
Abstract
Objective
This study was to assess the clinical features and prognostic factors of posterior circulation cerebral infarction (PCCI) patients.
Methods
A total of 165 PCCI patients who were admitted to the Department of Neurology, Beijing Friendship hospital, Capital Medical University between January 2016 and December 2016 were included. Patients had complete medical record and received 12-month follow-up. The demographics, risk factors, clinical manifestations, National Institutes of Health Stroke Scale (NIHSS) score and imaging findings were collected and factors affecting their prognosis were further analyzed.
Results
The mean age was 59.5 ± 10.8 years and the mean National Institutes of Health Stroke Scale (NIHSS) score on admission was 6.6 ± 2.8. The one-year recurrence rate of stroke was 6.7%; 84.8% of patients had good prognosis (modified Rankin Scale [mRS] score 0–3) and 15.2% had poor prognosis (mRS score >3). The one-year mortality was 3.0%. Patients with ≥50% stenosis in the basilar artery and higher NIHSS score were more likely to have poor outcome.
Conclusion
The majority of PCCI patients have a good prognosis and a low mortality. The prognosis is poor in patients with ≥50% stenosis in the basilar artery and higher NIHSS score on admission.
Keywords
Introduction
Stroke represents a major cause of morbidity and mortality worldwide and affects millions of people annually. In China, there are about 2.7 million new cerebrovascular disease cases each year, accounting for 1/3 of stroke patients worldwide. More than 65% of survived patients will develop disability of varying degrees. The cost related to the treatment of stroke in China is as high as 40 billion RMB each year and it is on the rise.
Ischemic stroke comprises 80%–90% of all the strokes. Approximately 20–25% of ischemic strokes occur in the posterior circulation, known as vertebrobasilar arterial system. 1 The recognition of symptoms of acute posterior circulation cerebral infarction (PCCI) in the acute stage is relatively difficult, possibly because of the complexity of the vertebrobasilar artery and brainstem anatomy. Therefore, fewer studies have been conducted to investigate the PCCI as compared to anterior circulation cerebral infarction.
Generally, PCCI has a poor prognosis and may cause high disability and mortality rates. With the development of neuroimaging and the advances in the diagnosis and treatment of cerebrovascular diseases, the prognosis of PCCI has been improved. In a widely accepted New England medical center posterior circulation registry (NEMC-PCR), results showed 284 patients had good prognosis among 361 patients (78.3%). 2
At present, venous ultra-early rt-PA (within 4.5 h) thrombolysis is still the gold standard for the treatment of ischemic stroke; for patients with moderate-to-severe neurological dysfunction due to the proximal aortic occlusion, intravascular recanalization within 6 h is safe and effective. However, due to time window limitation, safety and economic concern, only a very small number of patients receive thrombolytic and endovascular treatment. Currently, little is known about the factors related to the prognosis of PCCI.
In this study, a total of 165 patients with PCCI (patients with intravenous thrombolysis and endovascular treatment are not included) admitted to the Department of Neurology, Beijing Friendship Hospital, Capital Medical University between January 2016 and December 2016 were retrospectively reviewed. The factors affecting the prognosis were analyzed and compared with previous findings. Our findings may provide guidance for future clinical treatment of PCCI.
Materials and methods
This study was undertaken at the Neurology Department, Beijing Friendship Hospital of Capital Medical University. Among 1024 subjects with ischemic stroke admitted between January 2016 and September 2016, 165 patients with PCCI were retrospectively included and reviewed.
This study was approved by the Ethics Committee of Capital Medical University. All study protocol and procedure were conducted in accordance with the declaration of Helsinki.
The inclusion criteria were as follows: patients were aged >18 years; patients had PCCI on diffusion-weighted magnetic resonance imaging (DW-MRI) within 14 days after presentation.
Exclusion criteria were as follows: patients with other diseases other than ischemic stroke (bleeding, tumor, etc.) on cranial MRI; patients were admitted at >14 days after disease onset; patients underwent intravenous thrombolysis, or other surgical treatments in the Emergency Department; patients with moderate to severe mental disorders or dementia; patients with the modified Rankin Scale (mRS) score >2 before the disease onset.
Medical records were retrieved from the hospital database and following information was reviewed: demographics, risk factors (hypertension, diabetes, hyperlipidemia, hyperhomocysteinemia, heart disease, history of ischemic stroke, history of hemorrhagic stroke, smoking status, drinking status), laboratory findings as well as National Institutes of Health Stroke Scale (NIHSS) scores.
Imaging examination
The posterior circulation was divided into the proximal, middle and distal segments based on the post-circulation vascular dominance zone segmentation criteria used in NEMC-PCR. The vascular lesions were identified by computed tomography angiogram (CTA), magnetic resonance angiography (MRA), vertebral artery ultrasound, transcranial Doppler (TCD), or digital subtraction whole brain angiography (DSA). All imaging examinations were performed by two experienced radiographers who were blind to the patient's characteristics. Discrepancy was resolved by consulting the third imaging specialist.
Follow-up
The prognosis was assessed at 3, 6 and 12 months after disease onset. The following information was included: recurrent cerebrovascular events (cerebral infarction or transient ischemic attack [TIA]); cerebral hemorrhage; rehospitalization for endovascular treatment or bypass surgery; death of any causes (including death of cerebrovascular and non-cerebrovascular causes); occurrence of cardiovascular events and other vascular events; mRS scores in follow-up period. The prognosis was classified based on the mRS scores: no disability (mRS 0 to 1), mild disability (mRS 2 to 3), severe disability (mRS 4 to 5) and death (mRS 6); mRS score of 0–3 suggests a good prognosis, and mRS score of >3 was indicative of a poor prognosis.
Statistical analysis
SPSS version 20 for Windows was used for statistical analysis. The univariate regression analysis was performed on the potential prognostic factors, followed by multivariate logistic regression analysis of those with significance in univariate analysis. A value of P < 0.05 was considered statistically significant.
Results
Clinical characteristics
A total of 165 patients were included in this study. The mean age was 59.5 ± 10.8 years and the mean NIHSS score on admission was 6.6 ± 2.8. There were 123 (74.5%) males and 42 (25.5%) females. The most common risk factor was hypertension (n = 114; 69.1%), followed by history of smoking (n = 94; 57.0%), hyperlipidemia (n = 91; 55.2%), diabetes mellitus (79; 47.9%), and history of drinking (n = 63). Among them, 41 (24.8%) had a history of stroke, and 30 (18.2%) had pre-existing hyperhomocysteinemia. In addition, 34 had heart disease (20.6%) and 11 had atrial fibrillation (6.7%).
At the time of initial presentation, paresis was found in 81 (49.1%) patients, dizziness in 77 (46.7%), dysarthria in 41 (24.8%), ataxia in 9 (5.5%), diplopia in 9 (5.5%), headache in 4 (2.4%), seizures in 1 (0.6%) and impaired consciousness in 4 (2.4%).
The posterior circulation was divided into the proximal, middle and distal segments based on the post-circulation vascular dominance zone segmentation criteria used in NEMC-PCR. Lesions of the proximal segment were found in 31 patients (18.8%), lesions of the middle segment in 62 (37.6%), and lesions of the distal segment in 58 (35.1%). Lesions of >2 segments were found in 14 (8.5%) patients who were included in the mixed group.
Among these patients, 126 (76.4%) had a single lesion, which was found in the pons (n = 55), cerebellum (n = 20), medulla oblongata (n = 10), thalamus (n = 32), occipital lobe or temporal occipital lobe (n = 5), midbrain (n = 3) and pons medulla oblongata junction (n = 1). There were 39 lesions (23.6%) with multiple lesions, of which 10 cases (6.1%) had anterior circulation infarction.
Radiographic examinations suggested vertebrobasilar artery stenosis (≥50%) or occlusion in 77 patients. In these patients, stenosis involved a single vessel in 56 patients (33.9%) and multiple vessels in 21 patients (12.7%). The most common vascular stenosis was extracranial vertebral artery (ECVA), which accounted for 22.4% (n = 37), followed by anterior inferior cerebellar artery (ICVA), posterior cerebral artery (PCA), basilar artery (BA), and superior cerebellar artery (SCA). Moreover, 38 patients had the simultaneous stenosis (≥50%) or occlusion of the intracervical system.
Prognosis
One year after disease onset, 11 patients (6.7%) had recurrent ischemic stroke (cerebral infarction or TIA), including posterior circulation ischemic stroke (n = 8) and anterior circulation ischemic stroke (n = 3). Of the 11 patients, the recurrent ischemic stroke occurred within 3 months in 7 patients, within 3–6 months in 1 patient, and within 6 to 12 months in 3 patients. In addition, cerebral hemorrhage (n = 1), neoplastic stroke (new oncology; n = 1), re-hospitalization for endovascular treatment (n = 5), and cardiovascular events (n = 6) were also noted in the patients. No apparent disability was found in 87 patients (52.7%), mild disability in 53 (32.1%), serious disability in 20 patients (12.1%), and death in 5 patients (3.0%) at 1 year after disease onset. Twenty-five patients had a poor prognosis, accounting for 15.2%, the mean age of them was 64.76 ± 12.09 years, and there were 16 males and 9 females.
Prognostic factors
Univariate regression analysis showed, compared with patients with good prognosis, patients with poor prognosis were older, had higher NIHSS score on admission, and had a higher prevalence of heart disease and drinking (P < 0.05) (Table 1).
Factors related to the prognosis of PCCI in univariable regression analysis.
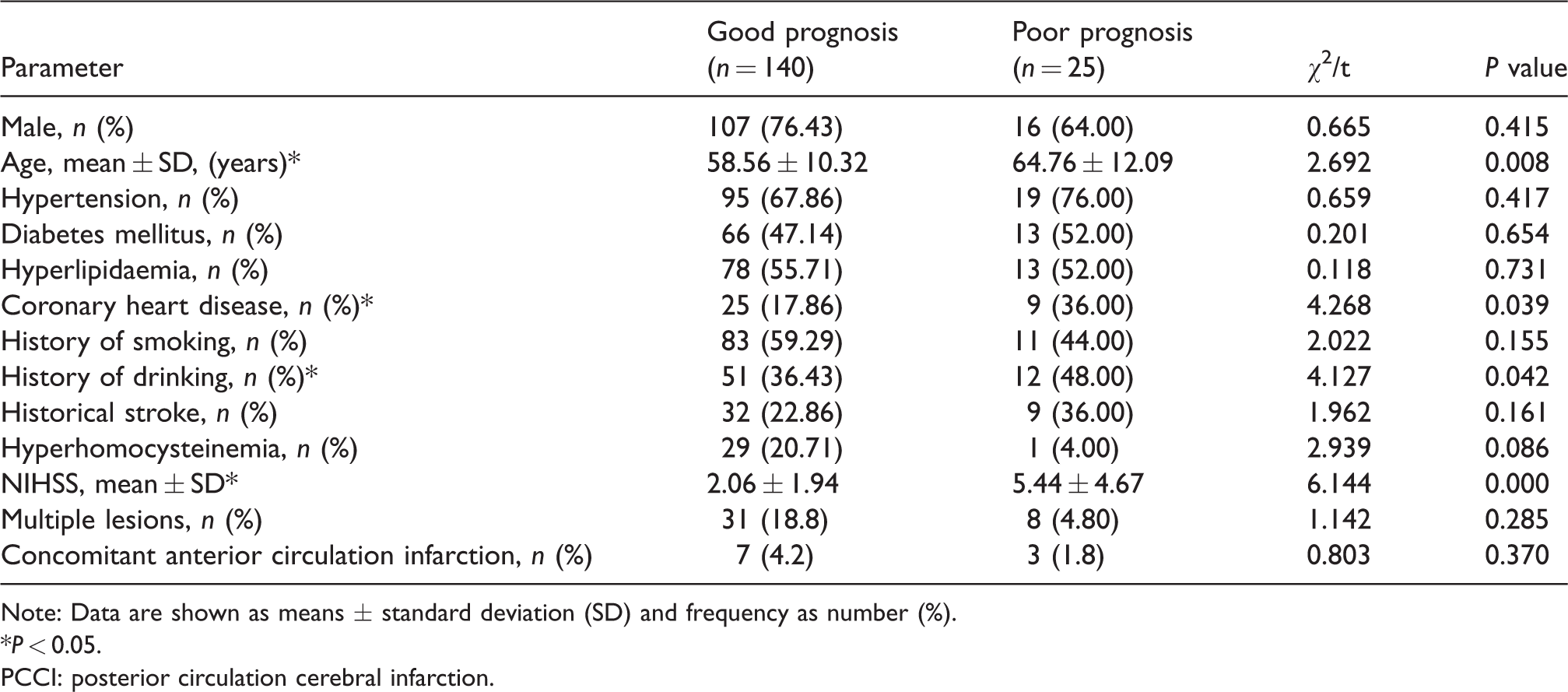
Note: Data are shown as means ± standard deviation (SD) and frequency as number (%). *P < 0.05.
PCCI: posterior circulation cerebral infarction.
Multivariate logistic regression analysis showed that the NIHSS score on admission and BA lesions (stenosis ≥50%) was independent risk factors for one-year prognosis in PCCI patients (Table 2).
Multivariable logistic regression analysis of factors related to the one-year prognosis of PCCI.
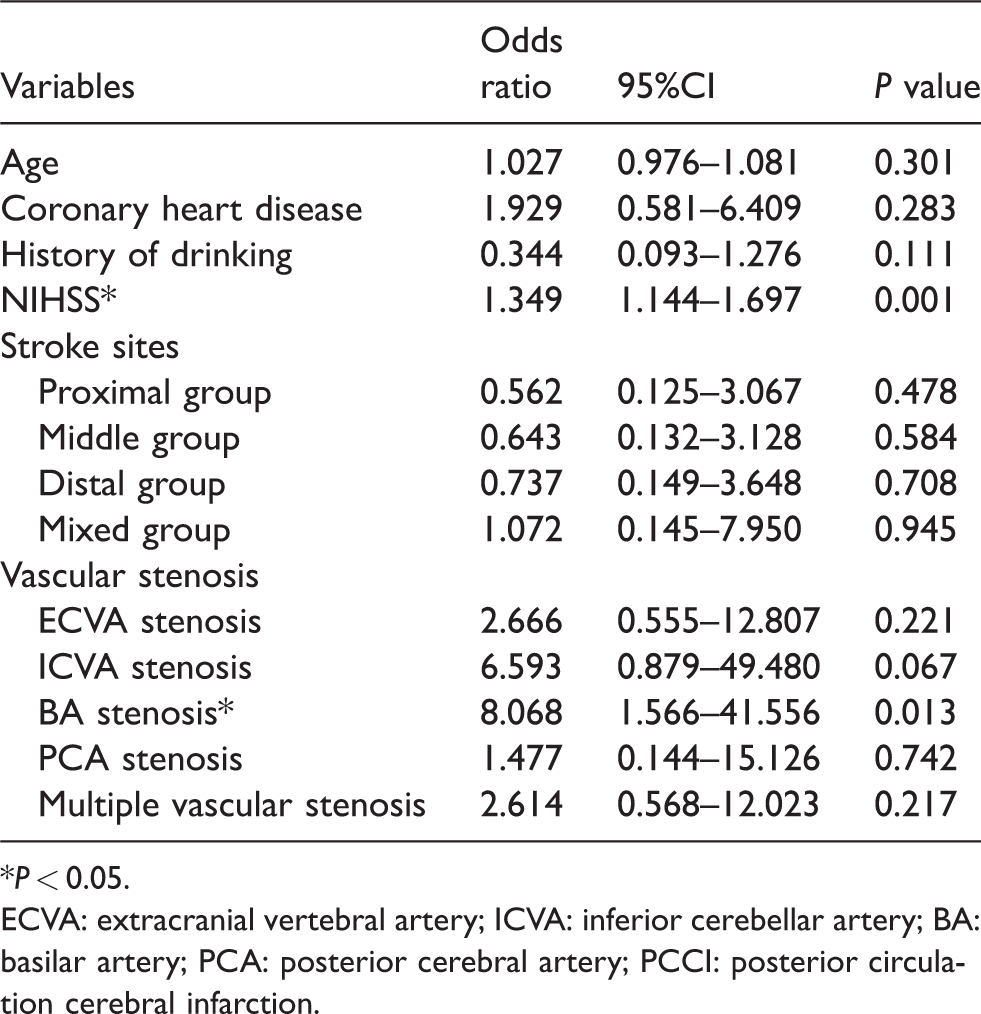
*P < 0.05.
ECVA: extracranial vertebral artery; ICVA: inferior cerebellar artery; BA: basilar artery; PCA: posterior cerebral artery; PCCI: posterior circulation cerebral infarction.
Discussion
The posterior circulation, also known as the vertebrobasilar system, consists of vertebral arteries, basilar arteries, posterior cerebral arteries and its branches. It supplies the brainstem, cerebellum, base of temporal lobe, occipital lobe, and thalamus. Post-circulatory ischemia accounts for about 20% of ischemic strokes. Compared with the anterior circulation, the posterior circulation has a large variation in the shape and branching. In addition, in the posterior circulation, a considerable part of the tissue is supplied by the small perforator artery. 3 The anatomical characteristics of these vessels make them highly susceptible to changes in lumen volume and hemodynamics, resulting in ischemic lesions. However, relative to the pre-circulatory cerebral infarction, fewer studies have been conducted to investigate PCCI, and currently, the prognosis of PCCI and its influencing factors are still poorly understood.
The anatomic structure and physiological functions of the posterior circulation are complex, and the regions supplied by the posterior circulation involve a variety of important structures and regions such as the cranial nerve, reticular upward activation system, ascending and descending nerve conduction bundles, and even respiratory centers and other life centers. When the blood supply is disordered, the core or contact fibers that are highly concentrated may be affected. Therefore, the clinical manifestations of PCCI are complex and vary, and when the disease is serious, the prognosis will be poor, but sometimes the diagnosis of PCCI is very difficult due to its complexity. In this study, the common symptoms and signs of PCCI were unilateral limb weakness (49.1%), dizziness (46.7%), unilateral numbness (24.8%), dysarthria (24.8%) and dysphagia (10.3%). Although cross-symptoms or signs are characteristics of PCCI, it is not common and was found in only six cases (3.6%) in this study. This was consistent with previously reported. 4 Dizziness is the most common symptom in NEMC-PCR studies, 2 accounting for 47%. Dizziness is a common symptom of PCCI, because the vestibular nucleus is superficial in the brainstem, has a long conduction path and thus is sensitive to ischemia. Most of the dizziness caused by PCCI will be accompanied by the symptoms of cerebellum or brainstem, but for the old patients with isolated dizziness who have risk factors of cerebrovascular diseases, posterior circulation ischemia should be considered. The brainstem reticular upward activation system is responsible for the maintenance of consciousness. If the lesion involves this structure, consciousness disturbance may be present. Therefore, consciousness disturbance is also a common clinical manifestation of PCCI. Previous studies have shown that the incidence of consciousness disturbance in PCCI is approximately 10%–20%.5,6 In this study, only four patients (2.4%) experienced consciousness disturbance, which was also associated with other neurological deficits. This may be ascribed to the neuroimaging examination which makes recognition of relatively mild PCCI easier. In addition, all the patients included in this study were inpatients, some of whom had received treatments in the Emergency Department. This might also be related to the lower prevalence of consciousness disturbance in this study.
Because of the complex anatomy of the posterior circulation system and the diverse clinical manifestations, PCCI generally has a poor prognosis, high morbidity and high mortality. It has been reported that the mortality rate of PCCI is above 25%, and the risk of PCCI recurrence is higher than that of anterior circulation ischemia.7,8 However, the development of neuroimaging examinations 9 improves the diagnosis of PCCI 10 and great progress has also been achieved in the treatment of cerebrovascular diseases, which improves the prognosis of PCCI. The NEMC-PCR Center study showed 78.7% of patients with PCCI had a good prognosis. 2 A follow-up study of 101 patients with brainstem infarction revealed the recurrence rate was 9.8% at one year and the mortality rate was 11.7%. 11 Another study showed patients with PCCI had lower mortality rate at one month, three months and one year than those with anterior circulation ischemia (3.93%, 5.3%, and 9.7% vs. 7.26%, 9.3%, 13.7%, P < 0.05), and the proportion of patients with PCCI who had a poor prognosis at one year after disease onset was also lower than that of patients with anterior circulation ischemia (6.5% vs. 15.2%, P < 0.01). 12 Among the 165 PCCI patients in this study, the recurrence rate at three months and one year after disease onset was 4.2% and 6.7%, respectively; 15.2% of patients had a poor prognosis, and the mortality rate was 3.0%. These results show the overall prognosis of PCCI is good. The discrepancy as compared to previously reported might be ascribed to the source of cases, the sample size and the techniques used for the diagnosis and treatment.
There are many factors that affect the prognosis of PCCI, but the available factors are still controversial. NEMC-PCR study showed the BA stenosis was an independent risk factor of poor prognosis in patients with PCCI. In the Chinese intracranial atherosclerosis (CICAS) study, repeated TIA attacks, arterial stenosis ≥70%, multiple-site infarction and no antithrombotic therapy at discharge were found as the factors for stroke recurrence. Caplan et al. found multifocal lesions were independent risk factors of prognosis in patients with PCCI.
In this study, 77 patients had post-circulatory vascular lesion, accounting for 46.7%, which is consistent with previously reported. ECVA lesions were the most common, and most of the lesions were located at the origin of the vertebral artery. However, multivariate analysis showed ECVA lesions were not the independent risk factors affecting the one-year prognosis of PCCI. This may be due to the fact that, when there is a severe stenosis or occlusion at one vertebral artery, the brain can compensate for the ischemic state of the posterior circulation through collateral circulations, including the anastomosis of the cervicothoracic and vertebral artery, muscular branches of the external carotid artery, the posterior ICVA, the pial branch of the PCA, and the posterior communicating artery, etc., and the blood flow of the contralateral vertebral artery will also increase as a compensation, thereby ensuring the supply of the BA.
The clinical prognosis of BA lesions varies widely. Some patients die or remain severely disabled, while others only have minor disabilities or even no sequelae at all. The prognosis of BA lesions is related to the severity, location and extent of thrombosis, it's association with vascular disease at other parts of the circulation, and the condition of collateral circulation. Most studies have shown that BA lesions are independent risk factors of poor prognosis in PCCI patients. The risk for poor prognosis in patients with BA lesions is five times that in patients with other independent factors. 13 A Japanese study also found that PCCI with large arterial lesions of the BA had a higher disability rate at three months. 14
In addition, our results also showed high NIHSS score on admission was associated with poor prognosis. The NIHSS score has been widely used to reflect the severity of acute cerebral infarction. Higher NIHSS score suggests more serious disease, susceptibility to disease progression and worse prognosis. Compared with the anterior circulation ischemia, NIHSS is less sensitive to the PCCI, because the NIHSS score is not high when PCCI patients have neurological deficits except for limb weakness. However, patients with high NIHSS score at early stage are more likely to develop significant disability or even die. Some investigators have proposed a more sensitive e-NIHSS (expanded NIHSS) scale, which requires to be validated in more studies. 15
In this study, high blood pressure (69.1%) was the most common risk factor of PCCI. Another study also revealed hypertension was a risk factor of PCCI (OR, 1.090; 95% CI, 1.001–1.109; P = 0.027) compared with the anterior circulation-related stroke. 16 However, multivariate analysis showed these common risk factors of stroke such as hypertension, diabetes mellitus, hyperlipidemia, history of smoking, history of heart disease, and hyperhomocysteine failed to affect the prognosis of PCCI in our study. This may be due to the presence of multiple risk factors in the majority of these patients.
In summary, the clinical manifestations of PCCI are complex, which is related to the difference in its prognosis. In this study, the prognosis of PCCI was studied, and results showed PCCI patients did not have a poor prognosis as traditionally considered. The severity of BA lesions and high NIHSS score on admission were found to be associated with poor prognosis.
More multi-center clinical studies with large sample size and long-term follow-up are required to provide further insight into the clinical features and prognosis of PCCI. With the increasing awareness of stroke and the improvement of diagnosis and treatment, the prognosis of PCCI will be significantly improved in the future.
Conclusion
The majority of PCCI patients have a good prognosis with a low mortality rate. The prognosis is relatively poor in patients with ≥50% stenosis in the BA and higher NIHSS score on admission.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No. 81671191).