
Abstract
Objectives
We evaluated the necessity of revascularization for acute mesenteric ischemia in symptomatic patients with spontaneous isolated dissection of the superior mesenteric artery.
Methods
This retrospective study included 28 consecutive, symptomatic patients with spontaneous isolated dissection of the superior mesenteric artery treated at our hospital between December 2005 and December 2017. Patients with concomitant aortic dissection were excluded. We reviewed the patients’ clinical presentation; laboratory evaluations; computed tomography findings, including the true lumen residual ratio (i.e., the minimum true lumen size compared to the diameter of the transverse section of the dissected artery) at the time of admission; the number of patients who were suspected of having bowel ischemia; and the number of patients who required surgical or endovascular treatment and their outcomes. Additionally, to evaluate the true lumen residual ratio in symptomatic patients with bowel ischemia, the true lumen residual ratio in those with abnormal laboratory data were compared with that in those without abnormal laboratory data. Initial true lumen residual ratio values were also compared with final values. Furthermore, we assessed the clinical details of patients who had bowel necrosis. Categorical variables were compared using the χ2 test or Fisher’s exact test. Continuous values were presented as either the mean ± standard deviation or median (interquartile range 25–75), and the variables were analyzed using Student’s t-test or the Mann–Whitney U test.
Results
The patients’ age ranged between 41 and 85 years, and 25 were men. Although nine patients were suspected of having acute mesenteric ischemia, only one underwent bowel resection. None of the patients had an indication for revascularization. The true lumen residual ratio of the nine patients with abnormal laboratory data were significantly lower than those of the 19 without abnormal laboratory data (10 [0–25]% vs. 40 [20–50]%, p = 0.005). The patient who underwent bowel resection had a true lumen residual ratio of 10%; however, there was no obvious abnormal laboratory data suggestive of bowel necrosis. Dissections were managed conservatively in all patients. True lumen residual ratio increased from initial value of 30 (10–48)% to 98 (60–100)% at the final imaging study (p < 0.0001). There were no adverse events related to the mesenteric circulation during the follow-up period of 2–11 years.
Conclusions
Reintervention is rarely required for spontaneous isolated dissection of the superior mesenteric artery, even in symptomatic patients, and spontaneous resolution of the luminal compromise is the rule.
Keywords
Introduction
Several recent studies have reported that most patients with spontaneous isolated dissection of the superior mesenteric artery (SIDSMA) can initially be treated conservatively.1–5 However, acute mesenteric ischemia (AMI) is a rare but life-threatening complication.6–8 Recent review articles have reported that symptomatic patients managed conservatively have relatively high late secondary intervention rates. 9 Therefore, the decision to perform revascularization in patients with SIDSMA is challenging and must consider the optimal timing and interventional approach, and which patients stand to benefit.
The aim of this study was to evaluate the necessity of revascularization for AMI in symptomatic patients with SIDSMA.
Methods
This retrospective study included 28 consecutive, symptomatic patients with SIDSMA treated at our hospital between December 2005 and December 2017. All patients presented with acute onset abdominal pain. The diagnosis of SIDSMA was made on the basis of multi-detector computed tomography (CT) findings. Patients with concomitant aortic dissection were excluded from the study.
We reviewed the following information: clinical presentation; laboratory and CT findings on admission; the number of patients who were suspected of having bowel ischemia; the number of patients who required surgical or endovascular treatment on admission; the type of treatment; the number of patients who required additional treatment; and the patients’ outcomes.
The CT findings included the true lumen residual ratio (TLRR; i.e., the minimum value of the true lumen size compared to the transverse section of the dissected artery), 2 length of the dissected artery, maximum diameter of the dissected artery, blood flow through the branches of the superior mesenteric artery (SMA) (i.e., the middle colic, inferior pancreaticoduodenal, inferior pancreatic, jejunal, right colic, and ileocolic arteries), and other visceral arteries (i.e., the celiac artery [CA] and inferior mesenteric artery [IMA]), and contrast effect of the bowels. Additionally, to evaluate the effectiveness of TLRR as an indicator for AMI in symptomatic patients with SIDSMA, the TLRR in patients with abnormal laboratory data were compared to those in patients without abnormal laboratory data. Moreover, the initial TLRR values were compared with final values.
Furthermore, we assessed the clinical details of patients who experienced bowel necrosis, underwent laboratory evaluations, and had CT findings including TLRR.
Statistical analysis
Statistical analyses were performed using SPSS software (Windows version 22.0; SPSS Inc., Chicago, IL). The values are presented as either mean ± standard deviation for normally distributed data or median (interquartile range (IQR) 25–75) for non-normally distributed data. Categorical variables were compared using the χ2 test or Fisher’s exact test, and continuous variables were analyzed using Student’s t-test or the Mann–Whitney U test. Statistical significance was defined as a p value of less than 0.05. The cutoff value of TLRR was calculated using receiver operating characteristics (ROC) curve analysis based on TLRR and the ratio of patients with abnormal laboratory data. Our university’s ethics review board approved this study (18 R-067) and waived the need for consent of the patient because of the retrospective design and minimal risk to human subjects.
Results
Baseline patient characteristics are shown in Table 1. This study included 25 men and 3 women, all of whom were Japanese. None of the patients had a clinical or family history of arterial dissections, connective tissue diseases, or viral or bacterial infections based on the results of our hematological examinations.
Patient characteristics.
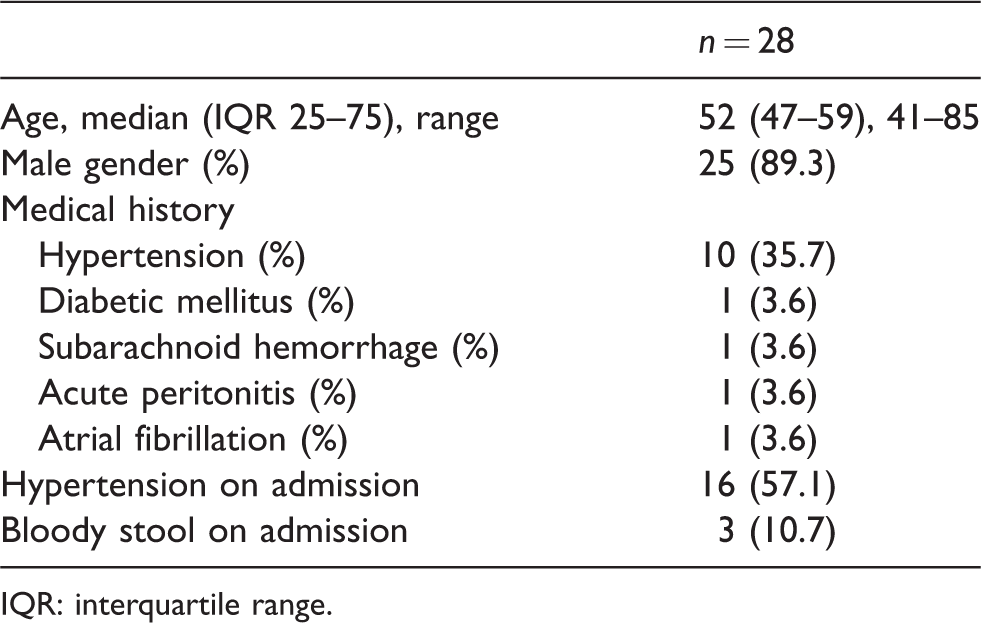
IQR: interquartile range.
The number of patients who had abnormal laboratory findings on admission and the maximum abnormal values are shown in Table 2. There were nine patients with at least one abnormal test result. Abnormalities in white blood cell (WBC) count were observed in five patients, in lactate level in 6, in D-dimer level in 7, and base deficit in 1 patient. Results of the other laboratory data including the serum amylase level were normal.
Laboratory evaluations.

The initial CT findings are shown in Table 3A. The TLRR of the nine patients with abnormal laboratory data was significantly lower than that of the 19 without abnormal laboratory data (10 [0–25]% vs. 40 [20–50]%, p = 0.005) (Table 3B). The cutoff value of TLRR to achieve the highest Youden index was 15% (sensitivity, 84.2%; specificity, 77.8%). The area under the curve was 0.822 (p = 0.007). The proportion of patients with TLRR <15% was significantly higher among those abnormal laboratory findings (77.8% vs. 15.8%, p = 0.003) (Table 3B).
CT findings.
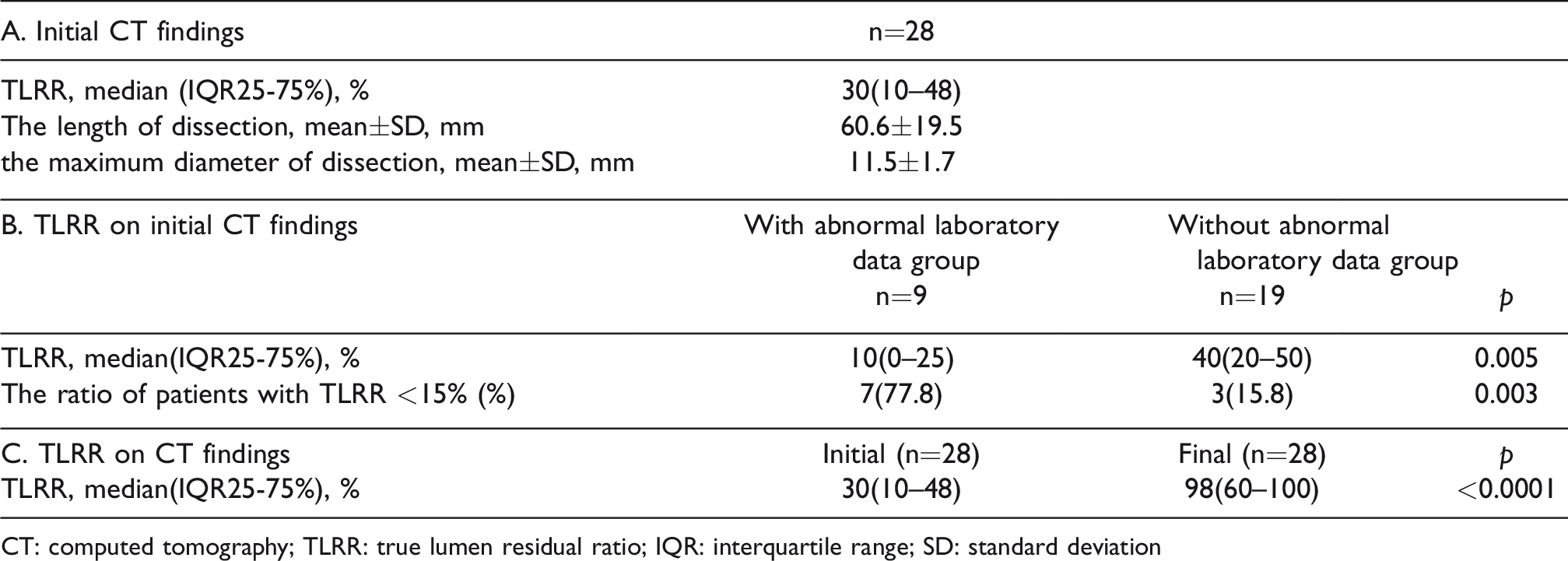
CT: computed tomography; TLRR: true lumen residual ratio; IQR: interquartile range; SD: standard deviation
There were nine symptomatic patients with abnormal laboratory data who were suspected of having AMI on admission. Although three who were strongly suspected of having AMI underwent exploratory laparotomy, only one was found to have bowel necrosis irreversible localized necrosis and underwent right hemicolectomy of part of the transverse colon. None of the patients had an obvious indication for revascularization on admission for AMI, including the patient who underwent bowel resection. Dissections were managed conservatively without endovascular or surgical intervention in all patients.
The patients’ abdominal pain was relieved within a few days of conservative treatment and the analgesics could be stopped. The follow-up CT findings in 14 patients showed almost complete improvement within a mean period of eight months (range 3–20 months). The other patients also showed gradual improvement. TLRR increased from initial value of 30 (10–48)% to 98 (60–100)% at the final imaging study (p < 0.0001) (Table 3C). There were no adverse events related to the mesenteric circulation during the follow-up period of 2–11 years.
Regarding the patient who exhibited bowel necrosis, although the WBC count and D-dimer level were increased at 19,800/mm3 and 0.8 μg/mL, respectively, the other laboratory data were normal. CT showed that the CA and IMA were patent; however, no blood flow through the middle colic artery and jejunal arteries could be observed and the TLRR was 10% (Figures 1–4).

Axial computed tomography angiogram in the arterial phase. Blood flow through the middle colic artery has disappeared (arrow), and the true lumen residual ratio is approximately 10% (arrowhead).

Computed tomography angiogram in the arterial phase. Blood flow through the celiac artery and inferior mesenteric artery is maintained. The arrows in A, B, and C indicate the superior mesenteric artery, celiac artery, and inferior mesenteric artery, respectively.
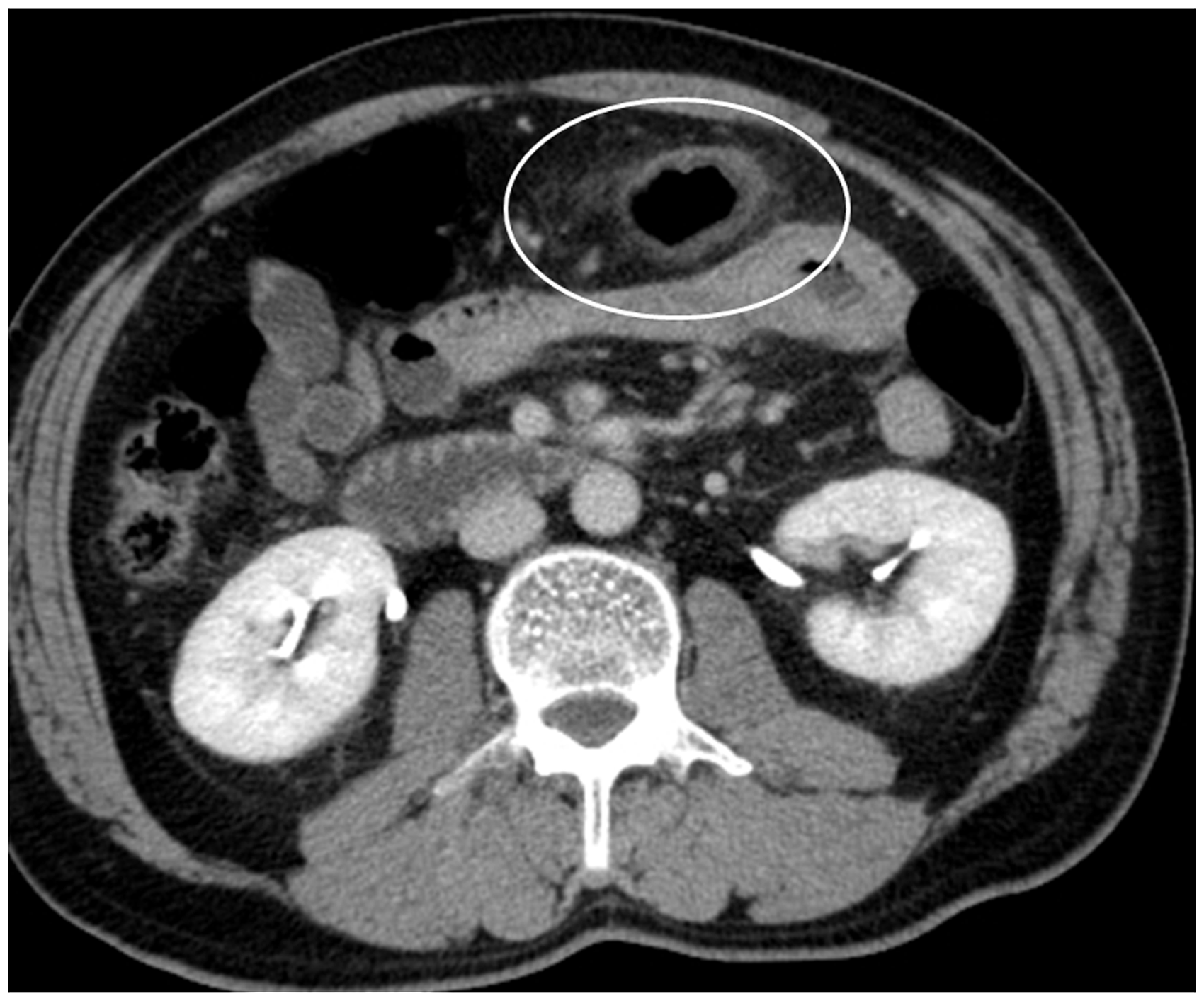
Computed tomography in the delayed phase. The circle indicates the part of the transverse colon that has swelled and weakened. As shown, the area is surrounded by fatty tissue.

Three-dimensional volume rendered computed tomography angiogram showing the narrow true lumen of the dissected artery (arrowhead). The arrows of A, B, and C indicate the superior mesenteric artery, celiac artery, and inferior mesenteric artery, respectively.
Discussion
The main finding of this study was that none of the patients with symptomatic SIDSMA had an obvious indication for revascularization for AMI. The majority of patients could be treated conservatively. Therefore, the decision of whether to proceed with revascularization remains challenging.
Recent reviews regarding SIDSMA reported that the majority of patients were treated conservatively. Additional treatment is required in only a minority of patients receiving conservative treatment.5,9,10 However, the definitive indications for additional treatment remain unclear.
Previous studies have reported some markers that may point to a diagnosis of AMI. Increased D-dimer and lactate levels may assist physicians in diagnosing AMI.6,11–14 CT should be performed as soon as possible for any patient suspected of having AMI.15–18 Several scoring systems and predictive factors to help in diagnosing AMI have also been reported. 19 However, their effectiveness in determining the necessity for revascularization in patients with SIDSMA remains unclear. Therefore, we believe that a multidisciplinary approach is currently needed until a superior management strategy is developed.
We diagnosed AMI in patients with SIDSMA when the following clinical and CT findings were present: the presence of pronounced and persistent abdominal pain, an increased lactate or D-dimer level, and CT findings suggestive of ischemic change.
Although nine patients were diagnosed with AMI in this study, only one required surgical management and underwent bowel resection without revascularization. As the blood flow through the resected margins was maintained, revascularization was not performed. This patient achieved complete recovery without additional interventions. Moreover, after dissection, all patients, including the patient who underwent bowel resection, improved naturally without endovascular or surgical treatment of their dissection. Ultimately, we determined that none of the patients had an obvious indication for revascularization.
Although the TLRR in the patients who were diagnosed as having AMI was <15%, the incidence of AMI in those with TLRR <15% was 70.0% (7/10), because 10 patients had TLRR was <15%, including those with normal laboratory findings. The incidence of bowel necrosis in patients with TLRR <15% was 10.0% (1/10). These results suggested that absolute TLRR values might be a good predictor of AMI, but not bowel necrosis or revascularization.
Endovascular treatment has continued to develop rapidly and has been proven to be clinically successful.11–24 It has been commonly used in patients with AMI due to its less invasive nature.21–24 Further, many studies have reported the use of stents for patients with AMI caused by SIDSMA.5,25–27 This approach may be effective for preventing the progression of bowel necrosis. However, it remains controversial because of some reported failures.26,27 In addition, there are no obvious indications for revascularization for AMI in patients with SIDSMA. Our results suggest that the actual number of patients who require revascularization may be fewer than previously reported. 5 Unnecessary treatment should be avoided, and further studies to determine the precise indications may be needed.
This study has several limitations. It was a single-center, retrospective study with a small sample size. A randomized control trial, although ideal, might be impossible to perform because of the relative rarity of this disease. Therefore, additional investigations are needed to validate our results.
We conclude that even in symptomatic SIDSMA patients, intervention is rarely required and spontaneous resolution of the luminal compromise can be expected. It is necessary to elucidate the definitive indications for revascularization in patients with SIDSMA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Presentation information
Not applicable.