
Abstract
Background
The current advancement and increasing use of diagnostic imaging has led to increased detection of abdominal aortic aneurysms (AAA). Many of these patients are unfit for elective AAA surgery.
Aim
To investigate the outcome of conservative management of unfit patients with large AAA (>5.5 cm) who are turned down for elective surgical intervention.
Patients and methods
Between January 2006 and April 2017, 457 patients presented with AAA >5.5 cm. Seventy-six patients (M: F 54:22) were deemed unfit for elective repair. Mean age was 79.8 years (range 64–96). Mean AAA size was 60.22 mm (55–83).
Results
Forty-nine of the 76 patients (64%) had died by April 2017. Fifteen (19.7%) patients died directly because of their aneurysm rupture. A further 34 (44.7%) patients died from non-aneurysm-related causes.
Conclusion
Patients with large AAA deemed unfit for elective surgery have an overall poor prognosis and die mainly from other causes than AAA. Surgical intervention when rupture occurs results in poor survival.
Introduction
The aim of elective abdominal aortic aneurysm (AAA) repair is to prevent fatal rupture. Operative intervention should be performed only if the risk of rupture outweighs the risk of surgery in patients whose life expectancy is long enough to result in long-term benefit. 1 Guidelines for elective repair of AAA tend, by necessity, to be focused on aortic size rather than patients’ general health, age and comorbidites. 2 Few studies have addressed non-operative management of patients with large AAAs (>5.5 cm) in diameter deemed to be at prohibitive risk for open or endovascular repair because of unfavourable anatomy or serious comorbidities. Much of the available information suggests a poor outcome for such patients.3,4 The turndown rates for elective AAA surgery vary widely. Data on turndown rates are important to contextualise operative morbidity and mortality. 5 The EVAR 2 Trial remains the only randomized controlled trial that has compared operative treatment versus conservative management, concluding that although fewer aneurysm-related deaths occurred in the endovascular group, compared to no intervention, there was no difference in long-term all-cause mortality.6.
Little information exists regarding the fate of patients with large AAA who are not offered surgical intervention. Published studies on AAA generally omit data on numbers of patients turned down for surgery, their survival, factors affecting survival, rates of rupture and the ultimate cause of death.
Aim
The aim of this study was to assess the outcome of conservative management of unfit patients with large AAA (>5.5 cm in size on CT scan) who are turned down for elective surgical intervention in our institution.
Patients and methods
In January 2006, a prospectively maintained database for surveillance and follow up of patients with AAA was established. The current study is a post hoc analysis of data collected from the aforementioned database.
Between January 2006 and April 2017, a total of 457 patients with unruptured infra-renal or juxta-renal AAA > 5.5 cm in maximal diameter on computerised tomography scan (CT scan) were assessed. Patients were evaluated clinically and radiographically. Patients presenting with symptomatic or ruptured AAA were excluded as well as those involving the renal or visceral vessels.
All CT scans were discussed at a vascular-radiology multi-disciplinary team (MDT) meeting. Decision regarding suitability for open or endovascular repair was recorded for all patients.
Fitness for surgery (open repair or EVAR) was determined by the anaesthetic team following assessment in the pre-operative assessment clinic. Our preassessment clinic has a predefined uniform process for assessment of all patients undergoing aortic surgery. This included a history, physical examination, 12-lead electrocardiogram and echocardiogram if indicated. Patients with particular indications underwent pulmonary function or other organ-specific testing. American Society of Anaesthesiology Classification Scale (ASA) was defined for each patient with recommendation for optimization, further consultation of other specialities and comment about the risk of intervention. Final risk assessment is given. Not only ASA grading was used but also anaesthetic consultant comments on degree of surgical risk, preoperative tests results, probability of major events and mortality and presence of major prohibitive comorbidities (as cardiovascular risks, advanced malignancy, etc.). Decision is discussed with surgical team.
Further discussion regarding management took place with the patient and family in the outpatient department where final decision is made and documented by the consultant vascular surgeon. Those patients deemed unfit for surgery were managed with best medical therapy. This comprised anti-platelet therapy, statin therapy and blood pressure management. Referral to any other medical, surgical or oncology services were ensured where applicable. The patient and accompanying family members were provided with education regarding AAA. The decision was recorded in the medical chart, electronic record and database and included a plan for management in case of rupture for patients deemed unfit for elective surgery.
Patient mortality data, including place and cause of death, were collated from the National Death Register (NDR) after obtaining required ethical approval. This is a single centralised independent register which records mortality data for the entire Irish population and is recorded prospectively.
Data collection and statistical analysis
Data were collected from a prospectively maintained AAA registry database in the Department of Vascular Surgery in St. Vincent’s University Hospital, Dublin. Further data were collected by analysis of electronic patient records on the hospital computer system. Mortality data were retrieved from the National Death Registry office.
Statistical analysis for tables was performed using Statistical Package for Social Sciences (SPSS for Windows, v.19.0; Chicago, IL, USA).
R statistical software version 3.4.0 (21-04-2017) was used to produce survival curves. [Copyright (C) 2017 The R Foundation for Statistical Computing, URL https://www.R-project.org]. p-value less than 0.05 was considered statistically significant.
Results
Two hundred and six of the total 457 patients’ evaluated (45%) patients underwent open AAA repair; 175(38.3%) patients underwent EVAR. Seventy-three patients were deemed to be at prohibitive risk for surgery because of major medical comorbidities. Another three patients were offered surgery but refused any surgical intervention despite explaining resultant risks.
A total of 76 (16.63%) patients therefore were managed conservatively. Age ranged between 64 and 96 years. The MEDIAN age was 80 years, inter quartile range was 74.75–84 years. Fifty-four (71%) patients were males and 22 (29%) were females (Table 1). Mean AAA diameter was 6.22 cm (5.5–8.3 cm). Sixty-six patients (86.8%) were deemed anatomically unsuitable for EVAR. ASA grading was used to objectively determine operative risk (Table 1).
Patients’ comorbidities, ASA grading.
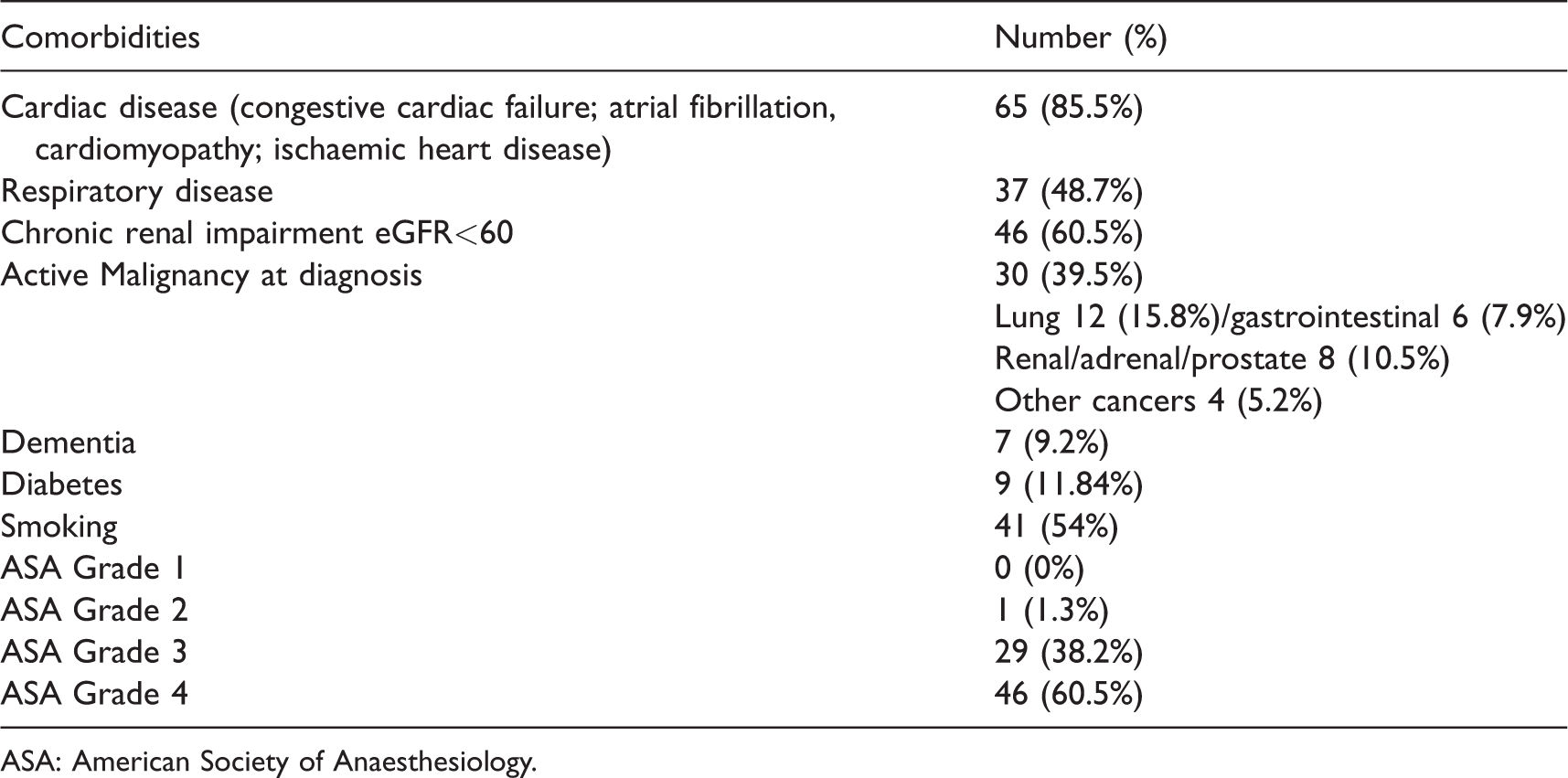
ASA: American Society of Anaesthesiology.
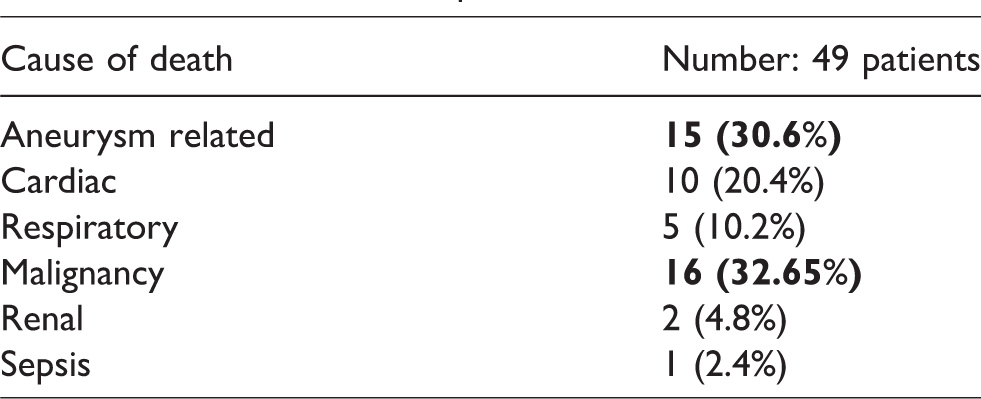
Of the 76 patients who were managed conservatively, 49 (64.5%) patients were recorded as deceased by April 2017. The mean duration of survival following diagnosis of large AAA was 24.9 months (range 1–96 months). The remaining 27 (35.5%) patients were still alive at 2 to 75 months of follow-up (mean 31.5 months). The fate of patients diagnosed with ruptured AAA in unfit patients group was very poor with only six patients received surgery and only one survivor as shown in Table 2. However, most patients (69.4%) died from non-aneurysm-related causes (Table 3).
Fate of ruptured AAA in unfit patients group.
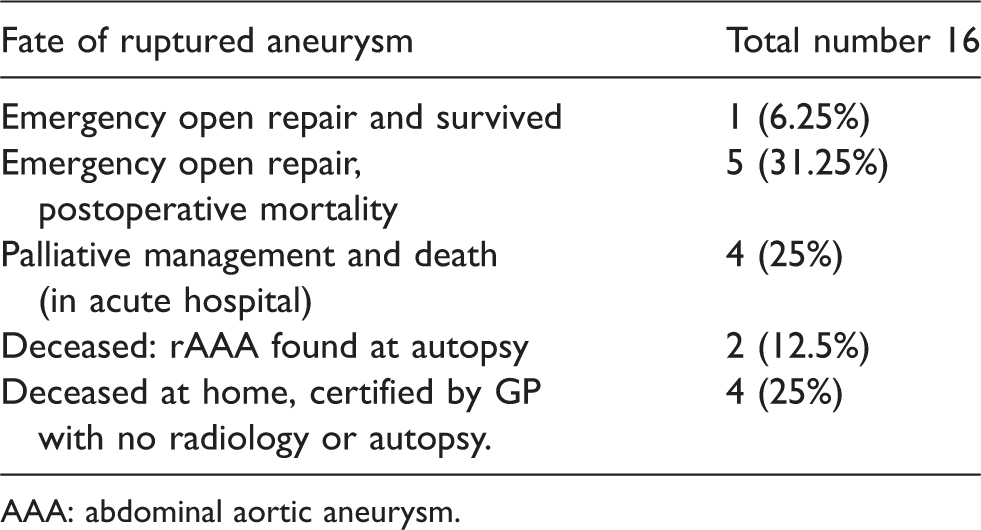
AAA: abdominal aortic aneurysm.
Causes of death in patients’ cohort.
A total of 16 conservatively managed patients (21%) suffered ruptured AAA. Six patients (37.5%) proceeded to emergency surgery of whom only one survived. All emergency repairs were performed using open surgery. None of these patients had been suitable for EVAR based on imaging at the time of first assessment or at the time of rupture. The single surviving patient had previously refused elective AAA repair despite having been deemed fit for surgery.
Neither adjusted (to other variables including cardiac, respiratory, renal disease and malignancy) nor unadjusted analysis of age at time of diagnosis of AAA had any impact on survival. No statistical difference was seen between those less than or older than 75 years old (Figure 1).
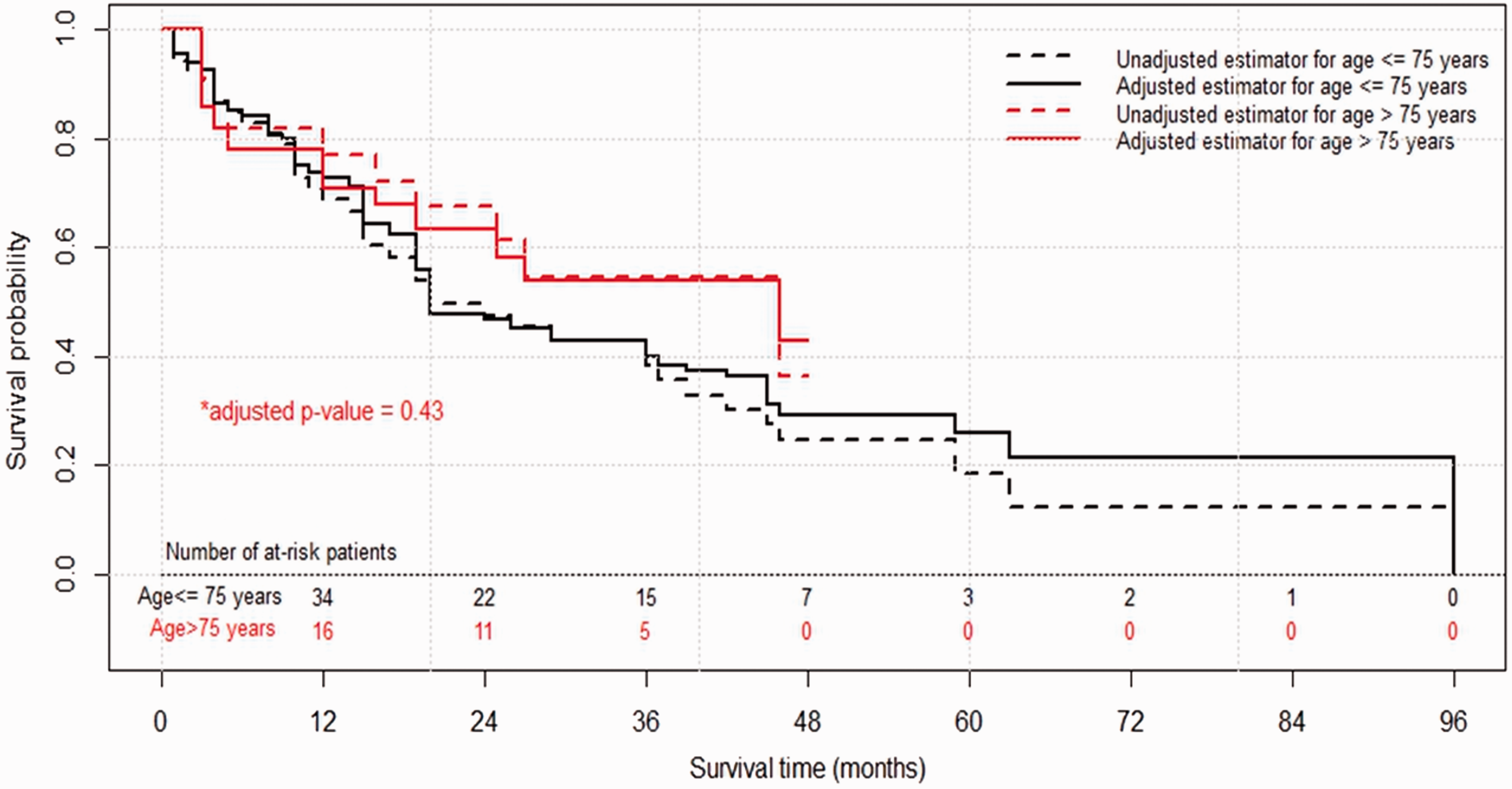
Comparison of survival rates among younger (<75 years) versus older (>75 years) patients. p value by log rank test.
Active malignancy at time of AAA diagnosis was detected in 30 (39.5%) patients. The majority of these patients died as a direct result of their malignancy. By the end of follow-up period, 21 patients with active malignancy had died, 16 (77%) from metastatic disease. Two patients (9%) died from ruptured AAA. Patients with active malignancy diagnosed with large AAA and managed conservatively had a significantly worse outcome than the remainder of the conservatively managed group without malignant disease (Figure 2).
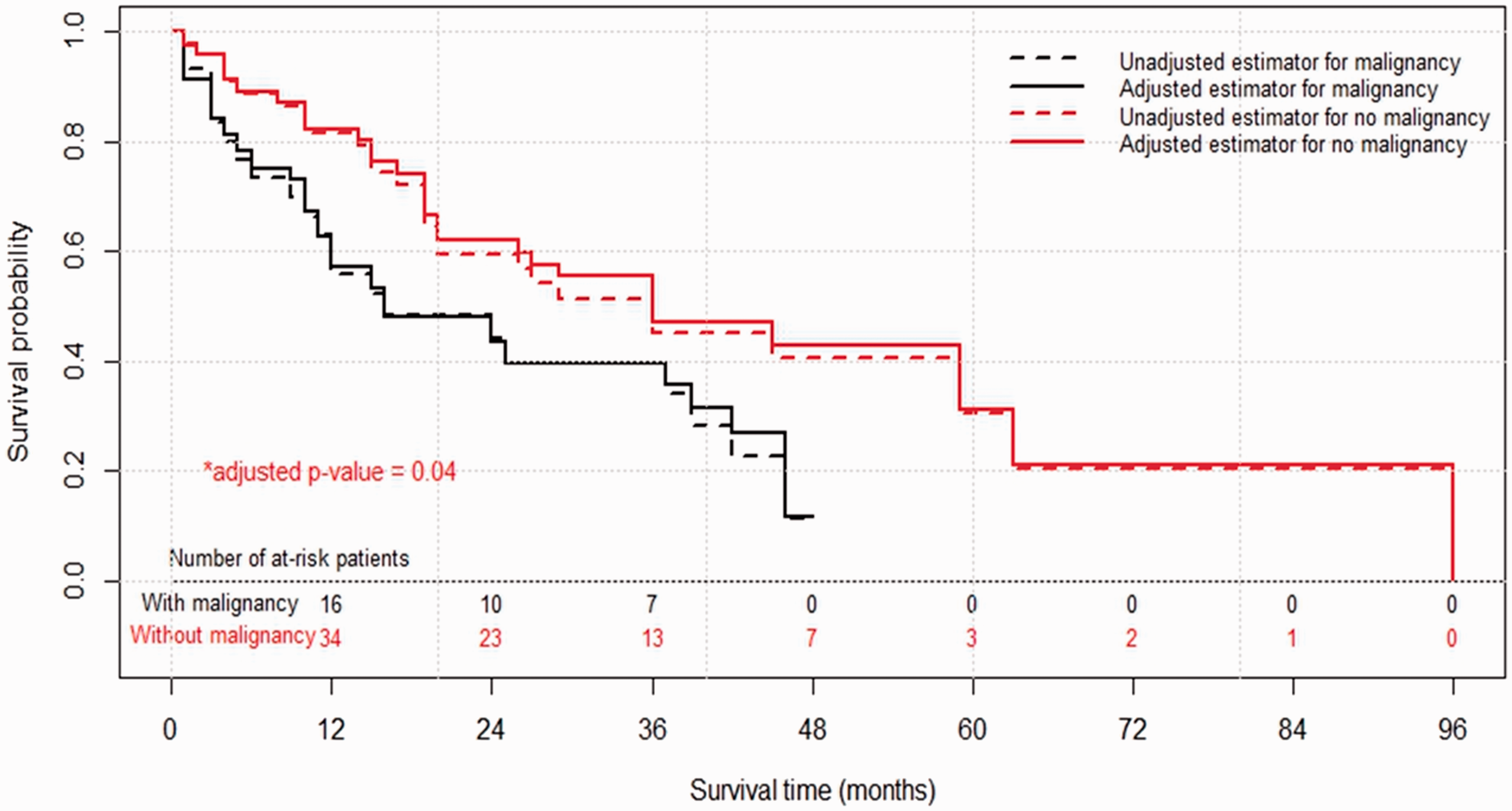
Comparison of survival rates in patients with and without active malignancy at time of AAA detection. p value by log rank test. AAA: abdominal aortic aneurysm.
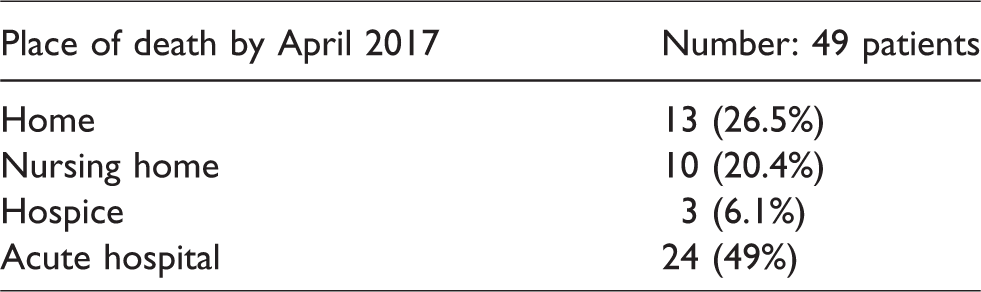
According to the NDR, only six (12.24%) patients underwent autopsy of whom three patients (6.1%) were found to have suffered ruptured AAA. A significant proportion of patients (49%) died in an acute hospital (Table 4).
Place of death.
Overall survival in the conservatively managed group (n = 76) was significantly worse than the 381 patients who underwent elective open or endovascular repair during the same time period (p < 0.01) (Figure 3). Pairwise comparisons using log-rank test were used to assess differences between treatment groups. There was a statistically significant difference between patients offered surgical treatment and those who were managed conservatively (open repair vs. conservative, p-value <0.001; EVAR vs. conservative p-value <0.001).
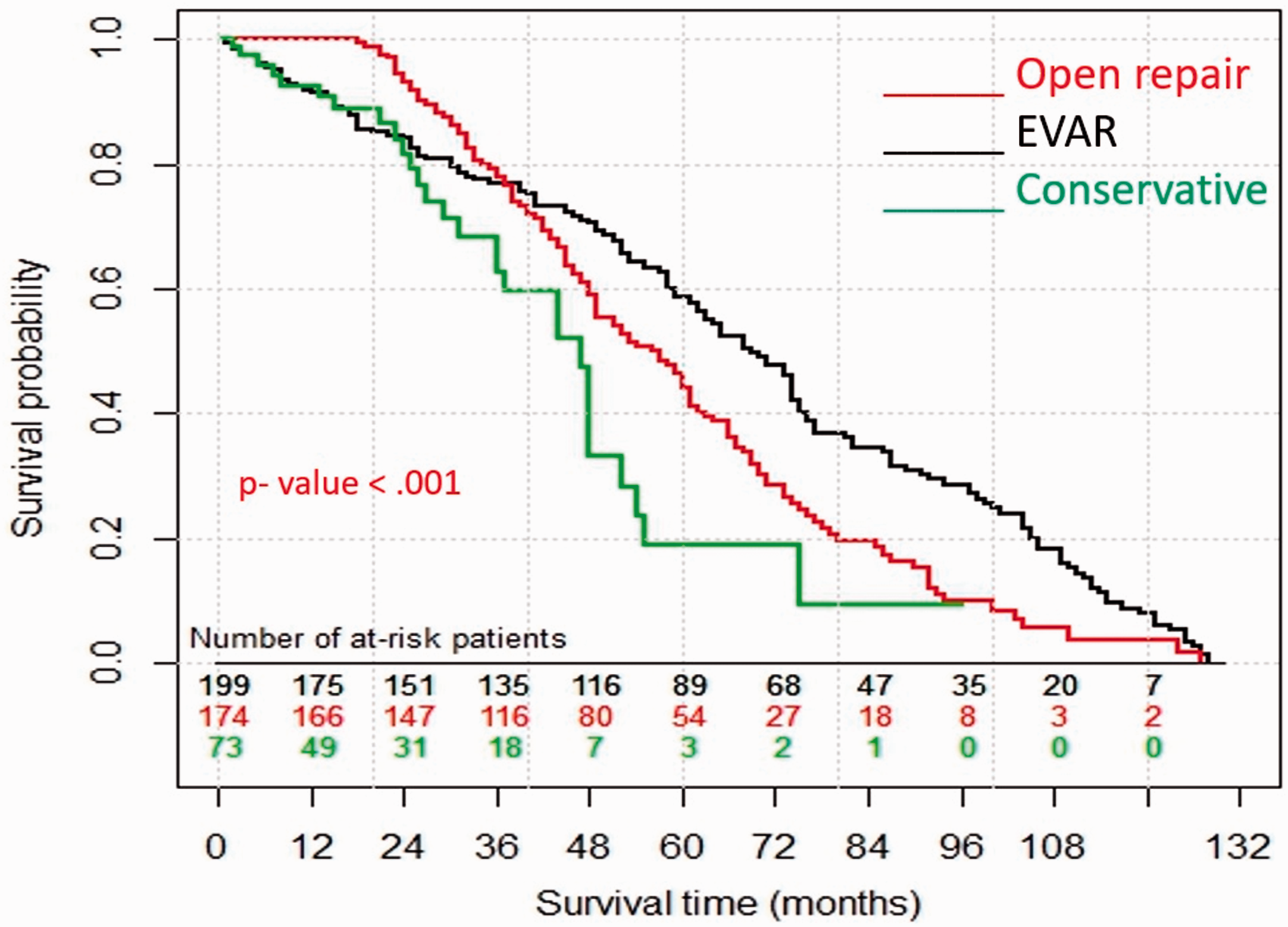
Comparison of survival rates among patients treated with open AAA repair, EVAR repair or conservative management. p value by log rank test. AAA: abdominal aortic aneurysm.
Discussion
The prevalence of AAA is estimated at 1.3–12.7% in the UK. Symptomatic AAA in men has an incidence of 25 per 100,000 at age 50, which increases markedly to 78 per 100,000 in those older than 70 years. 7
A recent Finnish study reported that ruptured AAA incidence in men over 65 years has declined by almost 30%, likely due to decrease in AAA prevalence. 8
While surgical repair in patients with large aortic aneurysm protects against fatal aneurysm rupture, it is associated with significant morbidity and mortality. 6 Decision making requires assessment of the balance of risks for intervention versus the risk of fatal rupture. A significant proportion of patients diagnosed with large AAA are deemed medically unfit for surgical intervention. As a result, these patients are managed conservatively often for extended periods of time. 9
Data on turndown rates for elective AAA repair remain largely unknown and under-reported. Knowledge of these figures is important when reporting morbidity and mortality figures from cohorts of patients treated for AAA.
The turn down rate in the current study is 16.63%. In a recent meta-analysis, Fran and Stuart 5 identified 11 studies with a wide range of turndown rates of between 8 and 31%.
Recently published studies evaluating turndown rates for elective AAA repair have shown similar demographic features to those in the current study. 10
In this study, mean duration of follow-up was 24.9 months with a non-aneurysm-related mortality rate of 69.5%. Lotfi et al. 10 reported a median survival of 38 months with a non-aneurysm related mortality rate of 80%. The EVAR-2 trial results suggested no survival advantage was provided by performing EVAR in poor surgical candidates. 6 Jones et al. 4 concluded that the majority of patients deemed unfit for surgery died from causes other than AAA and that only a very small number of patients would have benefited from elective aneurysm repair. 11 This suggests that a non-operative, conservative approach is justified in those patients with large AAAs whose medical co-morbidities preclude surgical repair.
In contrast, Fillinger et al. 11 reported that AAA rupture was the predominant cause of death in patients with an untreated AAA with a median time to rupture of nine months in patients with AAA >7 cm. A recent meta-analysis suggested a rupture rate of 27 per 100 patient years for aneurysms with a diameter larger than 6 cm. 12
The current study identified a significantly lower survival in patients deemed unfit for surgery, compared to those who underwent open repair or EVAR. In addition, perioperative mortality among patients presenting emergently and treated surgically was particularly poor.
In the current study, there was no statistical significance between younger (≤75 years) and older age (>75 years) cohorts. This illustrates that survival is determined by an individual patient’s general fitness rather than by their chronological age.
Another aspect of management of patients deemed unfit for elective AAA repair is the decision to be made in the event of these patients presenting as emergencies with acute aneurysm rupture. Fran and Stuart 5 report a series where emergency repair was offered to 32% of patients deemed unfit for elective AAA repair with a perioperative mortality rate of 58%. In the current series, emergency repair was performed in 37.5% of patients previously deemed unfit for elective surgery presenting with ruptured AAA. Only one patient (16.6%) survived. This experience suggests that this population of frail, elderly patients should not be subjected to futile emergency surgery. Our practice involves managing pain and providing end of life comfort measures in conjunction with the hospital palliative care medical and nursing teams.
Improved access and quality of diagnostic imaging have resulted in increased numbers of AAA being detected in patients being investigated for malignancy. This explains the high prevalence of cancer in our cohort of patients, with lung cancer being a commonly associated malignancy. Other studies have shown similar results but with different types of commonly occurring malignancies. 13
This study examines the fate of a relatively small number of patients in a single centre which limits more detailed sub-group analysis of factors which impact on patient outcome. Mortality data were cross-referenced with the hospital computer system and the National Death Registry, both of which provide accurate and verified information.
Accurate determination of patient outcome problematic in AAA ruptures studies because evaluation of cause of sudden death can be difficult to ascertain. The small number of autopsies carried out in this cohort means that the true rate of aneurysm-related deaths may be under-estimated and is the main limitation of the current study. A further potential problem arises if a patient has died outside of Ireland and the death has not been recorded in the NDR. Furthermore, data may have been lost if the process of death registration took more than three months which is the time from end of follow up to data collection from national death registry office.
Cardio-pulmonary exercise testing (CPET) was not routinely performed at the time of this study and may be seen as a limiting factor in providing objective evidence of a patient’s fitness for elective AAA surgery. However, the frailty of many of the patients particularly those ultimately turned down for surgery precluded this form of assessment.
Stratification of unfit patients according to aneurysm size at time of rupture was not possible in our study because patients were not routinely followed up to assess aneurysm size once a decision had been made not to proceed with surgery. A study by Lederle et al. 14 reported that patients with probable rupture had a significantly greater mean AAA enlargement rate than patients without rupture (0.75 cm per year vs. 0.41 cm per year; p < 0.003). However, the absence of this data does not diminish the main conclusion of the current study which remains that the mortality of patients turned down for elective AAA repair, for whatever reason, is high.
Conclusion
Ruptured AAA was not a major cause of death in patients deemed unfit for elective surgical repair of large AAAs. Most of such patients die from causes unrelated to their aneurysm.
Survival may be unrelated to the age of patients at time of turndown for elective surgery mainly because of other significant confounding factors as malignancy. Patients with active malignancy at the time of diagnosis have lower survival rates with most of deaths due to metastatic disease rather than aneurysm rupture. Attempted repair of ruptured AAA in this group does not add any benefit to patient survival.
Publication of turndown rates, alongside mortality rates would provide more accurate indication of morbidity and mortality and allow for more realistic comparison of outcome data from elective AAA repair.
Footnotes
Acknowledgements
The article has been presented at the following meeting: Irish and North Ireland vascular associations of vascular surgery (IAVS and NIVASC) Joint annual meeting, Dublin, Ireland, May 6, 2017.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.