
Abstract
Aim
To evaluate the performance of two different flexible devices, the balloon-expandable BeGraft stent as on-label chEVAR use with the Endurant (Medtronic, Santa Rosa, USA) stent graft compared to the self-expandable off-label employment of Viabahn (Gore Flagstaff, Arizona, USA).
Methods
All patients treated for pararenal aortic pathologies between 2008 and 2017 using Endurant II (Medtronic, Santa Rosa, CA, USA) abdominal endograft in combination with Viabahn (Gore, Flagstaff, AZ, USA) or BeGraft (Bentley, Hechingen, Germany) at our institution were retrospectively analyzed. Patients were divided into two groups according to the employed chimney graft, namely Viabahn (group A) and BeGraft (group B). The primary endpoint was the incidence of type IA endoleak at one month and last follow-up. Secondary endpoints included reintervention rates, primary patency of the chimney graft, and need for additional placement of bare metal stents also known as relining.
Results
A total of 27 patients (mean age: 76 years) were treated with overall 47 chimney grafts. In particular, 11 patients received 21 Viabahn and 16 patients underwent placement of 26 BeGraft stents. Mean follow-up was 14.3 ± 9.0 months for group A and 13.0 ± 13.7 for group B, p = .451. The mean chimney graft length was 85.1 ± 38.9 mm for group A and 34.9 ± 9.8mm for group B (p < .001). The oversizing rate at the proximal sealing zone was significantly higher in group B (Group A: 23.1 ± 16.5% vs. Group B: 33.6 ± 7.6%, p = .007). The primary patency rates were similar between groups (p = .250). The subgroup analysis showed a significantly higher early (9–42.9% vs. 2–7.7%, p = .005) and at last CT follow-up (5–23.8% vs. 0–0.0%, p = .011) type IA endoleak, higher primary relining (14–66.7% vs. 5–19.2%, p = .001) and reintervention rates (5–23.8% vs. 0–0.0%; p = .011) for group A chimney stent grafts.
Conclusions
Both chEVAR combinations displayed similar patency rate, showing the BeGraft-Endurant composition less need for relining and fewer one-year type IA endoleak and reintervention rates in the subgroup analysis.
Introduction
The chimney endovascular technique (chEVAR) represents an alternative approach for the treatment of aneurysms featuring a short proximal neck, not suitable for a standard endovascular aneurysm repair. 1 The technique involves the placement of covered stents in the target branches, parallel to and outside the aortic stent graft. While growing off-label use of the technique and several devices over the last years led to rapidly expanding horizons and increasing applicability at many centers around the world,2,3 the heterogeneity of component combinations has contributed to the achievement of mixed results and the creation of some degree of skepticism regarding overall performance and its place in surgeons’ armamentarium.4,5
The chEVAR technique employs off-the-shelf use of standard abdominal endografts and different covered stents available on the market. The most profoundly evaluated and commonly used combination of these two components is the Endurant II (Medtronic, Santa Rosa, CA, USA) abdominal endograft with the Advanta/i-Cast V12 (Getinge, USA) as chimney stent. 6 As a result, the Endurant device received Conformité Européene (CE) approval to be employed with balloon-expandable covered stents (BECS). However, with the exception of in vitro studies,8,9 scarce clinical data are available on the use of stents other than Advanta BECS. 9
The BeGraft stent (Bentley InnoMed, Hechingen, Germany) is a cobalt chromium BECS with an indication for use (IFU) in renal arteries. The device is flexible, which can be beneficial in angulated renal arteries avoiding the need for endolining with flexible bare stents and minimizing the risk of occlusion. 10 Thus, it is preferred and has been widely employed in angulated target vessels. Recently, Spear et al. published their experience with BeGraft stents as bridging devices during fenestrated endovascular aortic aneurysms repair. 11 However, evaluation focusing on its performance within the chEVAR technique is lacking. Similarly, self-expandable covered stents (SECS) have been employed within chEVAR being preferred at our institution in angulated renal arteries due to their flexibility and a wide range of diameter and length. However, its applicability with the Endurant device is still an off-label combination.
The purpose of the present analysis is to evaluate the performance of two different flexible devices commonly employed within the chEVAR technique, the BeGraft stent as on-label chEVAR use compared to the off-label employment of SECS (Viabahn, Gore Flagstaff, Arizona, USA).
Methods
Prospectively collected clinical and radiographic data of all patients treated with chEVAR at our institution were retrospectively reviewed and analyzed. Between January 2009 and December 2017, 222 patients underwent chEVAR for treatment of abdominal aortic pathologies. All patients with placement of abdominal endografts other than Endurant II were excluded (n = 11). From the remaining 211 patients, bare metal stent and BECS combinations other than BeGraft (n = 184) were also excluded, leaving finally 27 patients for analysis. A total of 27 patients were treated with overall 47 chimney grafts. In particular, 11 patients received 21 SECS (Viabahn, Gore Flagstaff, Arizona, USA) and 16 patients received 26 BeGraft stents. Clinical charts were reviewed for demographic data, clinical history, and radiologic, and procedural details. The present study complies with the principles of the Declaration of Helsinki, and the data collection and acquisition were approved by the local ethics committee and institutional review board. The local ethics committee and institutional review boards approved data acquisition.
Indication for chimney
All patients considered candidates for chEVAR were deemed to be high-risk candidates for open surgical repair including several cardiovascular or anatomic comorbidities such as active chronic obstructive pulmonary disease, poorly controlled congestive heart failure, symptomatic coronary artery occlusive disease, American Society of Anesthesiologists score of 3 or more, previous myocardial infarction, coronary stent or bypass, and/or prior open abdominal aortic repair. Indication for chEVAR included symptomatic/ruptured cases and rupture threatening pathologies of the abdominal aorta such as penetrating aortic ulcer. Anatomical unsuitability for fenestrated/branched endografts (f-EVAR) including severe aortic neck angulation or calcification and stenosis or angulation of the iliac vessels was also an indication for chEVAR as reported by the participating centers.
Technical aspects
Chimney selection was driven by anatomical parameters. The BeGraft stent was considered for cases of particularly angulated target vessels due to their increased flexibility. SECS was preferred in similar angulated cases with, however, longer distance between the proximal covered end of the abdominal endograft and the target vessel. Endolining was performed with additional placement of a self-expanding bare metal stent to smoothen and reinforce the transition of the chimney graft in the kinked segment of the target vessel.
Follow-up protocol
A 1-mm-slice control computed tomography angiography (CTA) was performed during the first 30 days postoperatively, at 12 months, and then annually. All included patients had at least one CTA or MRA postoperatively. Duplex ultrasound examination was performed six months postoperatively and in case of renal insufficiency and contraindication to MRA. MRA was used to follow up patients with renal impairment or need of endoleak evaluation in case of significant aneurysm sack expansion defined as sack growth of more than 0.5 cm within six months, detected by CTA or duplex ultrasound. If the postoperative control imaging showed a type II endoleak, no changes were undertaken in the follow-up protocol. Reintervention was planned in case of significant aneurysmatic sac growth. If a chEVAR-related type IA endoleak was detected, additional three-month CTA was performed, and if it was persistent, a reintervention was implemented.
Image analysis and study endpoints
CTA data were analyzed using OsiriX MD v.8.5.2 (Pixmeo, Bernex, Switzerland). Measurements were made using a plane perpendicular to the aortic blood flow centerline. 12 The measurements on the blinded samples were performed independently by two vascular surgeons not involved in data collection (GTT and MVU).
Primary endpoints included aneurysm chimney graft patency and freedom from type I endoleak. Secondary endpoints included all-cause mortality, aneurysm-related mortality, chimney graft-related reinterventions, and need for relining.
Definitions
Pararenal pathologic processes include juxtarenal and suprarenal clinical entities such as degenerative aneurysms, penetrating atherosclerotic ulcers, type IA endoleaks after EVAR, and para-anastomotic aneurysms after previous open repair. Stent patency and endoleaks were defined by the Society for Vascular Surgery reporting standards. Chimney graft-related secondary procedures were labeled as reintervention due to restenosis >70% or occlusion of the chimney graft confirmed by angiogram.
Statistical analysis
Descriptive statistics were used to assess study demographics and outcome variables as appropriate. Continuous data were compared with non-parametric Mann-Whitney U test, as appropriate. Categorical data were analyzed by Pearson's Chi-square test. A p value of less than 0.05 was considered statistically significant for all analyses. Statistical analysis was performed using SAS Version 9.4 (SAS Institute, Cary NC, USA).
Results
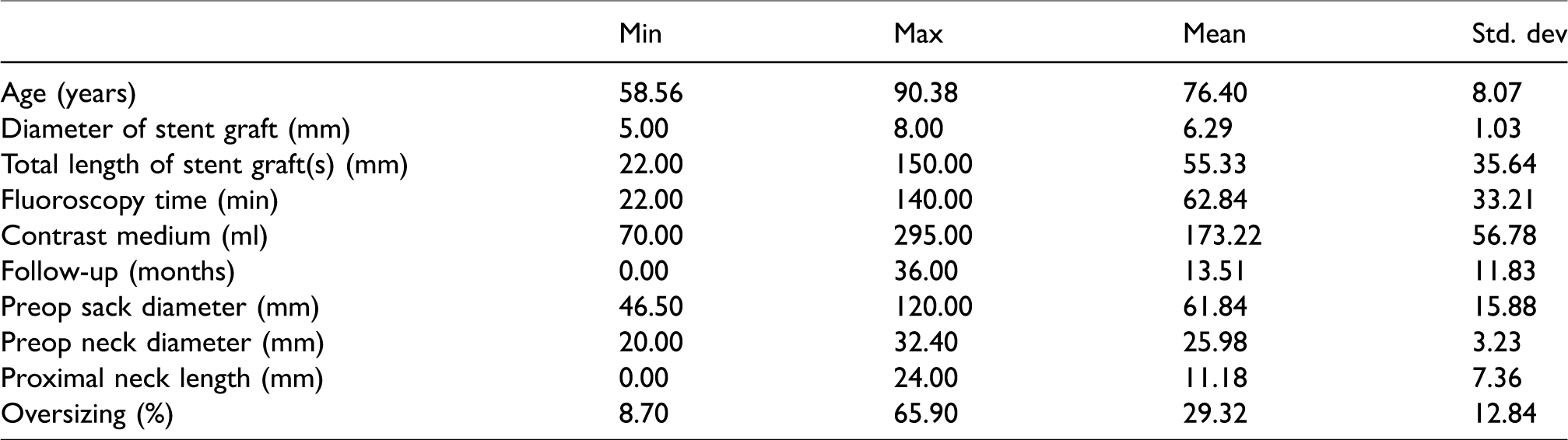
Mean age within the cohort was 76 ± 8 years. Table 1 shows demographics, anatomical features, and characteristics of the procedures. Mean preoperative sack diameter was 61.8 ± 15.8 mm with mean proximal neck length of 11.1 ± 7.3 mm. Mean oversizing was 29.3 ± 12.8%, while mean follow-up time of the entire cohort was 13.5 ± 11.8 months. The selected 27 patients were treated with overall 47 chimney grafts. In particular, 11 patients received 21 SECS and 16 patients received 26 BeGraft stents, respectively. Both groups showed similar fluoroscopic time (74.1 ± 40.4 vs. 55.1 ± 25.8 min) and contrast medium use (165.0 ± 59.1 vs. 178.9 ± 56.4 ml) (Table 2).
Demographics, anatomical, and operative data in the total series of 27 patients.
Comparison of clinical, anatomical, and intraoperative variables.
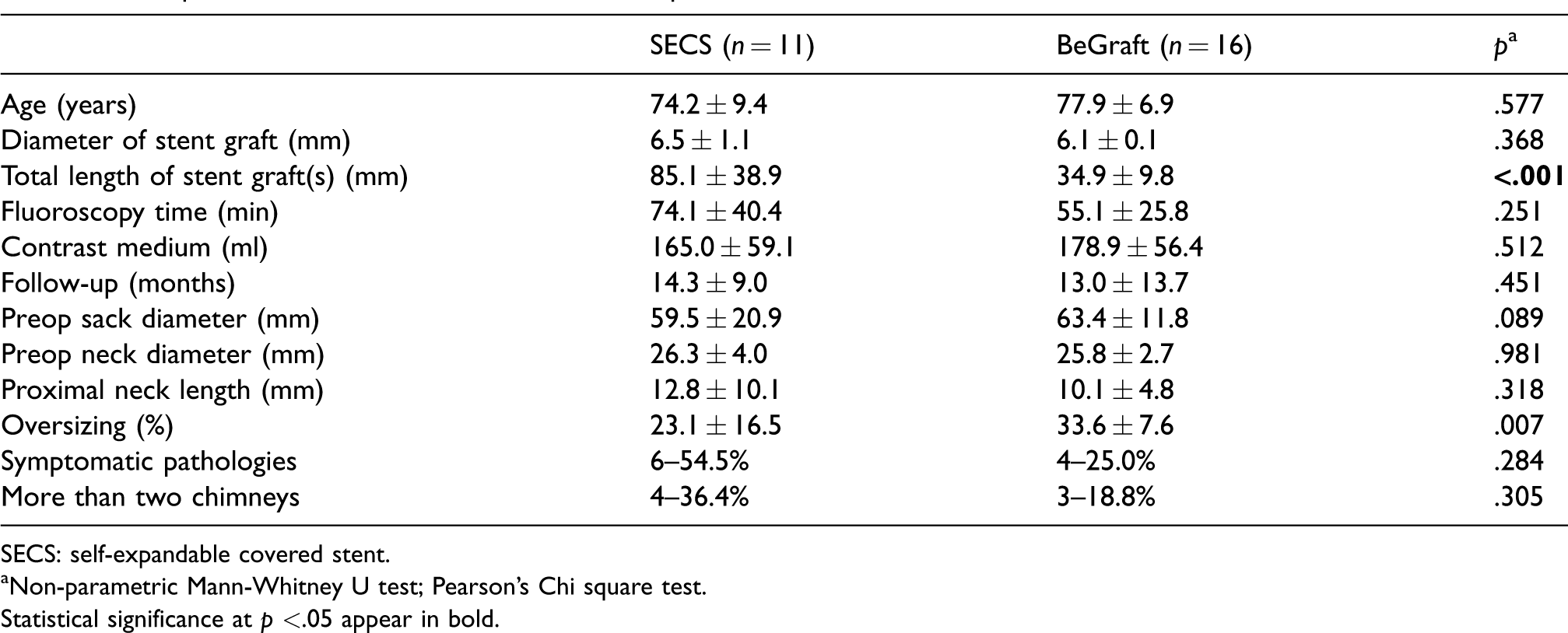
SECS: self-expandable covered stent.
Non-parametric Mann-Whitney U test; Pearson’s Chi square test.
Statistical significance at p <.05 appear in bold.
The SECS group had longer total stent length (85.1 ± 38.9 vs. 34.9 ± 9.8 mm, p < .001), while abdominal endograft oversizing was higher for the BeGraft group (23.1 ± 16.5 vs. 33.6 ± 7.6%, p = .007). No statistical differences were observed in terms of symptomatic repair (6–54.5% vs. 4–25.0%, p = .284) or multiple chimney use (>2) (4–36.4% vs. 3–18.8%, p = .305).
Both groups showed similar primary patency and 30-day mortality outcomes (Table 3). The SECS group showed higher primary relining rate (8–72.7% vs. 3–18.8%, p.005). No reinterventions due to chimney graft stenosis were performed in neither group during the study period. Two patients within the SECS group suffered renal chimney occlusion three and six months after the procedure, respectively. The first patient presented with flank pain while the second was asymptomatic. In both cases, an attempt for recanalization was endeavored without success due to stent graft compression at the proximal edge of the chimney graft. One patient within the BeGraft group presented asymptomatic renal chimney occlusion identified in the control CTA two years after the intervention, and thus conservative treatment was indicated. No patient required hemodialysis due to chimney graft occlusion. Early and late type IA endoleak (4–36.4% vs. 2–12.5%, p = .143 and 2–18.2% vs. 0–0.0%, p = .086, respectively) and reintervention rate (2–18.2% vs. 0–0.0%, p = .086) were higher in the SECS group without reaching statistical significance.
Clinical and radiological outcomes comparison between self-expandable covered stent (SECS) vs. BeGraft treated patients.
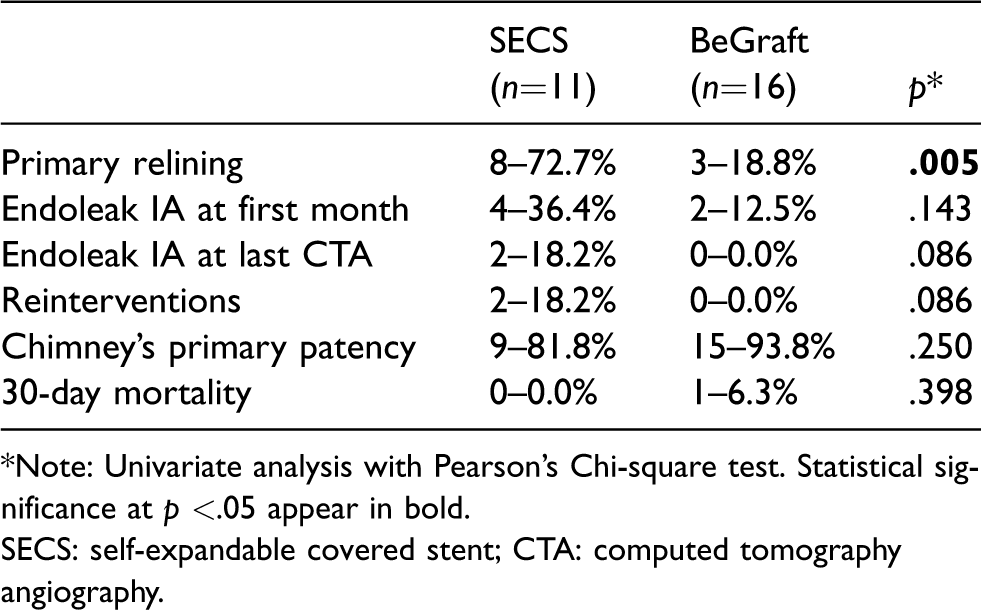
*Note: Univariate analysis with Pearson’s Chi-square test. Statistical significance at p <.05 appear in bold.
SECS: self-expandable covered stent; CTA: computed tomography angiography.
Subgroup analysis
The subgroup analysis per stent events showed similar primary patency (19--90.4% vs. 25--96.1%, p .250) and 30-day mortality results (0.0% vs. 6.3%, p = .398) (Table 4). The SECS group showed higher primary relining rate (14–66.7% vs. 5–19.2%, p = .001), early and late type IA endoleak (9–42.9% vs. 2–7.7%, p = .005 and 5–23.8% vs. 0–0.0%, p = .011, respectively), and reintervention rate (5–23.8% vs. 0–0.0%, p = .011).
Results of self-expandable covered stent (SECS) vs. BeGraft subgroups. Comparison in the total of 47 chimneys.

Note: Univariate analysis with Pearson’s Chi-square test. Statistical significance at p <.05 appear in bold.
SECS: self-expandable covered stent; CTA: computed tomography angiography.
Discussion
To our knowledge, the present analysis is the first clinical evaluation of the BeGraft stent in comparison with SECS in combination with the Endurant II abdominal endograft for chEVAR treatment of short proximal neck AAA. The operative parameters in terms of fluoroscopic and contrast medium time, indication for symptomatic pararenal pathology or more than two chimney stents application, as well as, primary patency and mortality were similar in both combinations. Although both stents behaved similarly per se, the subgroup analysis showed significantly more type IA endoleaks and reintervention rates within the SECS group.
In accordance to a previous metanalysis by our group, it seems like chimney graft occlusions tend to occur a few months after placement with generally asymptomatic clinical presentation when affecting the renal arteries, although in some cases, the patient may exhibit flank pain. 13 To our knowledge, chimney stent length has not been previously regarded as risk factor for chimney failure. However, the number of chimney grafts and stent graft relining have shown to be risk factors for chimney occlusion. 4 In our opinion, the differences observed in the present analysis stand rather in relation to the lower radial force of the Viabahn stent and its need for relining rather than the stent graft length itself. However, further analysis may regard this topic.
The PROTAGORAS study demonstrated the efficacy of the Endurant II abdominal endograft combined with a BECS, especially the Advanta/i-Cast V12 covered stent thereby receiving CE approval of this combination. 6 However, clinical evaluation of other BECS as on-label use within this technique has not been conducted up to now. Despite our small sample size, the here displayed data seem to compare to data displayed within the cited analysis. 6 One of the big issues related to the first generation BeGraft stent is device fracture and separation between the stent and the expanded polytetrafluoroethylene (ePTFE) cover.7 Compared with the first BeGraft generation, the second generation was modified by increasing the thickness of the ePTFE (from 100 mm to 200 mm) and the width of the stent connectors (by 20%), resulting in significantly improved radial force. Despite the apparent heterogeneity of the here employed BeGraft stents due to timeframe, no separation between components of the stent was observed during follow-up, and this BECS still showed better outcomes compared to Endurant-SECS. Spear et al. group recently evaluated the performance of 101 BeGraft devices as bridging stents for fenestrated endovascular aortic repair, showing also good results at one-year follow-up. 11 Vos et al. also showed favorable outcomes when using the BeGraft stent to proximally extend an iliac branch device for the treatment of isolated common iliac artery aneurysms. 14
There are a few in vitro studies evaluating device combinations for the chEVAR technique. Mestres et al.’s testings strived to find the most adequate parallel stent combinations and degree of oversizing combining different diameters of Endurant with BeGraft and Excluder with SECS. 8 Although a silicon model cannot be compared to an in vivo situation, the reported higher stent compression and risk of infolding with the Excluder-SECS combination confirm the displayed hereby worse outcomes when using SECS with a higher need for relining. A similar analysis was conducted by Overeem et al. 9
At our institution, SECS are preferred in angulated arteries with longer distance to the target vessel due to their large length availability. Still, the smaller radial force of the Viabahn results in compression at the major resistance points like the proximal edge of the main graft and the orifices of the target vessels increasing stent graft stenosis and finally, occlusion. Thus, SECS present higher relining need and their applicability in combination with the Endurant stent graft has to be individualized. The combination of this covered stent previously showed good midterm results with another abdominal endografts like the Excluder device (Gore, Flagstaff, AZ, USA) featuring infrarenal fixation and lacking suprarenal stents. 15 The similar radial force presented by both devices, achieving a harmonic semilunar shape around the SECS and minimizing the risk for persistent gutters may explain the favorable outcomes. In the same line, while different chEVAR combinations were displayed within the PERICLES registry showing good midterm results and confirming this technique as a valid alternative in the treatment of complex abdominal EVAR, a small number of SECS were associated with the Endurant device, demonstrating efficacy in case of long distance between the proximal end of the fabric and the target vessel. 2 Also, the reliability of this stent in case of preserving the accessory renal arteries with a chimney stent has been shown in another previous report. 16
Several limitations should be considered as for the retrospective nature of the present analysis and the relatively small number of patients. Data are self-reported lacking core laboratory analysis of clinical and radiological events. Also, our median follow-up period (13.5 months) was relatively short, and though it stretched to more than three years in some of the cases, longer follow-up is warranted. Although both compared stents are preferred in angulated renal arteries due to their proven flexibility, some essential differences which may have influenced the here driven results should be acknowledged. On one hand, the Viabahn stent has longer length availability, thus preferred in case of long distance between the proximal end of the fabric and the target vessel. However, its self-expandable nature demands a higher need for relining to avoid compression when used with the Endurant device. On the other hand, the BeGraft stent has higher radial force, though it requires bigger stent oversizing. Comparison between the BeGraft and the mainly employed Advanta/i-Cast V12 stent in our group was avoided in the present series due to the significant discrepancy in the number of treated patients which would fail to draw any robust conclusions. Consequently, we avoided to provide any comparison of findings with the published PROTAGORAS experience including the use of Advanta/i-Cast V12 in 128 patients and having a midterm CTA-based follow-up.
Conclusion
Even if both chEVAR combinations displayed similar patency rates, the BeGraft-Endurant composition required less relining compared to SECS-Endurant, showing less one-year type IA endoleaks and reintervention rates in the subgroup analysis. Further confirmatory studies are needed to confirm the present findings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.