
Abstract
Objective
Data in literature suggest iliac artery dilatation and endograft retraction as complications after endovascular aneurysm repair. However, mainly older generation endografts were included. Therefore, we sought to evaluate the distal sealing zone chronological changes after endovascular aneurysm repair with newer generation stent-grafts.
Methods
Clinical and radiological data of patients with abdominal aortic aneurysms treated with endovascular aneurysm repair between January 2010 and December 2013 were reviewed. Measurements were made using volumetric reconstructions in the first and last available computed tomography angiography. Endpoints of the study were the presence of iliac dilatation and retraction of the endograft. Association with distal oversizing and sealing length was analyzed.
Results
Consecutive patients with a total of 52 common iliac arteries were included in the study (mean age 74.9 ± 6.8 years, four women (7.7%)). The mean follow-up was 3.1 years. The mean iliac diameter increased from 15.5 to 17.1 mm (p < .001) in the first control computed tomography angiography and to 18.7 mm (p < .001) in the last available computed tomography angiography. No endograft (Endurant by Medtronic (24/52; 46%), Excluder de Gore (23/52; 44%), Zenith by Cook (5/52; 9%)) was associated with dilatation (p = .066) or iliac retraction (p = .591). Two type Ib endoleaks were found (3.8%) and successfully treated with distal graft extension. An iliac branch retraction of ≥5 mm was identified in seven cases (13%). Iliac arteries treated with limbs of ≥24 mm in diameter dilated significantly more than the rest of limbs (5.37 mm versus 3.12 mm; p = .022). In the last available imaging, iliac dilatation was ≥20% in 28 cases (53.8%) and had exceeded the diameter of the implanted endograft in 20 cases (38.4%). Iliac dilatation (OR 15.11 per mm, p = .025) was identified as a risk factor for retraction ≥5 mm.
Conclusion
Iliac dilatation and endograft limb retraction are common findings after endovascular aneurysm repair despite the use of new generation endografts. Optimizing the iliac sealing length and meticulous computed tomography angiography surveillance are recommended especially in case of use ≥24 mm iliac stent-grafts to prevent possible complications.
Keywords
Introduction
Endovascular aortic aneurysms repair (EVAR) offers a less invasive alternative especially for patients with severe comorbidities deemed unfit or high risk for open surgery,1,2 though long-term results are less inspiring due to late complications requiring reintervention. 3 There is plenty of data regarding the proximal neck changes, dilatation, and migration after EVAR;4,5 however, the evidence on iliac evolution after implantation is scarce.
Previous publications have suggested iliac artery dilatation and endograft retraction as common events after EVAR.6,7 Nonetheless, the results are mainly withdrawn from the first generation, more rigid endografts,8,9 which had previously been regarded to be prone to iliac sealing complications. 10 New generation more flexible and adaptable devices are being continuously developed to broaden the treatment range and improve outcomes. 11
In that matter, we sought to evaluate iliac sealing evolution after EVAR with the nowadays available endografts and their possible association with clinical events.
Methods
Study design
All patients treated at our center with EVAR for abdominal aortic aneurysm (AAA) between 2010 and 2013 were retrospectively reviewed. Only endografts with sealing in the common iliac arteries were included. The presence of iliac, infected or anastomotic aneurysms, as well as endografts with extension to external iliac was excluded. Patients without at least two control computed tomography angiographies (CTAs) were also excluded. Data collection and acquisition was approved by the local ethics committee.
According to our practice, all patients have at least one preoperative CTA.
Our surveillance protocol includes control postoperative CTA maximum one month after surgery, and if no complications are noted, duplex ultrasound at six months and subsequent annual control CTA. Ultrasound surveillance was adopted only in cases without complications (correct sealing, stable sack or shrinkage, no leaks or migration) detected in control CTAs.
Definitions
Iliac dilatation was defined as an increase > 2 mm of the iliac outside to outside diameter. Retraction of the endograft was considered if the distance between the last stent and the iliac bifurcation had increased ≥5 mm. Oversizing was calculated using the formula: (diameter of the implanted limb − native iliac diameter)/native iliac diameter. Complications of the iliac seal were considered if one of the following occurred: Type Ib endoleak or iliac limb related reintervention. Presence of iliac tortuosity was set at ≥ 90° based on the preoperative CTA.12,13
CTA analysis
A specific workstation was used for all measurements (Philips, Eindhoven, The Netherlands). Two trained observers analyzed the defined parameters after manually performing central luminal line (CLL).
Following SVS AAA management guidelines, iliac diameter measurements included wall thrombus burden excluding calcification. 1 Iliac dilatation and retraction were measured by previously described and validated method by Gonçalves. 7 The distal edge of the last implanted stent was used as a starting point. Iliac diameter was measured 10 mm proximal to that point in the first control CTA, last available CTA, and in the preoperative CTA. To evaluate the endograft retraction, the distance from the distal edge of the last graft stent to the iliac bifurcation was measured in the first and last control CTA.
Iliac seal length, as for the circumferential apposition length between the stent-graft and the iliac artery wall, was also measured by previously described methods. 14
Statistical analysis
Discrete variables are presented as counts and percentages, and continuous variables as mean standard deviation, if they are normally distributed or median (interquartile range) if they are not normally distributed. Individual differences in length and diameter over time were calculated using related samples. Associations between iliac dilatation, stent retraction, and complications of distal sealing were tested using Mann statistics. Whitney U for nonnormal continuous variables or with Pearson’s chi square data for categorical variables. An α value of <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics (version 22, IBM Corporation, Somers, NY, USA).
Results
Seventy-eight patients with AAA were treated by EVAR in our center from January 2010 to December 2013. Of these, nine had iliac aneurysms and one aortic pseudoaneurysm. Twenty-six patients without at least two postoperative control CTAs were also excluded. Among the remaining 42 patients (5 aortouniiliac AUI EVAR (9.6%) and 74 bifurcated stents), 27 iliac arteries with sealing in external iliac arteries were excluded. Finally, 52 common iliac arteries were included for analysis (Figure 1).

A diagram of patient flow through the inclusion and exclusion process. AUI: aortouniiliac; CTA: computed tomography angiography; EVAR: endovascular aortic aneurysms repair.
Baseline patient and device characteristics
The average age of the studied population was 74.9 ± 6.8 years, and there were four (7.7%) women (Table 1). The preoperative AAA diameter was 60.3 ± 9.1 mm, while common iliac arteries diameter was 15.7 ± 3.2 mm. The employed devices were Medtronic Endurant (24/52, 46%), Gore Excluder (23/52, 44%), and Cook’s Zenith (5/52, 9%). The mean time of follow-up was 3.1 ± 1.4 years. Mean iliac limb oversizing was of 9.5%. Vessel tortuosity ≥90° was present in 15.3% of the iliac arteries.
Baseline patient, aortoiliac, and device characteristics.
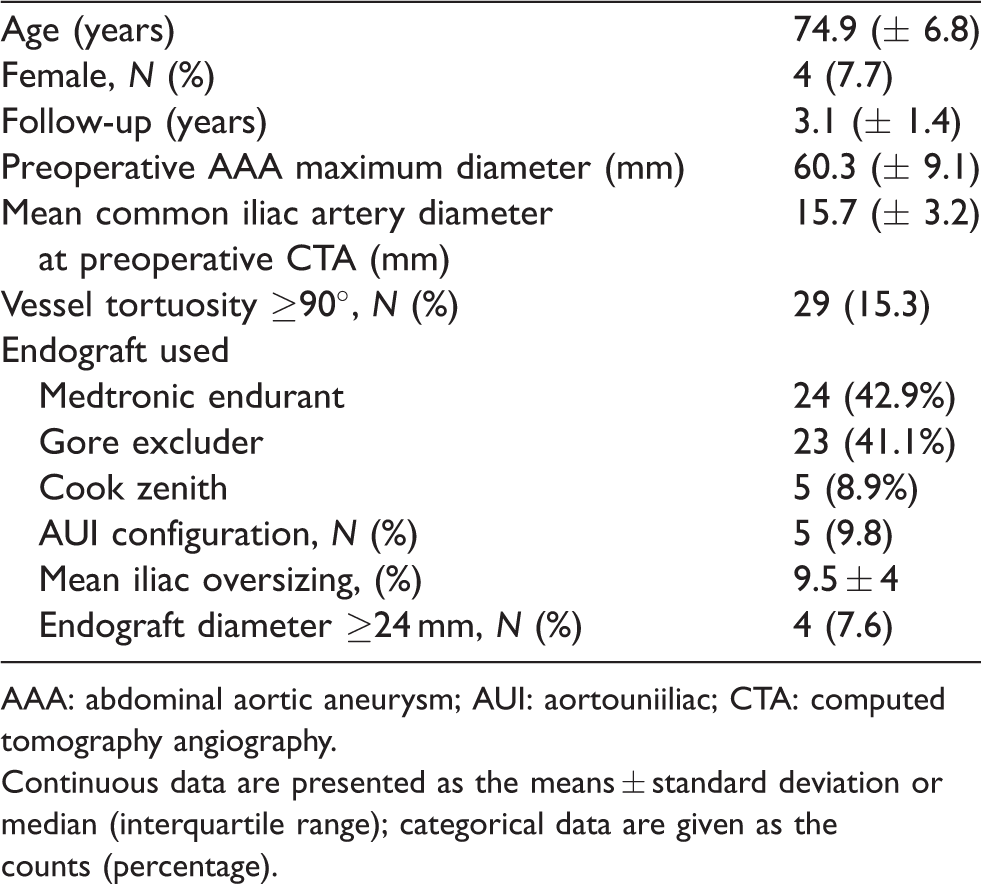
AAA: abdominal aortic aneurysm; AUI: aortouniiliac; CTA: computed tomography angiography.
Continuous data are presented as the means ± standard deviation or median (interquartile range); categorical data are given as the counts (percentage).
Iliac dilatation
The mean iliac diameter measured increased from 15.5 to 17.1 mm (p <.001) in the first control CTA and to 18.7 mm (p < 0.001) in the last available CTA (Table 2). In the last available CTA, iliac dilatation was ≥20% in 28 cases (53.8%) and had exceeded the diameter of the implanted endograft in 20 cases (38.4%). Among the patients treated with stents of ≥24 mm in diameter, the mean iliac dilatation was 5.37 ± 2.24 mm, while for the remaining patients it was 3.12 ± 1.81 mm (p = 0.022). None of the devices was significantly associated with iliac dilatation (p = .066).
Iliac evolution and sealing complications during follow-up.
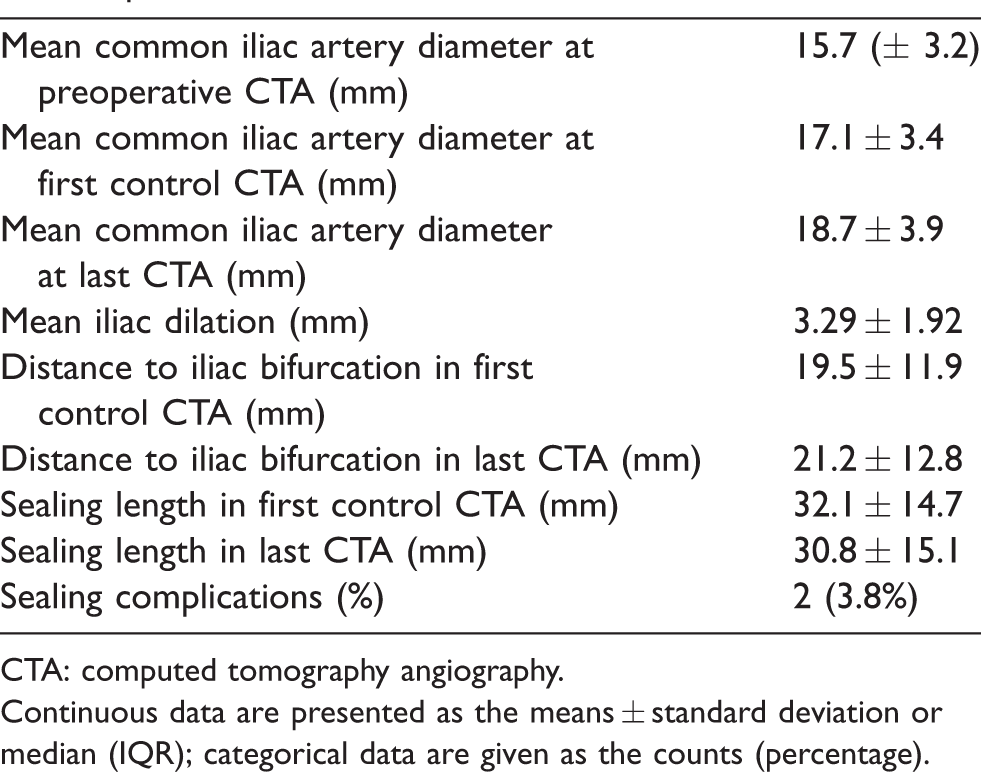
CTA: computed tomography angiography.
Continuous data are presented as the means ± standard deviation or median (IQR); categorical data are given as the counts (percentage).
Retraction
In the first control CTA, the mean distance from the distal edge of the stent to the iliac bifurcation was 19.5 ± 11.9 mm. A retraction of ≥5 mm was observed in seven cases (13%). Iliac artery dilatation was identified as a statistically significant risk factor for endograft retraction ≥5 mm (OR 15.11, 95% CI, p = 0.025) (Table 3). Mean iliac seal length was 32.1 ± 14.7 mm in the first control CTA decreasing to 30.8 ± 15.1 mm in the last available CTA. None of the identified abdominal devices was associated with retraction ≥5 mm (p = 0.591).
Risk factors for endograft retraction.
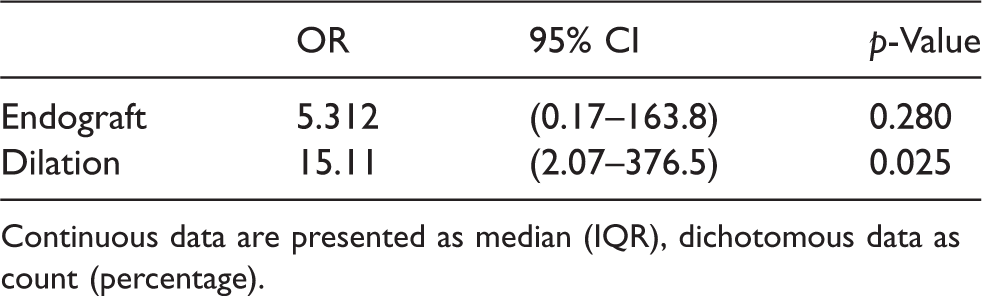
Continuous data are presented as median (IQR), dichotomous data as count (percentage).
Iliac seal complications
Two type 1b endoleaks were identified after the first control CTA among the 52 treated iliac (3.8%), of which one presented retraction ≥5 mm. Both endoleaks were successfully treated by distal extension of the prosthesis. Twenty-one patients presented type 2 endoleaks (40.3%) of which five required embolization with coils due to significant sac growth. There were four iliac arteries treated with ≥a 24 mm stent, two of which were AUI devices.
Acute thrombosis of the prosthesis was not observed in the present cohort during the follow-up period. One of the AUI grafts presented nonocclusive thrombus inside the prosthesis posteriorly to the first CTA and was treated with indefinite anticoagulation.
Discussion
While proximal EVAR attachments can be accurately assessed following already standardized methods,5,15 measurements of iliac changes after implantation are complex and difficult to reproduce, and thus, difficult to standardize. Different evaluation methods for iliac artery changes after stent-graft implantation have been described over the years.16,17 However, literature mainly focuses on diameter changes in ectatic iliac arteries indicating iliac diameter measurement at different anatomical points. Kaladji et al., 6 for example, measured diameter at three points of the iliac arteries showing finally a trend toward dilation over time. Besides vessel dilatation, our evaluation focused on iliac limb retraction following Gonçalves’ method, based on CLL and anatomical marks allowing measurements at the same location as well as the evaluation of iliac limb retraction. 7 In that matter, iliac sealing zone has proven to remain dynamic and a possible source of morbidity and treatment failure6,7—a finding corroborated in the present study. Iliac dilatation starts at implantation and continues expanding over time. 7 Although the presents study reports a relatively high rate (38.4%) of iliac artery dilatation exceeding the diameter of the implanted endograft, few sealing complications as for type 1B endoleaks (3.8%) were noted as apposition between the graft and the iliac artery was still conserved over the follow-up period. However, following the natural history of iliac seal zones, it seems like iliac arteries will continue to degenerate possibly leading to type 1B endoleaks,6,14,16 keeping the premise that larger iliac arteries seem to grow faster over time.
Iliac dilatation has shown to be a risk factor for limb retraction, which is possibly the preceding step before developing a sealing complication. 15 Insufficient iliac fixation length has been associated with the risk of proximal device migration, sidewise displacement, and related adverse events,18,19 regardless of the type of proximal endograft fixation. 20 In the same line, limb retraction has been linked to iliac seal complications. 21 Data in literature analyzed first generation devices known to have stiffer iliac components with high columnar force previously regarded to be more prone to iliac seal complications.8,22 Our study reviewed new generation endografts with more flexible iliac limbs despite which iliac dilatation and retraction were again common events. None of the commonly used abdominal endografts have been particularly associated with iliac dilation, per se, up to date. Dilation following implantation of oversized self-expanding stent-grafts reproduces an already well-characterized phenomenon at the proximal aneurysm neck. 5 Similarly, iliac expansion beyond the diameter of the implanted endograft and stent retraction seems to be common events despite the flexibility and adaptability of the new generation stent-graft. A tentative explanation of these findings is based on the increased wall shear stress at areas of overlap as well as at the kinking zones of the endograft. The presence of the endograft, in addition to decreasing pressure in the aneurysmal sac, also alter the constraints at the level of the iliac arteries resulting into more significant stress and pressure compared to the preoperative period. 6 Besides, the fact that patients with an aneurysmal arterial disease with collagen or connective tissue disorders per se are being treated shall be taken into account. Therefore, increasing the distal seal length at the original implantation to reduce the risk of complications, regardless of the specific endograft model, is recommended. 14
It has been previously shown that common iliac artery enlargement was more pronounced in patients with ectatic iliac arteries—a finding corroborated in the present cohort.16,23 Also, iliac diameter of ≥ 20 mm has shown to be an independent risk factor for sac enlargement. 24 Several other studies reported a higher risk of complications and endograft-related reinterventions in patients requiring bell-bottom iliac limbs.17,25 Probably due to the few complications, these findings were not corroborated by the present series. Of note, while oversizing greater than 15% in the common iliac artery and tortuosity have shown to be risk factors of limb occlusion after EVAR,26,27 oversizing of less than 10% and only 15.3% of patients having tortuosity greater than 90° may have acted as a protective factor for complications in our cohort.
Previous analysis of aortoiliac characteristics leading to EVAR nonsuccess has ruled out calcification or iliac thrombus formation to be statistically significant features related to that matter.28,29 Following this premise, and since our analysis focused on iliac changes after EVAR, presence of calcium or thrombus was not considered for correlation taking into account other relevant iliac characteristics such as iliac tortuosity and diameter, having previously shown correlation with iliac seal.6,7
Limitations
The study is limited by its retrospective design, small sample size, and lack of long-term results. A larger span, patient recollection, and evaluation would have of course supposed larger patient cohort and higher statistical significance. However, on one hand, endovascular treatment of aortic pathologies at our institution started a few years before the initial patient inclusion. Hence, avoiding initial study curve, we preferred to initiate patient collection in 2010. And on the other hand, following previous studies on iliac evolution after endograft implantation,6,7 we preferred to obtain longer follow-up to evaluate possible iliac arterial wall changes after stent-graft implantation rather than obtain a larger number of patients. Also, following our objective of evaluating iliac changes using new generation devices, implantation of those devices at our institution was started in 2010. Therefore, inclusion of patients treated with other second generation endografts would have a relevant heterogeneity in the analysis and was avoided. Additionally, the use of three different abdominal endografts restrains the complete homogeneity of our cohort. Another limitation is the very few clinical events in the present series, which limits the capacity for discriminating risk factors to make stronger recommendations.
Conclusion
Iliac dilatation and endograft limb retraction are common findings after EVAR despite the use of new generation and more flexible endografts. Progressive iliac seal zone dynamics may lead to sealing complication. Optimizing the sealing length and surveillance with CTA are recommended especially in ≥24 mm stent to prevent possible complications. Long-term surveillance with CTA is advised to reveal loss of seal at the iliac attachments and prevent adverse clinical events.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.