodenal artery. (c) The symptoms of hemobilia reoccurred after four months. Angiography revealed a new picture—the development of a collateral circulation between the widened left gastric and superior pancreatic artery and low reaction of the aneurysm to the contrast medium. The above vessels were closed with PVA-1500. Hemobilia and pain withdrew. Occlusion of the right hepatic artery distally from the origin of the gastroduodenal artery. Trace reaction of the aneurysm (arrow).
Discussion
The common causes of acquired intrahepatic fistulas include direct trauma and iatrogenic complications (liver biopsy, percutaneous cholangiography, biliary tract drainage, endoscopic procedures involving the biliary tract, complications of cholecystectomy).1,4 The treatment of choice for intrahepatic aneurysms and fistulas is endovascular embolization of the bleeding vessel, irrespective of the cause.3–5 Aneurysms and pseudoaneurysms of the visceral arteries have been successfully treated using coronary stent-grafts. Such treatment can maintain the patency of vessels.6–8 At present, surgical artery ligation and resection of the liver is performed only in cases where endovascular treatment is not successful. 9 The cause of this complication is vessel injury, as well as bile leakage with potential subsequent infection. Bile has a toxic effect on vessel walls, a negative effect on tissue healing and the incorporation of the implanted material.4,5 The prevalence of such post-surgical complications in patients with bile extravasation involving vessels is estimated at 4%. 4 It is very important to avoid implant infection in cases of fistulas involving structures other than vessels.4,10 In each of the above cases, bleeding from the biliary tract was successfully controlled using an endovascular embolization procedure. In four of the eight patients, the most probable cause of vessel damage was the presence of decubitus calculi, a consequence of chronic biliary tract inflammation. Eight of the 11 fistulas were located distal to the porta hepatis, therefore any surgical intervention would have been difficult and would have required resection of the liver. The order in which various treatment procedures were carried out is of note: embolization, biliary tract revision, and deposit removal. The presence of a deposit in the proximal segment of the common biliary tract and associated inflammatory edema reduced the intensity of bleeding. Removal of such a deposit prior to dealing with an aneurysm and fistula may have resulted in massive hemorrhage. Endovascular embolization was a safe, effective and in these cases, a life-saving treatment. To date, the use of stent-grafts in the treatment of arterio-biliary fistulas has not been documented. Adequate stent-grafts that could have been potentially used were not available during the above procedures. However, it can be assumed that their use could have been effective in these cases. 8 Although the primary treatment was endovascular embolization, this had to be complemented with an endoscopic procedure in each case, in order to re-establish the normal bile flow that had become hindered by the migration of the embolization coil. The use of stent-grafts reduces the possibility of implant migration, albeit their use increases the risk of infection from the biliary tract.
Conclusions
Endovascular treatment of arterio-biliary fistulas is a safe, effective, and life-saving procedure. The treatment of arterio-biliary fistulas requires multi-disciplinary cooperation between surgeons, radiologists, and clinicians skilled in endoscopic procedures. As shown, soft and biodegradable materials used for embolization (thrombin or histoacrylic glue) are the most effective and safe.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.