
Abstract
Objective
Buerger’s disease is one of the worst diseases causing peripheral artery occlusions (especially lower extremity) with increased morbidity and mortality. Endovascular treatment of the diseased arteries gains preference over bypass surgery nowadays. Here, we aimed to present the clinical outcomes of 16 consecutive Buerger’s disease patients underwent extended endovascular recanalization which is a new technique to restore direct blood flow to at least one foot artery, with the performance of angioplasty for each tibial and foot artery obstructions.
Methods
A total of 16 consecutive patients with confirmed diagnosis of Buerger’s disease that percutaneously treated in our center between February 2014 and March 2018 were included in the study. The mean age of the patients was 44.25 ± 4.28 ranging from 36 to 50 years. After physical examination and complementary diagnostic tests, performance of extended angioplasty for occluded arteries was intended to restore direct blood flow to at least one of the blow-the-knee arteries.
Results
A successful extended endovascular treatment was performed in 20 of 22 limbs, achieving a technical success of 91%. All patients were successfully discharged without any complication. Mean follow-up duration was 21.43 ± 7.08 months. Reintervention was performed in one patient and minor amputation was needed in one of the failed limbs. Limb salvage rate was 100%. A significant difference was observed based on Rutherford classification, ankle brachial index, direct blood flow to foot, presence of ulcer and rest pain when compared before and after the intervention.
Conclusion
We showed successful extended endovascular recanalization of Buerger’s disease patients with a high technical success rate and sustained clinical improvement. Extended endovascular recanalization could be a therapeutic option in Buerger’s disease patients, since they are not good candidates for surgery.
Introduction
Buerger’s disease (BD), which is also known as thromboangiitisobliterans (TAO), is a non-atherosclerotic, segmental, inflammatory, episodic, non-destructive, thrombotic and occlusive disease of unknown origin compromising small- to medium-sized distal arteries, veins and nerves. 1 Heavy tobacco consumer young men are more prone than any other subgroups of population. It usually starts before 40 to 45 years with claudication of extremities resulting ischemia of the distal small arteries and veins of legs, feet, arms and hands.
The exact pathophysiologic mechanism of Buerger’s disease is yet to be described; however, hypersensitivity to type I and III collagen have been shown with the presence of anti-collagen and anti-elastin antibodies. 2 The diseased segment contains highly cellular thrombotic changes powered with polymorphonuclear leukocytes, microabscesses and multinucleated giant cells without calcification in the vessel wall. The adaptive mechanism to overcome this obstacle is to develop a rich typical subcutaneous network of collaterals, usually named as “corkscrew collaterals”. 3
Intravenous iloprost, 4 calcium channel blockers, 5 intermittent pneumatic compression, 6 intramuscular vascular endothelial growth factor (VEGF) injections, 7 intramuscular bone morrow mononuclear cell implantation, 8 immunoabsorption therapy, 9 stimulating angiogenesis using Kirschner wire into medullary canal of the tibia, 10 bosentan 11 and cilostazol 12 are used or experimental medical therapies for TAO, though smoking cessation is the sole definitive therapy. Besides, surgical revascularization could be an option for only a few cases, since the distal runoff vessels available for bypass surgery is lacking. 13 The aggressive involvement of distal vasculature makes surgery technically challenging, with low feasibility and patency rates. 14
The present study aimed to demonstrate the feasibility, safety and effectiveness of extended percutaneous transluminal angioplasty (PTA) in Buerger’s disease patients with critical limb ischemia (CLI).
Method
Patient population and evaluation
A total of 16 (all the patients were male and mean age was 44.25 ± 4.28 years ranging 36 to 50 years) TAO patients treated percutaneously in our center between February 2014 and March 2018 were enrolled to the study. Twenty-two limbs were presented with CLI, while 1 of them was with major tissue loss and 16 of them were with minor tissue loss or ulceration.
All patients diagnosed as TAO were selected according to Olin’s 5 and Shionoya’s 15 criteria which enclose the following: (I) smoking history; (II) emerge before the age of 50 years; (III) presence of distal extremity ischemia as indicated by claudication, pain at rest, ischemic ulcers or gangrene, and documented by noninvasive vascular testing; (IV) exclusion of autoimmune diseases, hypercoagulable states, diabetes mellitus and toxicology such as cocaine and cannabis; and (V) exclusion of a proximal source of emboli and other non-atherosclerotic diseases.
All patients were investigated for the possibility of a hypercoagulability state (protein C and S, factor V Leiden mutation, anticardiolipin antibodies, antithrombin III, prothrombin 20210G>A mutations). Rheumatologic diseases were ruled out with an investigation of specific antibodies (antinuclear antibody, rheumatic factor, complement, cryoglobulinemia, anti-SCL-70, anticentromere antibodies, Westergren sedimentation rate and C-reactive protein). Renal function tests were assessed for the possibility of contrast-induced nephropathy (CIN) and liver functions and serologic panel studied to exclude critically ill patients. Besides these laboratory parameters, a complete blood count, fasting plasma glucose, hbA1c and thyroid function tests were performed in all the patients. Despite being interrogated carefully for the possible use of cannabis and cocaine, none of the patients admit the usage of these over the counter drugs. Nonetheless, all the patients admit the use of wrapped tobacco, since it is very common in this part of the country.
The ankle brachial index (ABI) was used for hemodynamic assessment of our patients before and after the interventions. The ABI was defined as the higher of two ankle pressures divided by the mean of two brachial artery pressures, unless right and left brachial systolic pressures differed by >10 mmHg, in which case, the higher value was used in the denominator. 16
Flow pattern of the distal arteries were investigated with Doppler ultrasonography. All the measurements were performed with an Aplio 500 Platinum ultrasound device (Toshiba Medical Systems, Japan) with high-frequency linear probe (frequency range: 5–14 Mhz). The probe was placed longitudinally to the arteries (dorsalis pedis artery and tibialis posterior). Arterial flow was confirmed with color Doppler and the flow pattern was assessed with pulsed wave Doppler. The Doppler waveform of the lower extremity arteries without significant disease is classified as a high pulsatility waveform and characterized by a triphasic flow pattern. 17 Monophasic flow pattern, on the other hand, is characterized with a damped pattern meaning slowed systolic flow acceleration, reduced peak systolic velocity and increased diastolic flow. 18 The monophasic pattern is observed at the stenotic site and the distal segment to the stenosis with a diameter reduction of more than 50%.
Diagnostic angiographic evaluation of the patients was performed after obtaining a broad anamnesis about risk factors, performing a complete physical examination and running diagnostic tests. Digital subtraction angiography (DSA) was used to evaluate the site and length of the lesion, corkscrew collaterals, 3 and distal runoff vessels.
The study is approved by the local ethics committee and written informed consent was obtained from each patient after a broad explanation of the risks, complications and benefits of the procedure. All the interventions were performed with supervision of a stand-by vascular surgeon.
Procedure details
All the procedures were performed by a single experienced operator under local anesthesia. In order to optimize angiographic details, the sum of radio opaque usage was decreased and the performance of endovascular intervention was increased. Antegrade femoral approach was used in every case which has already showed a better performance in the treatment of distal vessels of patients with wounds in previous studies.19,20 All the patients were started to dual antiplatelet therapy whenever percutaneous intervention decision was made. A 7-F femoral sheath (Super Sheath; Boston Scientific, Natick, MA) was placed to the ipsilateral groin, and intra-arterial heparin was administered at a dose of 125 IU/kg through the sheath. More heparin added in prolonged interventions aiming an activated clotting time of 250 s or more. The main aim of the interventions was to restore direct blood flow to the foot through either the dorsalis pedis artery and plantar artery or both.
Various crossing techniques were used to pass through the occluded segment of the arteries with dedicated 0.014, 0.018, and 0.035 inch guidewires. The direct catheter advancement technique over-the-wire balloon catheter, the penetration technique, the loop wire technique, the parallel wire technique, the anchor wire technique, reverse controlled antegrade and retrograde tracking (CART) technique were used to cross in total occlusions, while sliding technique was preferred in subtotal occlusions. Whenever the chosen technique fails, crossover to another technique or combination of techniques were performed for successful wire crossing. As we previously mentioned in one of our case, subintimal angioplasty was also tried as a last resort. 21 Recanalization was achieved with inflation of 1.5 to 5.0 mm balloons in diameter and appropriate length for at least 3 min. Appropriate balloon size was selected according to the angiographic measurements of the non-diseased proximal and distal vessel lumen (Figures 1 and 2). The objective was to restore direct blood flow to distal arteries with balloon angioplasty without stent placement. However, stent placement was remained as a last resort to restore blood flow in superficial femoral and popliteal arteries in dissections. The access site was restored using 8-FAngio-Seal™ STS Plus (TERUMO) in all patients.

The periphery angiography of the right lower extremity is showing a blunt total occlusion of superficial femoral artery and popliteal artery junction with grade IV “corkscrew” collaterals. There is no painted trace of anterior tibial artery, posterior tibial artery, peroneal artery and foot arch.
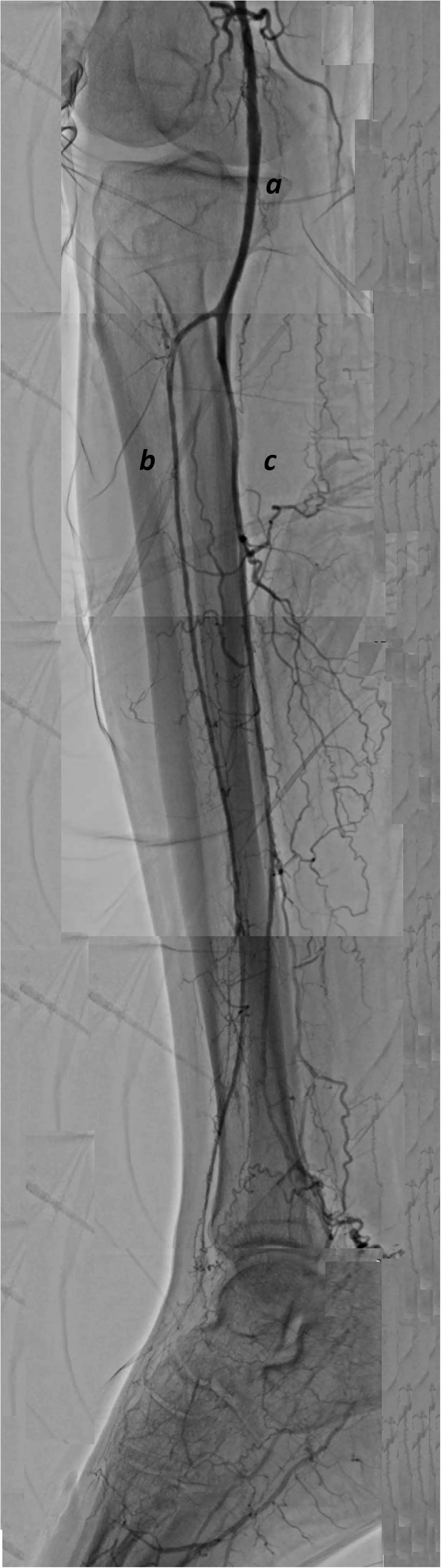
The peripheral angiography of the right lower extremity of the patient presented in Figure 1 after extended endovascular revascularization is showing popliteal artery (a), anterior tibial artery (b), and posterior tibial artery (c) clearly and the plantar arc.
The success of the intervention was assessed according anatomic, hemodynamic and clinical parameters that defined by the International Society for Cardiovascular Surgery Reporting Standard22,23:
Reestablishment of direct flow to dorsalis pedis artery or plantar artery with residual stenosis of <30% in treated arteries was accepted as an anatomical success; Subjective perception of improved walking distance, resolution of resting pain or healing of ischemic ulcer, resulting in at least one category improvement based on the Rutherford classification together with an increase in ABI was defined as clinical success; Triphasic blood flow pattern determined by Doppler USG was accepted for patency of the treated arteries.
A very strong recommendation was made to quit tobacco substances in any form of use. Acetylsalicylic acid (100 mg/day) and clopidogrel (75 mg/day) were prescribed for the first month. Acetylsalicylic acid (100mg/day) indefinitely and clopidogrel (75mg/day) for the first month were prescribed. All the patients were evaluated in the 1st, 3rd, 6th and 12th months. Pain-free walking distances, presence of CLI, wound healings, ABIs and Doppler USG results were recorded.
Definitions
Rutherford classification is a widely accepted clinical classification suggested by Rutherford et al. 24 in order to standardize reporting practices by grading the severity of chronic arterial occlusive disease.
Statistical analysis
Statistical analysis was performed with SPSS 18.0 software (SPSS Inc., Chicago, IL, USA). ANOVA was used to compare normally distributed continuous variables recorded before and after the intervention. Wilcoxon signed-rank test was used for nonparametric distributions. Fisher exact test or the chi-square (McNemar) tests were used in categorical variables when an appropriate p < 0.05 threshold was considered statistically significant.
Results
This retrospective study presents 16 TAO patients undergone PTA to lower limbs due to CLI. All patients were male and the mean age of the patients was 44.25 ± 4.28 years. One of the patient with history of previous major amputation stopped smoking one year ago, while the others were smoking tobacco products (especially wrapped tobacco) before the intervention. Two of them had hypertension while three others had a BMI more than 30 kg/m2. Coronary artery disease, diabetes mellitus and hyperlipidemia were not present in any of them (Table 1).
Demographic characteristics of patients.
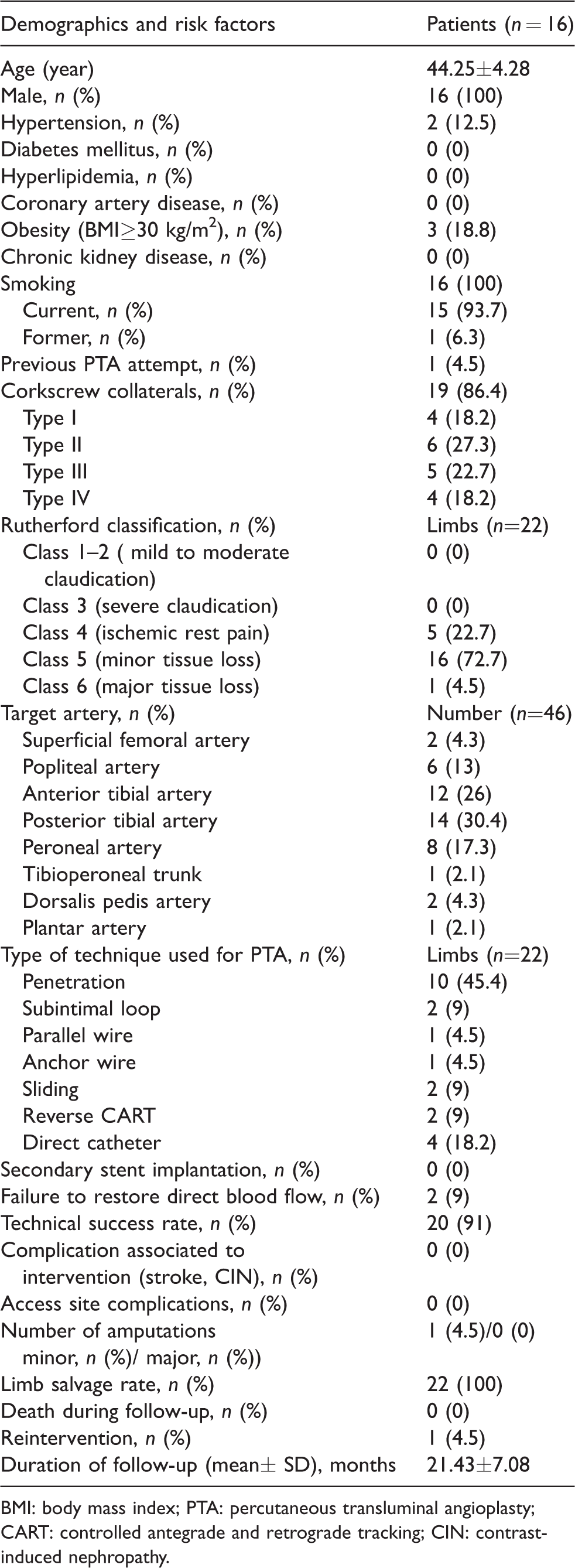
BMI: body mass index; PTA: percutaneous transluminal angioplasty; CART: controlled antegrade and retrograde tracking; CIN: contrast-induced nephropathy.
Corkscrew collaterals were present in 19 (86.4%) of the treated limbs. Four of the treated limbs had type I Corkscrew collaterals, six of them had type II, five of them had type III and four of them had type IV (Table 1).
The indication for intervention was CLI in all the treated limbs. Five of the treated limbs had ischemic rest pain (RC grade 4) (22.7%), while 16 of the treated limbs had minor skin ulceration (RC grade 5) (72.7%) and 1 of the treated limbs had major tissue loss (RC grade 6) (4.5%) (Table 1).
A total of 46 arteries were treated: 38 of them were below the knee (82.6%), 2 were superficial femoral arteries (4.3%) and 6 were popliteal arteries (13%). All the arteries were treated with PTA only, and there was no need to secondary stenting in any case. We failed to restore direct flow to distal vessels in two cases of the above-the-knee arteries (9%). One of the failed cases was previously attempted popliteal artery occlusion and the other was superficial femoral artery. Despite using various crossing technique (reverse CART also tried), we were unable to restore direct blood flow to distal vasculature (Table 1). On the other hand, we successfully restored direct blood flow to 20 limbs over 22 limbs with a technical success rate of 91% (Table 1).
All the patients were discharged safe and sound. There were no access site complication, vessel specific complication, organ specific complication (stroke, CIN) and systemic complication. During a mean follow-up of 21.43 ± 7.08 months, we observed no deaths with a limb salvage rate of 100%. However, one of our patients with failed intervention had a minor amputation (toe amputation) and another one needed reintervention (4.5%) (Table 1).
Clinical outcomes of the patients were presented in Table 2. A statistically significant decrease was observed in Rutherford Class before and after the intervention (Figure 3). ABIs were improved after the treatment. Fifteen of the 17 ulcers were healed after the intervention (around sixth month). Similarly, rest pain was resolved, and triphasic blood flow was restored in most of the patients (Figure 4). One of our patients has already stopped smoking before the intervention and nine others stopped after the intervention (in the first month) with a success rate of 62.5% (Table 2).

Rutherford classes of the patients stratified by follow-up periods. Each x-axis interval is equal to or greater than the lower limit of the interval and less than the upper limit.
Clinical outcomes of patients.


Rates of skin ulcers and rest pain stratified by follow-up periods. Each x-axis interval is equal to or greater than the lower limit of the interval and less than the upper limit. Numbers of rates are listed in Table 2.
Follow-up results
There were no mortality and morbidity in the first 30 day after intervention. Sustained clinical improvement provided in 19 of the 20 successfully treated limbs. A repeated intervention was performed to one of the below-the-knee arteries. In this specific patient, recanalization of anterior tibial artery was needed and provided at the postoperative day 27 due to ischemic rest pain. One of our failed cases with ischemic rest pain experienced pain-free interval with smoking cessation and medical management as a last resort. The other failed case (who already had ischemic ulcer at his second and third toes) had a minor amputation of the second and third toes.
Mortality and morbidity were not recorded in any cases during the 3rd, 6th and 12th month follow-ups. Sustained clinical improvement was achieved in all successfully treated limbs.
Discussion
We showed that extended endovascular intervention is feasible, safe and effective in the treatment of a consecutive series of TAO patients presented with CLI.
The gold standard to prevent disease progression and avoid amputations still is the complete cessation of cigarette smoking and/or tobacco use in any form in patients without CLI. 25 However, smoking cessation could not be achieved in the vast majority of the patients. The disease activity keeps worsening even when smoking one or two cigarettes daily, using smokeless tobacco (chewing tobacco or snuff) and nicotine replacement. 26 The amputation rate varies from 5% to 42% at Cleveland Clinics Foundation according to the tobacco use. Twenty-five percent of patients are likely to have had an amputation at 5-year follow-up while 45% at 10-year follow-up. A total amputation rate of 33%, comprising 24.4% for minor amputations and 8.6% for major amputations has been reported based on the most recent series. 27 New interventions, such as PTA, raised questions about the success of conservative (smoking cessation) treatment. On the contrary of the conservative treatment alone, we had a major amputation rate of 0(0/22) and a minor amputation rate of 4.5% (1/22) which was limited toes, in midterm follow-up with extended PTA with smoking cessation.
Antiplatelet agents to blockade thrombus formation, calcium channel blocker to overcome associated vasospasm, folic acid, pain relief with analgesics, antibiotics for superimposed infection are the supplementary medical treatment to conservative treatment. However, new therapeutic interventions are needed to restore distal blood flow and alleviate pain in critical limb ischemia besides conservative options. Lumbar sympathectomy and omental transfer were successfully performed in CLI of TAO patients. Despite owing good short-term clinical improvement and low amputation rates, the long-term outcomes and healing of ischemic ulcers stay unclear.28,29 Intramuscular gene transfer of vascular endothelial growth factor, stem cell implantation and spinal cord stimulator are newly performed interventions but there are not enough data about safety and effectiveness yet.7,30,31 Surgical revascularization is an option if the distal arterial vessel has a good segment for anastomosis and supply. Due to extensive involvement of both arteries, veins and lack of available distal vasculature surgical revascularization is very rare to be performed. It was reported only four cases of TAO patients (1.8%) over 225 were suitable and had undergone surgical revascularization in a one-year follow-up period in one study, 32 while it was reported less than 10% in other studies.33,34 At the same time, the primary patency rates were reported to be as low as 33.3% at the third year. 35 Inappropriate patient selection, technical difficulties and continuation of smoking could have played role in failure of grafts.
Endovascular interventions are taking over the other approaches in the treatment of TAO nowadays. The very first reflection of the current treatment to literature was the presentation of sporadic cases. However, in 2012, Grazini et al. 36 proved the safety, effectiveness and efficacy of endovascular treatment in 17 TAO patients with 20 CLI limbs (all the limbs were below the knee). In their study, they achieved a technical success rate of 95%, with a limb salvage rate of 100% during a mean follow-up of 23 months (standard error: ±4.05), with a sustained clinical improvement in 16 of the 19 limbs without mortality and procedure-related complication. Extended revascularization was aimed up to dorsalis pedis artery, plantar artery and foot arch in order to achieve direct blood flow as distal as possible. Our study was in harmony with this first ever study in relation of feasibility and concept. In our study, we performed extended revascularization with multiple vessel interventions in order to achieve direct blood flow at least one foot artery too. Two years later, another study 37 showed effectiveness of endovascular treatment of ‘atypical’ TAO patients. Yuan et al. showed a technical success rate of endovascular treatment of 100% in nine TAO patients with either iliac artery occlusion, femoral artery occlusion or both with PTA alone without stent placement. Similar to the previous study, all the patients were presented with CLI. A sustained clinical improvement was achieved in six patients with rest pain, and ischemic ulcers of three patients have healed three to five months after the procedure. Two superficial femoral artery occlusions and six popliteal artery occlusions were aimed to restore blood flow in our study. However, we could not recanalize one of the popliteal arteries that previously attempted and one superficial femoral artery. Similar to the study conducted by Yuan et al., none of our patients needed secondary stenting, and sustained clinical improvement was obtained in all the patients that the technique was successfully performed. A decreased Rutherford classification category, increased ABI, restored triphasic blood flow and healing of ulcers were observed. Another study showed successful PTA to upper limbs besides lower limbs. In their study, Kawarada et al. 38 treated 20 patients with 20 lower limbs and 5 upper limbs presenting with CLI (15 limbs) and claudication (10 limbs). They combined intravascular ultrasound besides various wire crossing techniques and PTA altogether to provide direct blood flow to the distal arteries and to better understand the pathophysiology of the disease. They used a combination of multiple wire crossing techniques (such as the subintimal and loop techniques, as well as the intraluminal technique) together to cross the non-atherosclerotic lesions in 21 limbs while a single technique in 4 limbs. Parallel to this study, we also used various crossing technique in combination in most of our patients owing to new guidewire technologies, sophisticated crossing techniques and complex endovascular interventions. However, there was no chance to assess the lesion characteristics with complementary imaging modalities.
Limitations
To be performed in a single center and retrospective design in nature with a relatively small sample size could be major limitation of the study. Presence of a control group of conservative treatment and surgery could have added value to the study. Finally, the angiographic evidence of patency in the follow-up is lacking.
Conclusion
Endovascular therapy with extended PTA could be feasible, safe and effective in TAO patients presenting with CLI without adequate distal vessel to bypass surgery. However, more prospective studies comparing endovascular treatment and other options in long term are needed to confirm our findings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.