
Abstract
Objectives
The purpose of this study was to conduct a meta-analysis to systematically compare the safety and efficacy of carotid endarterectomy and carotid artery stenting in contralateral carotid occlusion patients who needed reperfusion.
Methods
This study retrieved potential academic articles comparing results between carotid endarterectomy and carotid artery stenting for patients with contralateral carotid occlusion from the MEDLINE database, the PubMed database the EMBASE database, and the Cochrane Library from January 1990 to May 2018. The reference articles for the identified studies were carefully reviewed to ensure that all available documents were represented in the study.
Results
Four retrospective cohort study involving 6252 patients with contralateral carotid occlusion were included in our meta-analysis. During 30-day follow-up, there is significant difference in post-procedure mortality (odds ratio (OR) = 0.476, 95% confidence interval (CI) (0.306–0.740), P = 0.001); no significant differences are not found in post-procedure stroke (risk difference (RD) = 0.002, 95%CI (–0.007 to 0.011); P = 0.631), myocardial infarction (RD = 0.003, 95%CI (–0.002 to 0.008); P = 0.301), and transient cerebral ischemia (RD = 1.059, 95%CI (–0.188 to 5.964); P = 0.948).
Conclusions
Carotid endarterectomy was associated with a lower incidence of mortality compared to carotid artery stenting for patients with contralateral carotid occlusion. Regarding stroke, myocardial infarction, and transient ischemic attack, there was no significant difference between the two groups. More randomized controlled trials and prospective cohorts are necessary to help further clarify the ideal approach for these patients.
Keywords
Introduction
Carotid atherosclerotic stenosis has been the main cause of disabling stroke or death. It is reported that there are 700,000 cerebrovascular accidents every year in patients with carotid atherosclerotic stenosis. 1 Among those patients, 2.3% to 25% are accompanied with contralateral carotid occlusion (CCO), 2 and 14% of patients with CCO have twice as many post-reperfusion strokes as patients without CCO. 3
As we all know, carotid endarterectomy (CEA) combined with drug therapy has been a first-line reperfusion method for patients with carotid artery atherosclerotic stenosis. 4 Several large-scale clinical trials in recent years have established the status of CEA in the treatment of carotid stenosis as the “gold standard”.5–7 Simultaneously, carotid artery stenting (CAS) has gradually become an alternative reperfusion method to CEA and been commonly used in high-risk surgery, including those patients with CCO since the 1990s.8,9 Meanwhile, CCO disease has always been an independent risk factor for CEA and CAS, 10 and the effectiveness of CEA or CAS performed in patients with CCO was controversial in many clinical studies.11–16 Aburahma et al. 17 conducted a single center study to follow-up the results of 63 persons with CCO after CEA and show that it is necessary. In contrast, Baker et al. 11 conducted a study to compare the safety and efficacy of drug therapy vs. CEA for patients with CCO and demonstrated that no significant difference was found. A study of Northwestern 18 performed a data comparison on the results of CAS in patients with and without CCO, they found that there was no significant difference in two groups.
In theory, patients with CCO performed CAS have some advantages including reducing clogging time, avoiding shunt device, reducing complications of sedation or anesthesia. However, Nejim et al. 19 conducted a retrospective cohort study (RCS) involving 4326 patients with CCO and demonstrated that CAS is associated with a higher incidence of mortality and stroke for CAS compared to CEA during two-year follow-up. A meta-analysis of two surgical procedures was performed to compare safety and efficacy for CCO patients who needed reperfusion.
Materials and methods
PRISMA, 20 the abbreviation for preferred reporting items for systematic reviews and meta-analyses, was used for the study guidelines.
Search strategy
PRISMA was used to conduct our study. We sought to systematically and comprehensively retrieve all studies comparing results between CEA and CAS for patients with CCO through EMBASE, PubMed, MEDLINE, and the Cochrane Library of Controlled Trials from the date the first CEA was performed (in 1951) 21 and CAS was gradually used to treat carotid stenosis in the 1990s8,9 to May 2018. Complex search strategies were performed using “carotid endarterectomy OR CEA”, “carotid artery stenting OR CAS”, “carotid stenosis”, “contralateral carotid artery occlusion OR CCO”, “Carotid artery disease” as our search terms and keywords. All references for identified reports (including original studies, review papers, systematic reviews, and meta-analyses) were checked to search for trials that were not included in our electronic search.
Inclusion and exclusion criteria
Studies were included if they met the following preplanned criteria in accordance with PICOS: (i) population: limited the comparison to the CCO population; (ii) intervention: used strictly CEA and CAS; (iii) comparison: compared the results after CEA and CAS; (iv) outcome measures: the results with the 30-day follow-up; and (v) an official published full-text English-written randomized controlled trials (RCTs) or non-randomized controlled trial (non-RCT).
The exclusion criteria were as follows: (i) conference or commentary articles and letters to the editor; (ii) observational studies and animal trials; (iii) unclear patient characteristics and outcome data; (iv) case reports and case series; (v) systematic reviews or meta-analyses; and (vi) other types of carotid stenosis, such as radiation-induced carotid artery stenosis.
Data extraction
Preplanned data elements were extracted independently by two observers, W-QX and YZ, including basic data (author, publication time, age), study characteristics (trial type, postoperative follow-up time), and outcomes (stroke, mortality, myocardial infarction (MI), and transient ischemic attack (TIA)) in a tabular format and in a standardized form. The third investigator (X-YY) reviewed the data for accuracy and completeness, and he was simultaneously responsible for verifying and contacting authors in the event that data were incomplete or if disagreements occurred in the process of data extraction.
Ethical approval statement
All literature were carried out based on published studies, so ethical approval or patient consent was available.
Statistical analysis
Comparisons of the results after CEA and CAS were analyzed using standard software (Stata version 12.0 statistical software; StataCorp LP, College Station, Texas). For categorical variable outcomes, risk differences (RDs) or odds ratios (ORs) with 95% confidence intervals (CIs) were calculated for the assessment. When I2>50%, the data were considered as having obvious heterogeneity; therefore, a meta-analysis was conducted using a random effects model according to the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0). Otherwise, the fixed effect model was performed.
Results
Search results and study characteristics
Initially, 278 articles were identified by searching electronic databases and other sources, and 242 articles were removed by preliminary screening and duplicate article detection. Ultimately, four articles22–25 satisfied the inclusion and exclusion criteria for this research (Table 1). Full texts and references were carefully read. Other details are shown in the flow chart (Figure 1).
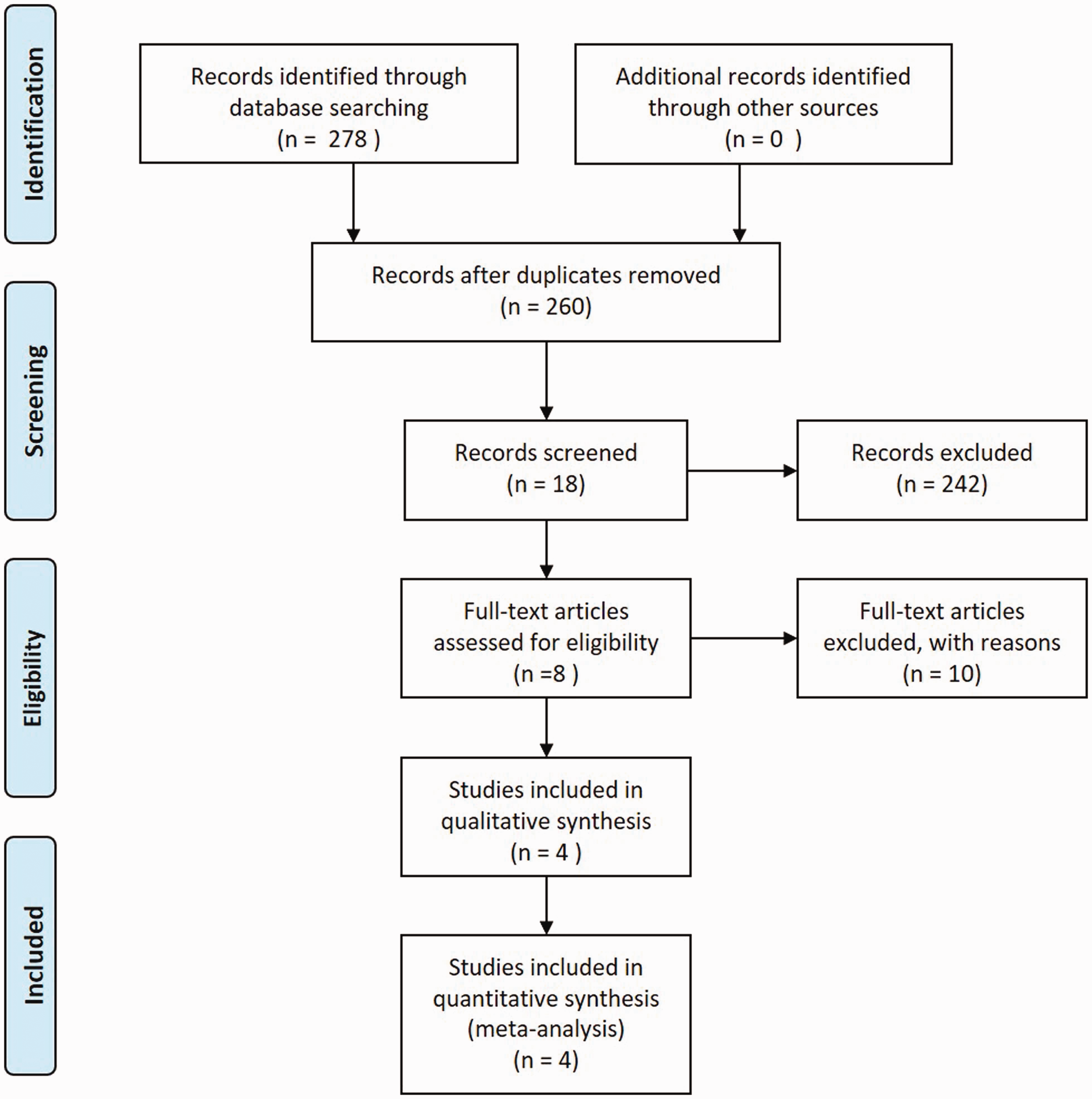
Study selection flow chart.
Summary of the included studies.

CEA: carotid endarterectomy; CAS: carotid artery stenting; EPD: embolic protection device.
Quality assessment
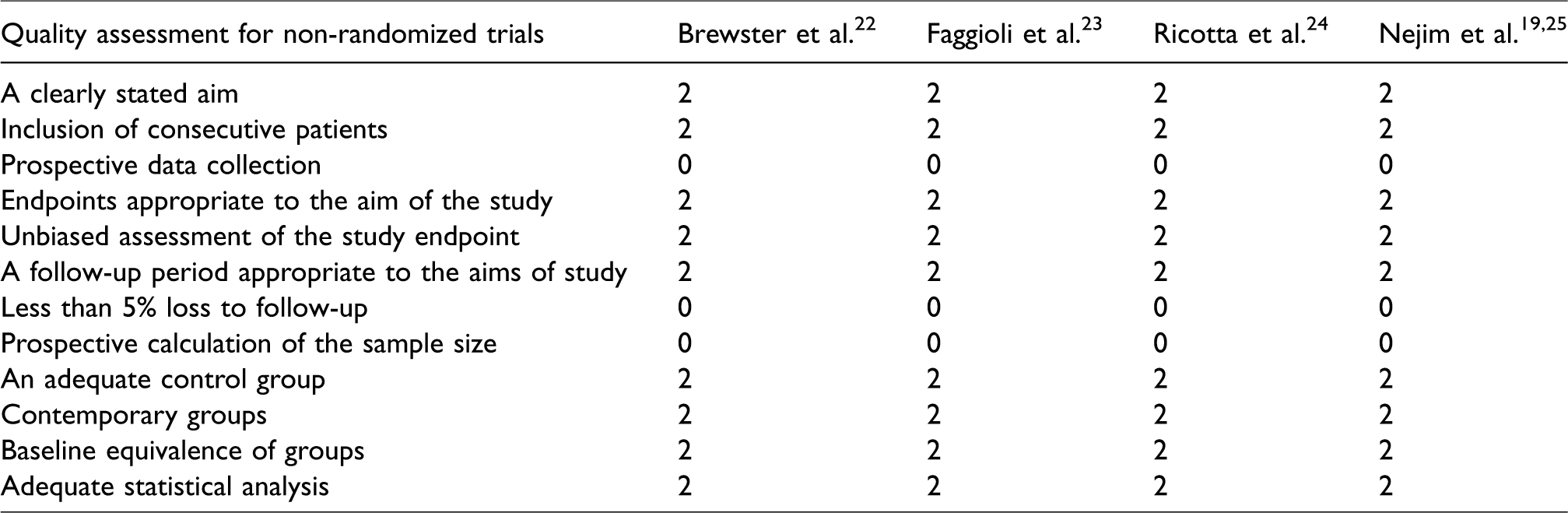
The literature quality evaluation was conducted separately by two reviewers. The study scores of all non-RCTs assessed by the methodological index for non-randomized studies and the scores of the four articles were all 18, more details are shown in Table 2.
Quality assessment score of the included studies.
Characters of patients
A total of four studies involving 6252 patients with CCO were performed with CEA or CAS with a follow-up period from 2 to 7 years, of which 3995 were CEA and 2257 were CAS. In the general condition, most of the patients were male with a mean age of about 60, although symptomatic and asymptomatic patients could dramatically impact the outcomes, no significant difference was found on this character in the two groups as shown in Table 3.
Characteristics of included trials.
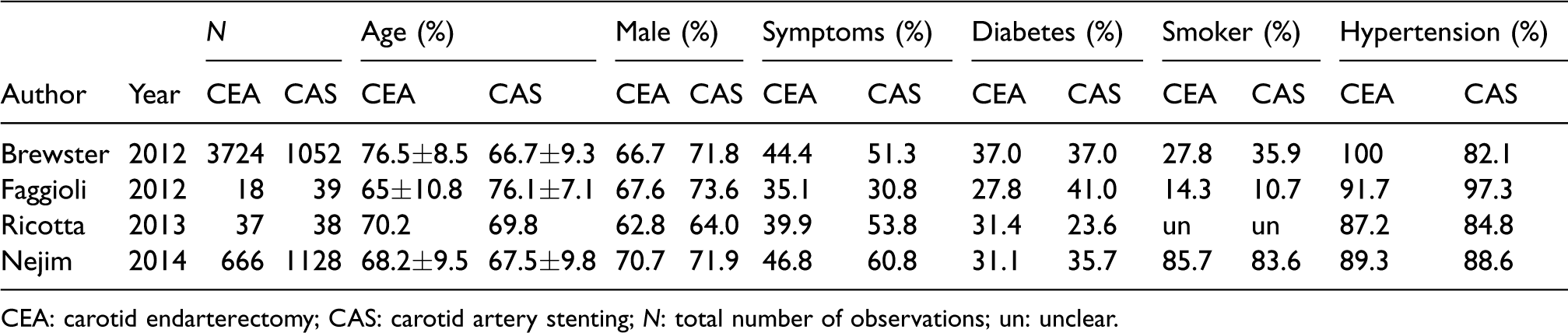
CEA: carotid endarterectomy; CAS: carotid artery stenting; N: total number of observations; un: unclear.
Thirty-day outcomes after surgery
A total of four results (postoperative mortality, MI, stroke, and TIA) that occurred within 30 days were analyzed in our study; the detailed information about the analysis of the other pooled results could not be carried out due to the lack of available data (Table 4).
Pooled results of post-procedure outcomes.
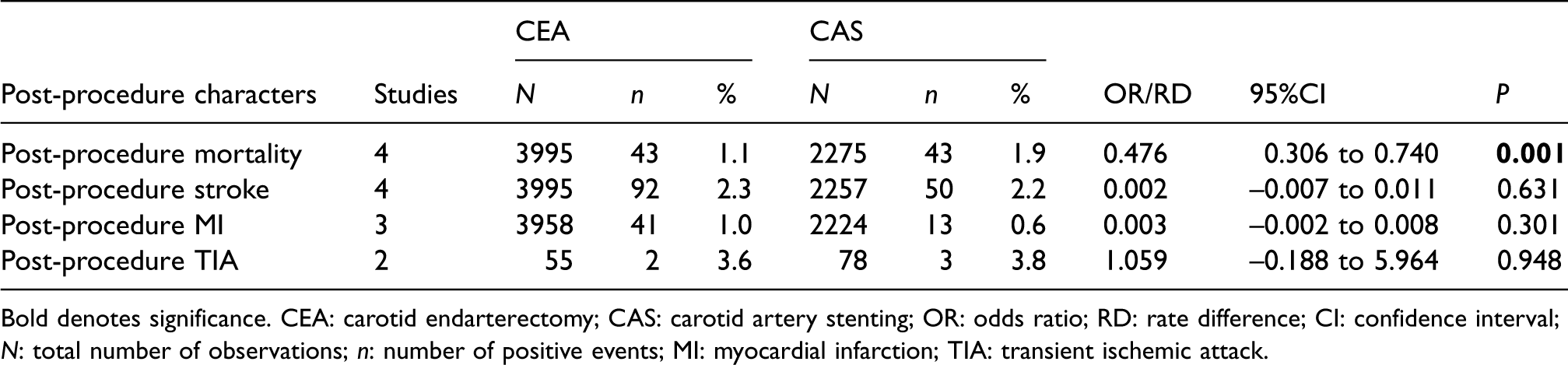
Bold denotes significance. CEA: carotid endarterectomy; CAS: carotid artery stenting; OR: odds ratio; RD: rate difference; CI: confidence interval; N: total number of observations; n: number of positive events; MI: myocardial infarction; TIA: transient ischemic attack.
Post-procedure mortality at 30 days
There are four publications including the results of postoperative incidence of mortality within 30 days, our meta-analysis showed that there was no heterogeneity between CEA and CAS groups (I2=0.0%, P = 0.512). A fixed effect model was used for analysis, the results showed that the 30-day incidence of mortality in the CEA group was significantly lower compared to CAS group (Figure 2), the related differences are statistically significant (OR = 0.476, 95%CI (0.306–0.740), P = 0.001).
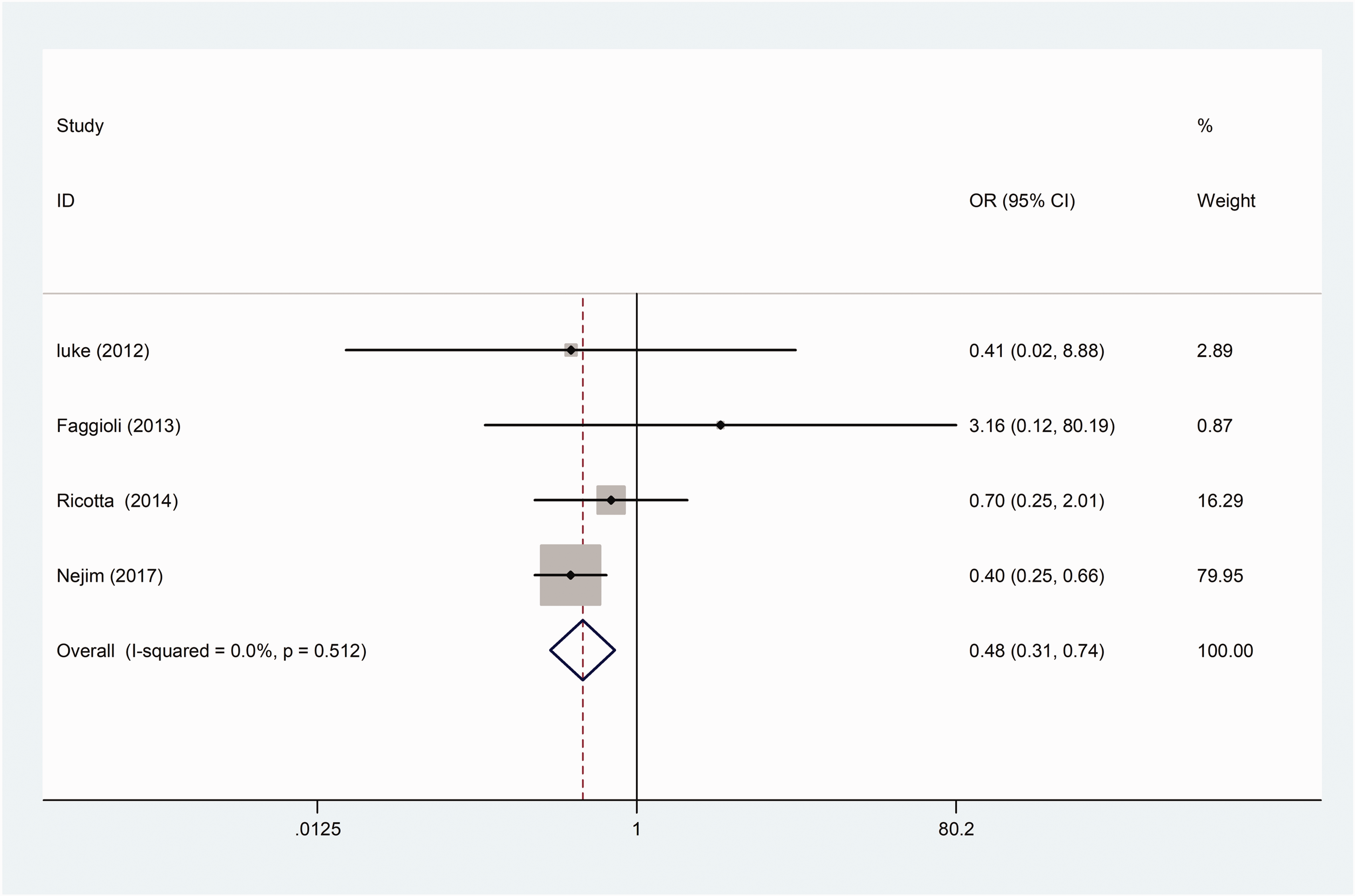
Forest plot of odds ratios (ORs) of post-procedure 30-day mortality with carotid endarterectomy (CEA) vs. carotid artery stenting (CAS; control).
Post-procedure stroke at 30 days
Four articles included the number of patients of postoperative stroke. In the CEA group, the incidence of stroke was 2.3% and in the CAS group it was 2.2%. Our meta-analysis showed that no heterogeneity was found (I2=0.0%, P = 0.190). The fixed-effects model was used to show that there was on differences in the rate of stroke between two groups (RD = 0.002, 95%CI (–0.007 to 0.011), P = 0.631; Figure 3).
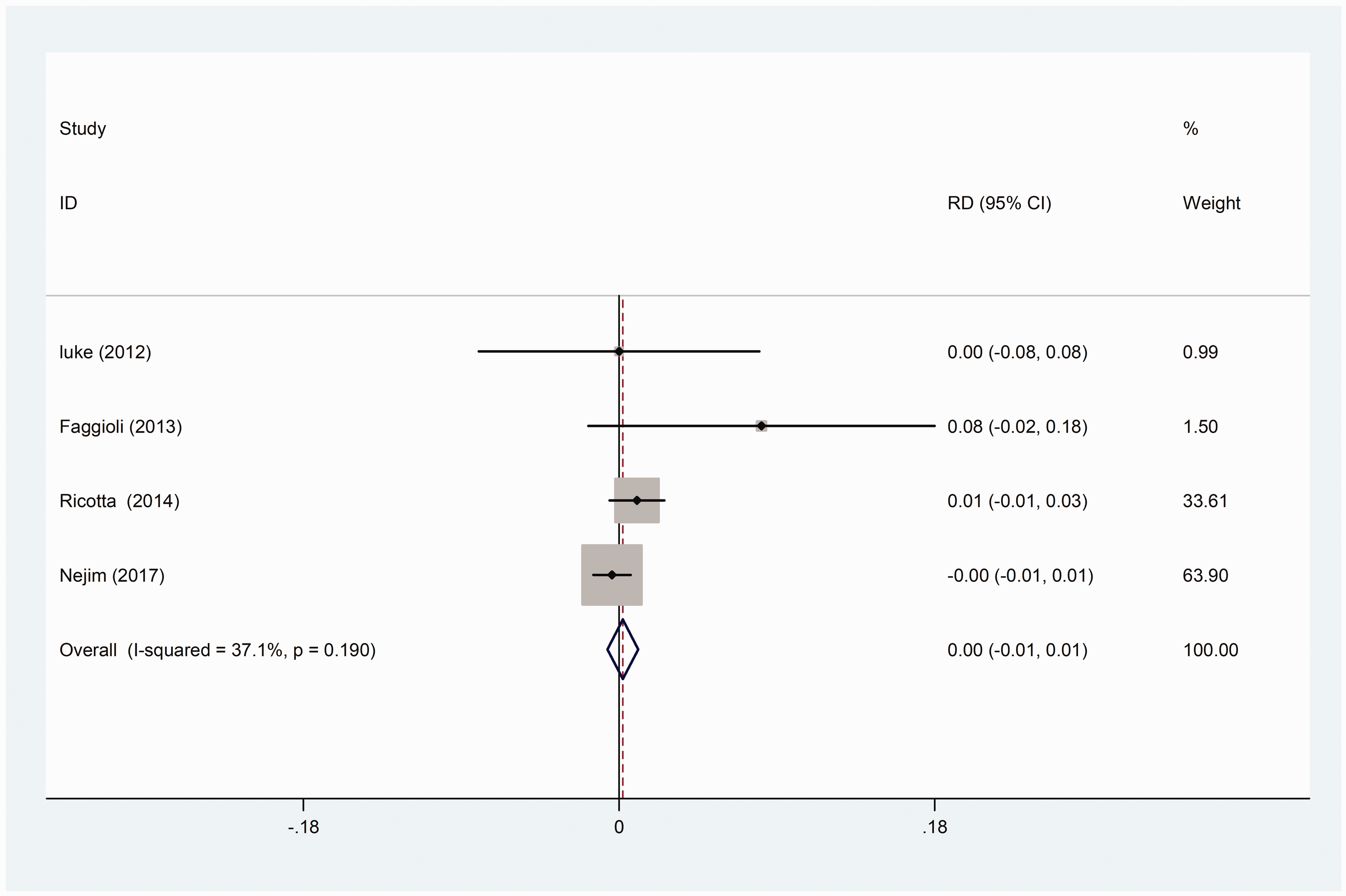
Forest plot of rate difference (RD) of post-procedure 30-day stroke with carotid endarterectomy (CEA) vs. carotid artery stenting (CAS; control).
Post-procedure MI at 30 days
There are three articles contained the number of patients of postoperative MI, there were 51 MIs and 13 MIs in the CEA and CCAS group, respectively. Our meta-analysis showed that two groups were not heterogeneous (I2=0.0%, P = 0.996). The fixed-effects model to show that no difference was found in the risk of MI appeared after surgery (RD = 0.003, 95%CI (–0.002 to 0.008), P = 0.301; Figure 4).
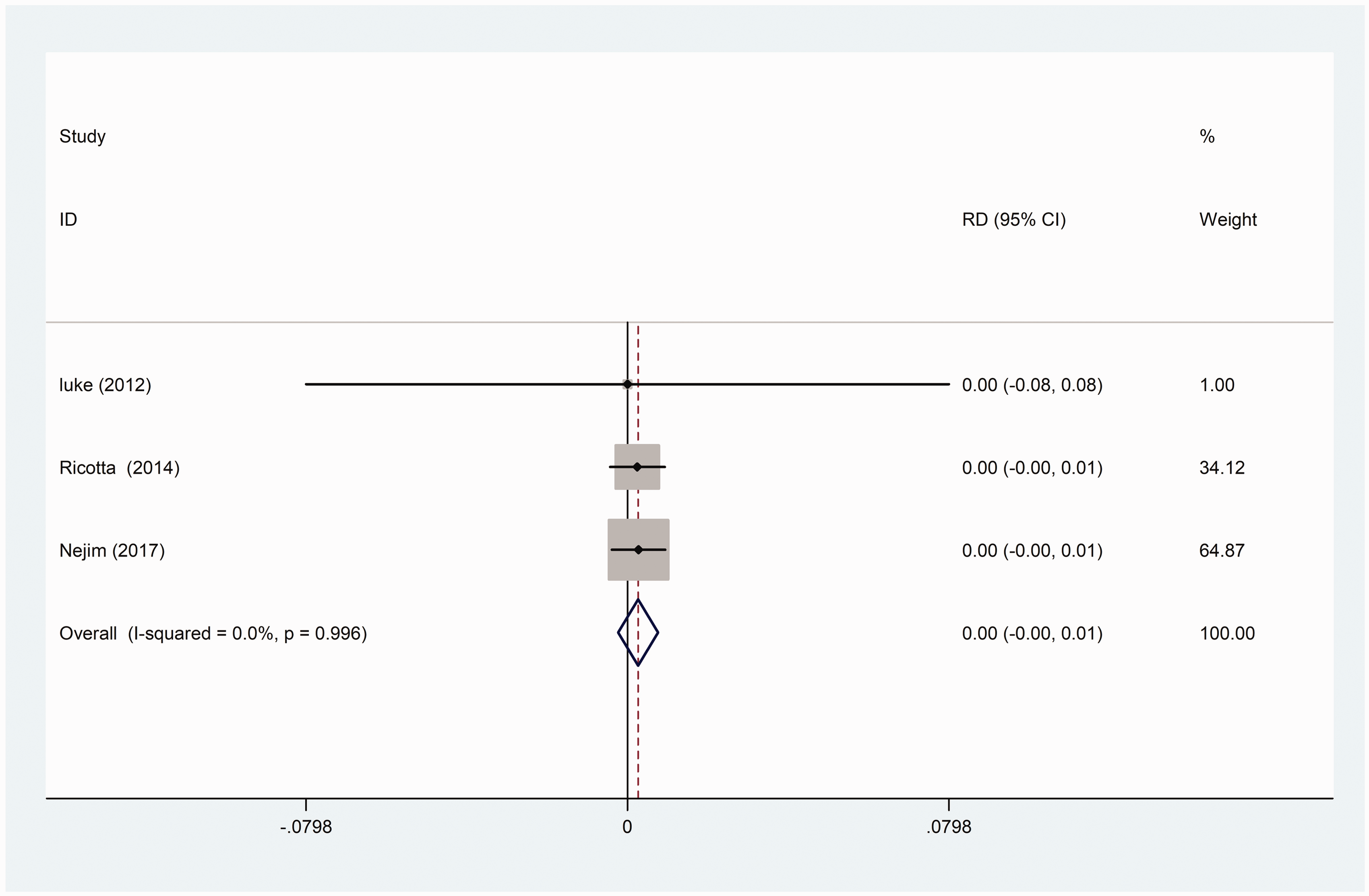
Forest plot of rate difference (RD) of post-procedure 30-day MI with carotid endarterectomy (CEA) vs. carotid artery stenting (CAS; control).
Post-procedure TIA at 30 days
Two studies reported the number of TIA patients in the postoperative period, of which 3.6% and 3.8% in the CEA and CAS group, respectively. The results showed that there was no heterogeneity between the two groups (I2=0.0%, P = 0.402), no difference in the risk of TIA within 30 days was found after surgery (RD = 1.059, 95%CI (–0.188 to 5.964), P = 0.948; Figure 5).
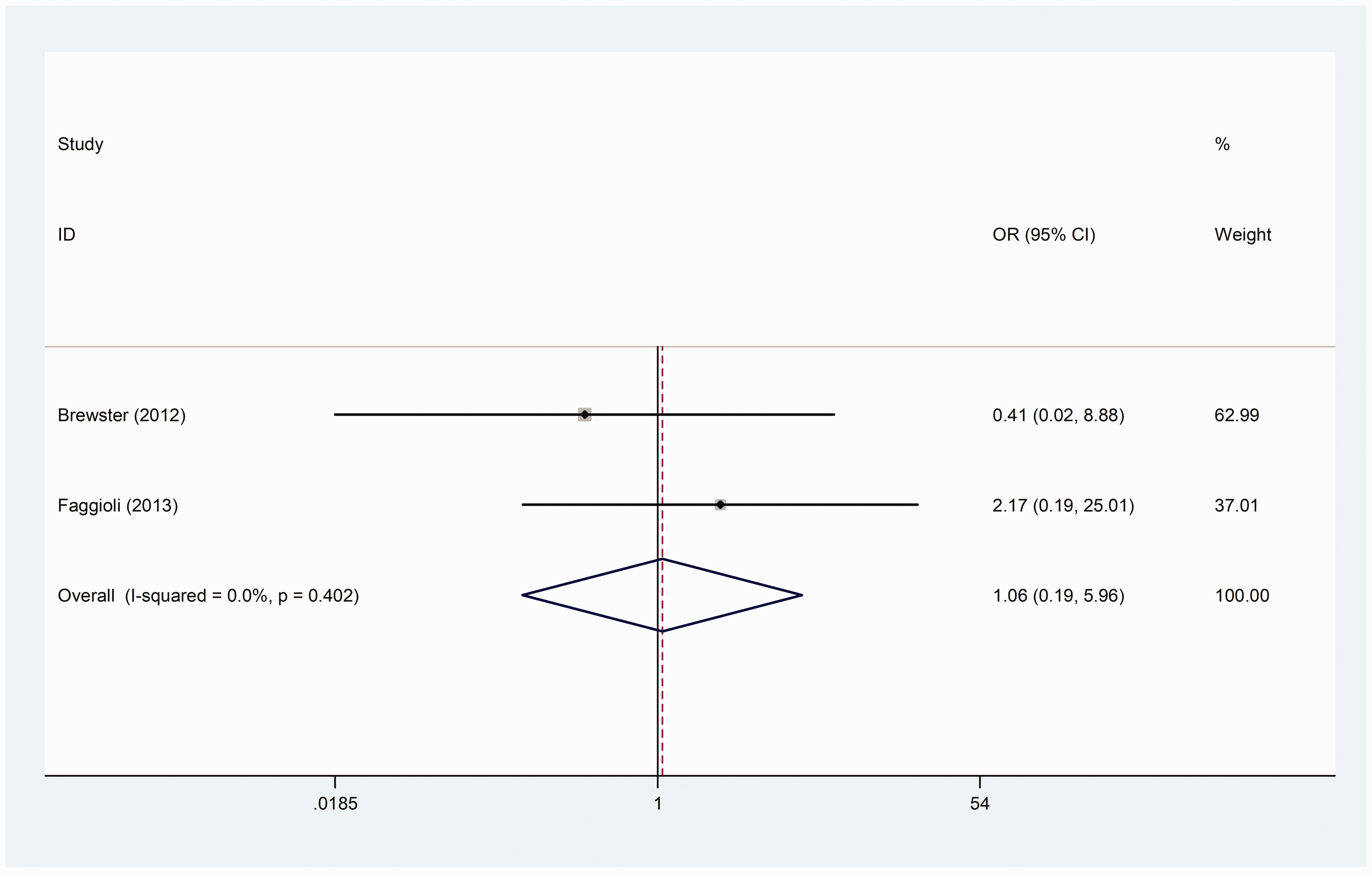
Forest plot of odds ratios (ORs) of post-procedure 30-day TIA with carotid endarterectomy (CEA) vs. carotid artery stenting (CAS; control).
Discussion
The efficacy and safety of CEA and CAS in the treatment of carotid stenosis, also in an acute setting, is gradually getting recognized. 8 Yuan et al. 26 performed CEA in 525 patients and CAS in 193 patients and showed that both reperfusion methods were useful for carotid artery atherosclerotic disease, but it was controversial for patients with CCO. 10 CCO may affect the intracranial collateral circulation and perioperative cerebral hemodynamics and then increase the risk of reperfusion. This study mainly analyzed the post-procedure 30-day rate of mortality, stroke, MI, and TIA in patients with CCO after surgery to examine the effect of the different reperfusion methods. Our meta-analysis showed that CEA was associated with a lower rate of post-operation mortality, regarding the incidence of post-operation stroke, MI, and TIA, no significant difference was found.
Keldahl et al. 18 conducted an RCS including 417 patients and considered that CAS will not increase postoperative mortality in patients with CCO, meanwhile, Mukherjee and Yadav 27 also pointed out that CEA can bring more adverse effects to CCO patients. However, the results of our meta-analysis indicated that the postoperative rate of mortality was significantly lower in the CEA group than CAS group, Brewster et al. 22 pointed out that one patient in the CAS group died of episode-induced respiratory failure three weeks after the operation, another one died of retroperitoneal hematoma. We speculated that it may be related to the postoperative use of anticoagulant and antiplatelet drugs. When the follow-up time was extended by two years or more, the CAS group increased by the death of five patients while four of the five patients in the CAS group died within two years, and the CEA group only was present with a death appeared in 44.8 months after the CEA; Nejim et al. 25 pointed out that the mortality rate of CEA group and CAS group was 1.1% and 1.9%, respectively (P < 0.001), after operation within 30 days, the similar results appeared in several larger multiple institutional studies.28,29 The hypothesis we had was that the degree of atherosclerosis is particularly severe for patients with CCO, and the plaque is likely to be soft plaques. Although protective devices were used in CAS – it requires a repeated pass through the stenotic blood vessels without block blood flow – emboli escape will still occur. Meanwhile, rejection reaction may be another cause of the higher rate of mortality in the CAS group. 30
Mackey et al. 31 persisted that CEA has a higher complication than CAS for patients with CCO, but the International Carotid Stenting Study (ICSS) indicated that no significant difference appeared in incidence of mortality, stroke, and myocarditis for patients with symptomatic CCO (CEA: 2 of 49 (4.3%); CAS: 1 of 37(2.7%); 95%CI, 0.14–16.61). 32 Similarly, our results showed that there were no statistically significant differences in the incidence of stroke, MI, and TIA between the two groups. According to Brewster et al., 22 no stroke and MI occurred in both groups, only two TIAs (5.1%) occurred in the CAS group. Faggioli et al. 23 conducted an RCS to demonstrate that CCO was an independent risk factor (any cerebral event and death) for CEA than CAS. And it pointed out that the incidence of TIA and stroke was higher in the CEA group than CAS group (stroke: CEA(8.1%), CAS(0%), P = 0.08; TIA: CEA(5.4%), CAS(2.6%), P = 0.10); Ricotta et al. 24 indicated that the number of patients appeared with stroke and MI were 21 and 4 in the CEA group and 24 and 4 in the CAS group, respectively; Nejim et al. 25 conducted a study comprised one of the largest numbers of patients with CCO to compare the results between CEA and CAS. He gained the similar conclusion that the difference in stroke and MI risk after surgery was not statistically significant (stroke: CEA(2.1%), CAS(2.5%), P = 0.445; MI: CEA(1.1%), CAS(0.9%), P = 0.449).
This study has several limitations: (i) The included studies were retrospective studies, and this meta-analysis was limited to the evaluation of 30-day results owing to the lack of available data. (ii) The results of new generation stents were not considered, which may have better results than those with larger or smaller cells. (iii) The experience of the center and operators was uneven. (iv) The details of shunt used in the CEA group are not comprehensive, and it should be reported for a better understanding of the risk of clamping ischemia in this particular group of patients with CCO.
Conclusion
CEA was associated with a lower incidence of mortality compared to CAS for patients with CCO. Regarding stroke, MI, and TIA, there was no significant difference between the two groups. More RCTs and prospective cohorts are necessary to help further clarify the ideal approach for these patients.
Footnotes
Authors’ contribution
XYY reviewed the data and contacted the authors; WQX and YZ helped with data extraction; T-ZM, Y-KG, H-YW and W-HW revised the article. All the authors obtained the important yet controversial data used in this article.
Acknowledgment
The authors thank Yun Yang, a student from Tianjin No. 1 High School Grade 11, for helping edit the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.