Abstract
Introduction
Guidelines have been recommending the use of arteriovenous fistula among the hemodialysis population, but no clear conclusion has emerged with regard to the adequate access type in octogenarians. In this paper, the outcomes of arteriovenous fistula in octogenarian cohort were presented for death-censored cumulative patency rate, complications, and patients’ survival rate.
Methods
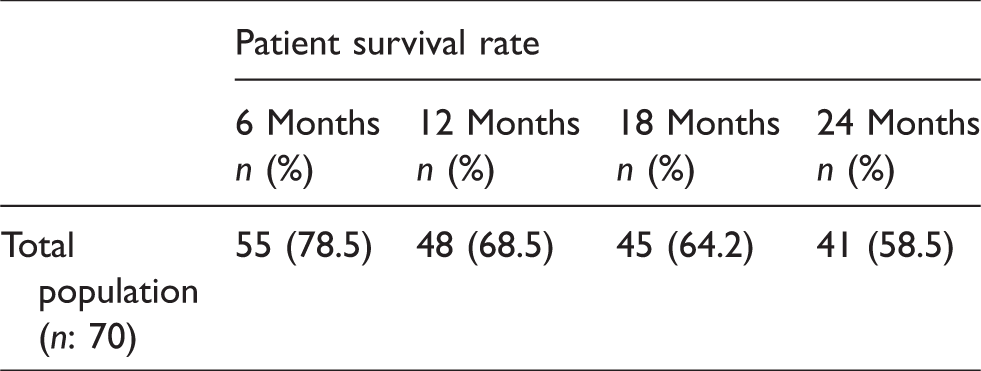
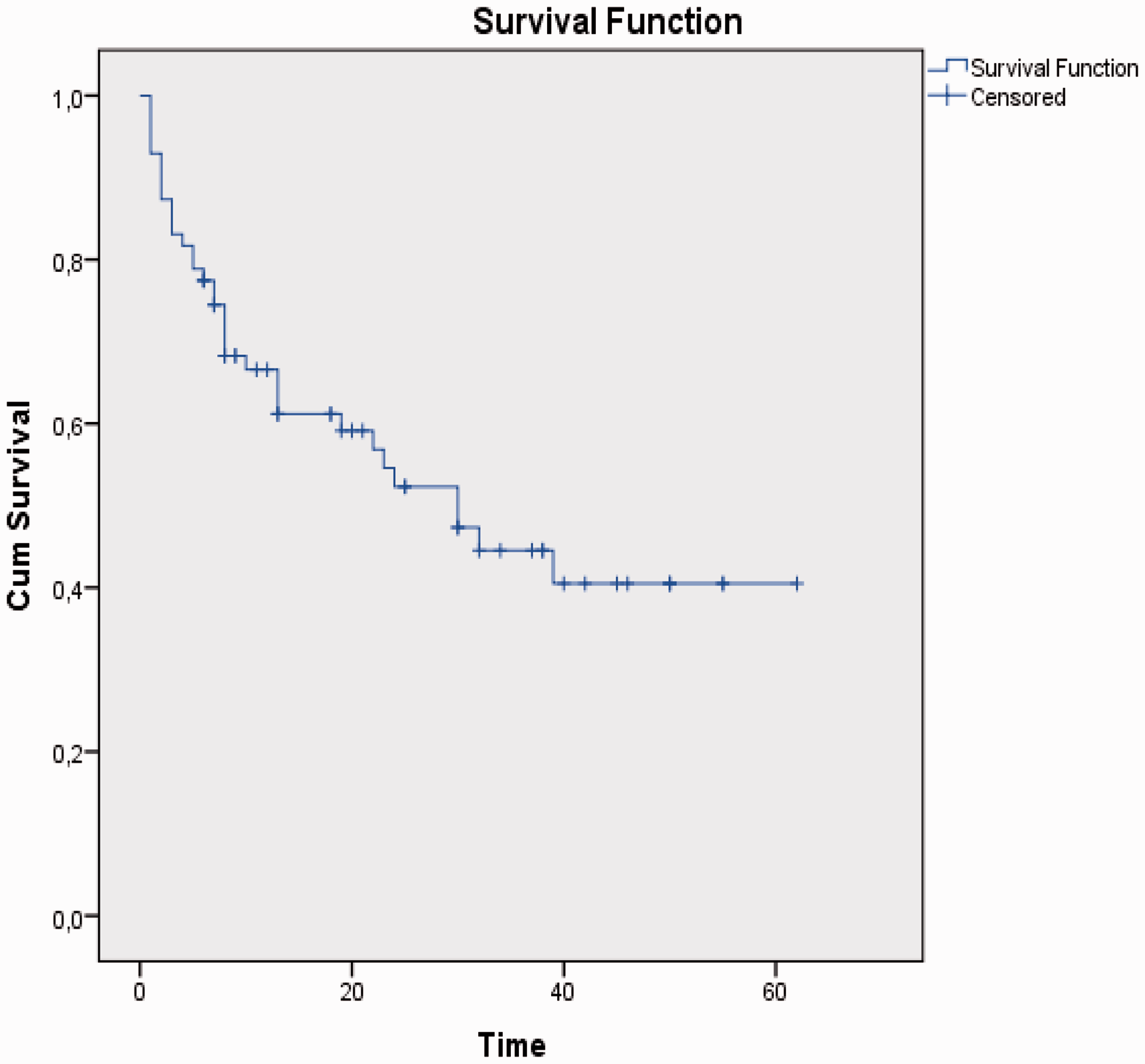
A retrospective review of 88 consecutive arteriovenous fistula interventions in 70 octogenarian patients were performed at one referral institution between January 2010 and June 2014. The patients’ records were analyzed and postoperative complications were documented. Death-censored cumulative arteriovenous fistula patency rates were calculated, and Kaplan–Meier method was used to analyze patient survival for 24 months.
Objective
The hemodialysis (HD) population has been growing increasingly around the world and this is partly due to the rising age of patients with end-stage renal disease (ESRD). Although the guidelines recommend arteriovenous fistula (AVF) as the preferred vascular access for all hemodialysis population, some questions arise about AVF creation in elderly, especially octogenarian, population. 1
AVF has pointed out better patient survival in elderly hemodialysis population when compared with catheters and arteriovenous grafts, and also cumulative patency rates have been found to be so similar with younger patients in some studies.2–4 In contrast, conflicting results have been reported, suggesting that the elderly ESRD patients have lower AVF cumulative patency and higher primary failure rates secondary to increased comorbidities. 5
Apart from that, survival expectancy is another issue in the planning of a vascular access. Older patients with ERSD have multiple comorbidities associated with poor survival; so, older age has been accepted as one of the principal factors limiting patient referral for AVF creation by some nephrologists.6,7
The aim of this retrospective study was to investigate the AVF cumulative patency and patient survival rates and also to determine the complications in octogenarian patients with ESRD.
Methods
Study design and population
In the period January 2010 to June 2014, 88 AVF interventions were performed on 70 octogenarian patients with ESRD at a single referral center. Preoperative demographic characteristics were obtained from the hospital patient records. Two-year cumulative AVF patency and patient survival data were noted by outpatient clinic records and telephone calls. The study was approved by the Ethics Committee and was exempted from obtaining patient consent.
Preoperative planning and surgery
Color-coded Doppler ultrasound assessment was performed for each individual preoperatively. Forearm and upper arm veins were examined with a 5 cm blood pressure cuff inflated to 60 mm Hg for at least 3 min. Native AVF was constructed only if the vein was dilated to a minimum diameter of 2.5 mm and target artery (radial or brachial) diameter was evaluated as 1.7 mm or more. If all these criteria were not met, the patient was referred for other vascular access options.
Draining veins and feeding arteries were also examined for stenosis. If stenosis of >50% in veins and arteries or arterial peak systolic velocity ratio of >3 for the narrowed segment and calcified arteries were present on Doppler ultrasound, the patient was not suggested as a candidate for fistula creation.
Operations were performed by the same vascular surgeons (CK, TK) under regional anesthetic block or local anesthesia with heparinization, with one-day hospitalization as ambulatory procedure. All anastomosis were constructed as end-to-side configuration.
Definitions
Cumulative patency was defined as the total of primary and secondary patency: the interval from the time of AVF placement until access abandonment including all surgical and percutaneous salvage interventions. Primary failure was defined as failed fistula function either immediately or within a few days after construction. AVF maturation was assessed as one that could be cannulated and could support a dialysis of blood flow of at least 350 mL/min without recirculation or by sonographic findings with a draining vein measuring at least 4–6 mm in diameter with a depth no greater than 5–6 mm and blood flow of 500–600 mL /min.
Follow-up
All patients were followed routinely by physical examination and by Doppler ultrasound if necessary. In case of detected delayed maturation, Doppler ultrasound findings of hemodynamically significant stenosis, clinical signs of failing access, difficulties in achieving hemostasis after the withdrawal of needles and non-efficient renal replacement therapy percutaneous or surgical interventions were considered for salvage of the fistula.
Follow-up telephone calls and outpatient clinic data were used to evaluate the patient survival rate. One patient with brachiobasilic vein transposition and patients who lost to follow-up were excluded from the study.
The endpoints of the study were primary failure, death-censored cumulative patency and patient survival rate for 24 months.
Statistical analysis
Findings were recorded in a spreadsheet (Microsoft Office Excel 2003; Microsoft Corporation, Redmond, WA). Statistical analysis was carried out with Excel and Prism statistical software (Prism v 3.0; GraphPad Software Inc., San Diego, CA). Kaplan–Meier survival curves were used to estimate patient survival.
Results
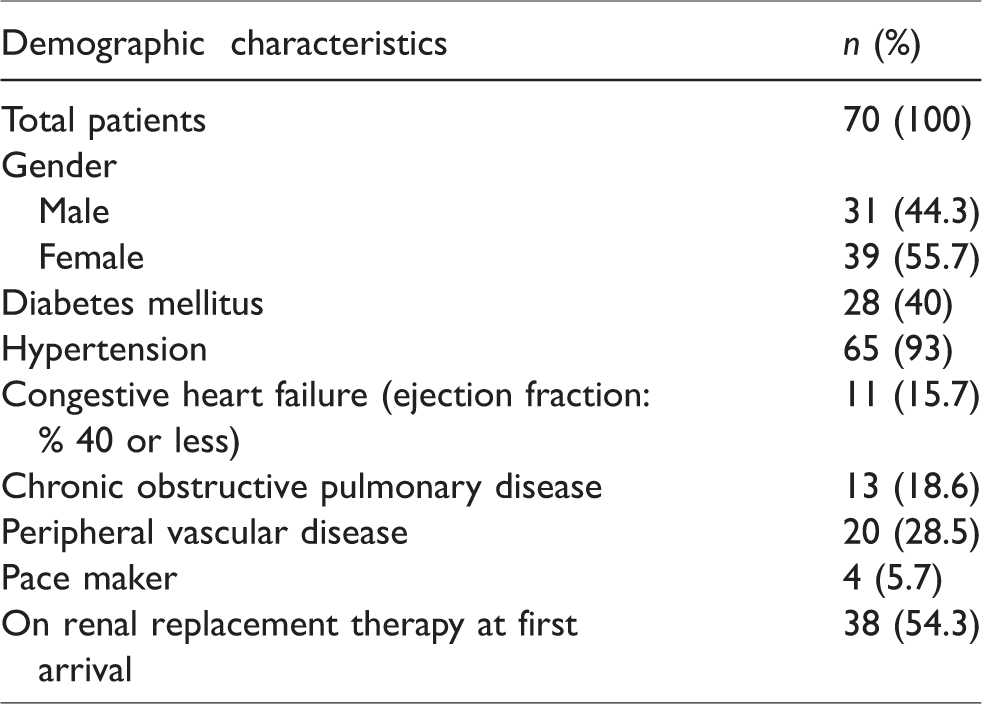
Eighty-eight AVF interventions were attempted in 70 octogenarian patients. The mean age was 83.4 ± 2.3 years (median: 85 years; range: 80–95 years) and 39 (55.7%) were female. Twenty-eight (40%) patients had diabetes mellitus and 65 (93%) hypertensive disease. Thirty-eight (54.3%) patients were on renal replacement therapy (RRT) with a catheter at initial admission. The demographic parameters of the cohort are given in Table 1.
Demographic characteristics of the octogenarian patients.
Fourteen patients had two and 4 patients had three attempts for arteriovenous fistula construction after primary failure. Totally six salvage interventions were performed with success: three percutaneous transluminal balloon angioplasties, two graft interposition for stenotic segment, and one aneurysm repair procedure. Fifty-four (61.3%) forearm and 34 (38.7%) upper arm fistulas were constructed. Forearm radiocephalic fistulas were located as 31 distal, 15 mid, and 8 proximal sites. Thirty-four upper arm fistulas were located as brachiocephalic site (Table 2).
Death-censored cumulative patency rate and primary failure rate of arteriovenous fistulas in octogenarians.
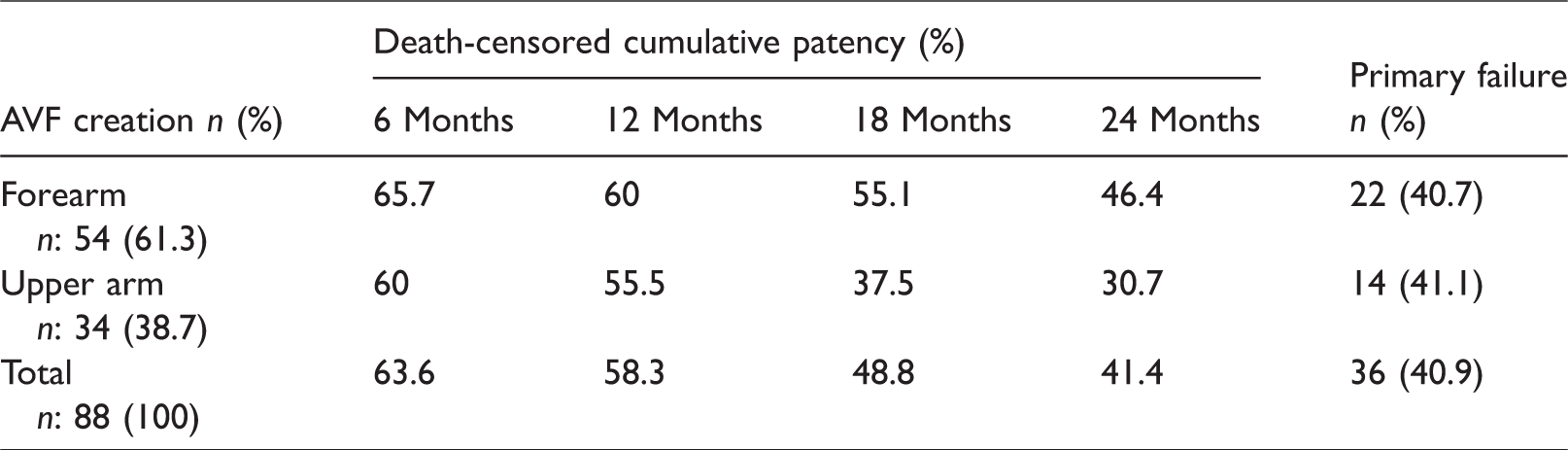
The 54 forearm fistulas had a 6-, 12-, 18-, and 24-month death-censored cumulative patency of 65.7%, 60%, 55.1%, and 46.4%, respectively. The 34 upper arm fistulas had a 6-, 12-, 18-, and 24-month death-censored cumulative patency of 60%, 55.5%, 37.5%, and 30.7%, respectively. All types of fistulas had a 6-, 12-, 18-, and 24-month death-censored cumulative patency of 63.6%, 58.3%, 48.8%, and 41.4%, respectively (Table 2).
The primary failure rate was 40.7% for forearm, 41.1% for upper arm, and 40.9 for all fistula types (Table 2).
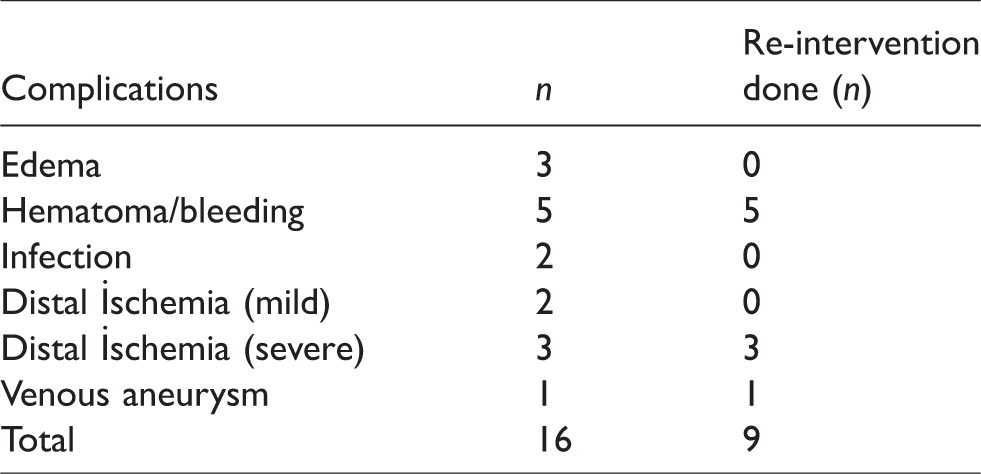
There were 16 complications determined during the follow-up time; three patients had edema, five had post-operative hematoma/bleeding that require re-intervention, two had infection that healed up with antibiotics, two had mild distal ischemia that not need any intervention, three had severe distal ischemia and end up with the closure of the fistula, and one had venous aneurysm that required surgical repair (Table 3).
Complications occurred in octogenarians during the two-year follow-up.
| Complications | n | Re-intervention done (n) |
|---|---|---|
| Edema | 3 | 0 |
| Hematoma/bleeding | 5 | 5 |
| Infection | 2 | 0 |
| Distal İschemia (mild) | 2 | 0 |
| Distal İschemia (severe) | 3 | 3 |
| Venous aneurysm | 1 | 1 |
| Total | 16 | 9 |