
Abstract
Objectives
Data about the circulating levels of cyclophilin A and matrix metalloproteinase-9 in stable coronary artery disease are contradictory. Moreover, their relationship in this disease is not established yet. Thus, this study was designed to assess the relationship between the circulating levels of cyclophilin A and matrix metalloproteinase-9 in coronary artery disease patients with and without type 2 diabetes mellitus (T2DM).
Methods
Serum levels of cyclophilin A, matrix metalloproteinase-9, and high sensitive C-reactive protein (hsCRP) along with fasting blood glucose, glycated hemoglobin, serum lipids, and the anthropometric parameters were measured in 120 participants who were divided equally into four groups (i) normal controls, (ii) T2DM patients, (iii) stable coronary artery disease patients with T2DM, and (iv) stable coronary artery disease patients without T2DM.
Results
Levels of cyclophilin A and matrix metalloproteinase-9 were significantly elevated in sera of coronary artery disease patients with and without T2DM compared to normal controls and T2DM patients. In multiple linear regression models, only cyclophilin A was observed in the final model where it explained the 24.9% variability of matrix metalloproteinase-9. Additionally, high circulating levels of cyclophilin A and matrix metalloproteinase-9 were associated with an increased risk of developing stable coronary artery disease. Finally, the diagnostic efficacy of cyclophilin A and matrix metalloproteinase-9 to discriminate stable coronary artery disease patients with and without T2DM from subjects without coronary artery disease was found to be higher than that of hsCRP.
Conclusion
Serum level of cyclophilin A might be a determinant factor of matrix metalloproteinase-9 level; both may contribute to the pathogenesis of stable coronary artery disease and they appear to be valuable diagnostic biomarkers of stable coronary artery disease with and without T2DM.
Keywords
Introduction
Because of its association with clustered risk factors such as hyperglycemia, dyslipidemia, hypertension, and obesity, type 2 diabetes mellitus (T2DM) is considered as a major risk factor affecting coronary artery disease (CAD) which remains, despite advances in diagnosis and treatment, the first cause of mortality and morbidity of cardiovascular disease (CVD). The latter is the leading cause of death worldwide.1,2 Thus, and compared to non-diabetics, diabetic patients have a 2–4 folds greater risk of developing CAD which appears to be more severe, more rapidly progressive, and commonly found as a multi-vessel disease. Accordingly, 75% of T2DM patients die as a consequence of CVD, including CAD.3,4
Cyclophilin A (CyPA) is a protein belongs to the immunophilin family which was initially thought to function primarily as an intracellular protein, where it plays an important role in intracellular signaling, protein folding and trafficking, and regulating the activity of other proteins. However, it was reported that CyPA can be secreted by cells in response to reactive oxygen species (ROS), and its secretion is regulated by excessive activation of Rho-kinase which plays a crucial role in inflammation, vascular contraction, and the development of atherosclerosis.5–8 Previous studies demonstrated a significantly higher circulating level of CyPA in patients with CAD in proportion to the severity of the disorder.9,10 Moreover, its level was found to be significantly higher in CAD patients with T2DM. 11
Matrix metalloproteinases (MMPs) are a large family of zinc-dependent, extracellular endopeptidases, responsible for the degradation of extracellular matrix and adhesion proteins. MMP-9 (gelatinase B) is a 92 kDa gelatinase (type IV collagenase) enzyme which represents the largest and most complex member of this family. 12 In the last few years, MMP-9 attracted a growing interest in human pathology; Welsh et al. showed an association of serum MMP-9 with the incidence of coronary heart disease in the general population. 13 Further, a higher level of MMP-9 in patients with CAD has been reported, was a correlate of coronary artery ectasia, and a predictor of increased mortality in CAD patients.14–16
Extracellular matrix metalloproteinase inducer, also named CD147, is a single trans-membrane glycoprotein that can stimulate MMP production via mitogen-activated protein kinase pathway,17,18 and it serves also as a signaling receptor for extracellular cyclophilins.19,20 It was demonstrated that the production of MMP-9 during foam cell formation is regulated by CD147 and its ligand CyPA. 21
Thus, these observations raised the possibility that the activation of CyPA/CD147/MMP-9 pathway may play a relevant role in promoting the vulnerability of atherosclerotic plaques and may CyPA be strongly associated with MMP-9 in stable CAD patients. Therefore, the present study was designed to explore the relationship between the circulating levels of CypA and MMP-9 in stable CAD patients with and without T2DM, their possible implication in the pathogenesis, and their diagnostic efficacy for the detection of the disease.
Subjects and methods
Study population
This was an observational study conducted on T2DM patients and stable CAD patients with and without T2DM. Patients who had coronary angiographically proven stable angina (SA) pectoris and evidence of ischemia on exercise electrocardiogram or a positive treadmill exercise stress test (>1 mm ST-segment depression) were enrolled. The degree of coronary stenosis was assessed, and a narrowing of the lumen by more than 51% of the diameter was considered to indicate clinically significant stenosis. The left anterior descending coronary artery, left circumflex coronary artery, and right coronary artery were examined to evaluate the number of stenotic coronary arteries, and patients were classified according to the severity of CAD on a scale of 0–3 as having no clinically significant organic stenosis, or stenosis in 1-, 2-, or 3-blood vessels, respectively. On the other hand, fasting blood glucose (FBG) level ≥126 mg/dl, on two occasions, in the presence of glycated hemoglobin (HbA1c) level >6.5% was used to assess the presence of T2DM.
Exclusion criteria were the existence of unstable angina, myocardial infarction, acute coronary syndrome, heart failure (left ventricular ejection fraction <50%), peripheral vascular disease, nephropathy, retinopathy, any infectious or systematic inflammatory disease, hematologic disorders, thyroid dysfunction, severe liver and/or renal insufficiency, malignancy, and pregnancy.
One hundred and twenty subjects participated in this study; they were divided equally into four groups: (i) normal healthy volunteers, (ii) T2DM patients, (iii) stable CAD patients with T2DM, and (iv) stable CAD patients without diabetes mellitus.
All patients were sequentially recruited from Cardiovascular and Ultrasonography Unit, Research Institute of Ophthalmolog, Giza, Egypt in the period from August 2016 to September 2017. Informed written consent was obtained from all participants included in the study. This work was carried out in accordance with The Declaration of Helsinki for experiments involving humans and the study protocol was approved by the local ethical committee.
Five milliliters of 12 h fasting venous blood were collected from each participant. A part of the sample (4 ml) was collected into dry tubes, left to clot, and centrifuged at 2000 × g for 5 min to obtain sera which were immediately separated and stored frozen at –80°C until assayed within batches. Another part of the sample (1 ml) was collected into ethylene diamine tetra-acetic acid (EDTA)-coated tubes for the determination of HbA1c level.
Anthropometric and biochemical parameters
Anthropometric indices including height (m), weight (kg), waist circumference (WC), and hip circumference (HC) were measured using standardized equipments and then body mass index (BMI) as weight/height 2 (kg/m2) and the waist-to-hip ratio (WHR) were calculated. Blood pressure was measured using standard methods after at least 10 min rest in a sitting position.
Biochemical analyses of FBG, serum total cholesterol (TC), triglycerides (TG), and high-density lipoprotein-cholesterol (HDL-C) levels were carried out using enzymatic-based available commercial kits provided by Biodiagnostics (Giza, Egypt) on Roche Hitachi 912 chemistry analyzer (Roche Diagnostics, In, USA) and low-density lipoprotein-cholesterol (LDL-C) concentration was calculated using the Friedewald’s formula. 22
The level of HbA1c was determined in whole blood using high-performance liquid chromatography with the use of D-10 Hemoglobin Testing System (Bio-Rad Laboratories, Inc., CA, USA).
Assays for hsCRP, CyPA, and MMP-9
Serum levels of high sensitive C-reactive protein (hsCRP) (Cat# CSB-E08617h), CyPA (Cat# CSB-E09920h), and MMP-9 (Cat# CSB-E08006h) were determined by commercial sandwich enzyme-linked immunosorbent assay kits according to the manufacturer’s instructions (Cusabio, TX, USA). The lower limit of detection of the assays was 0.156 ng/ml for hsCRP, 0.78 ng/ml for CyPA, and 0.284 ng/ml for MMP-9. The intra-assay and inter-assay coefficients of variation of the assays were <8% and <10%, respectively. The tests were performed on ChroMate® microplate reader (Awareness Technology Inc., FL, USA).
Statistical analysis
The assumption of Gaussian distribution was tested with the Shapiro-Wilk test; the Gaussian distributed data were expressed as mean±SD, non-Gaussian distributed data were expressed as median and interquartile range (25th and 75th percentile), and categorical variables are expressed as frequencies (percentages). Continuous variables were compared using unpaired Student’s t-test, one-way ANOVA followed by Tukey’s post hoc for multiple comparisons or Kruskal-Wallis test followed by Dunn post hoc for multiple comparisons as appropriate. χ2 test was used to compare the differences between categorical variables. After a significant crude correlation was found, multiple linear regression models with a subsequent backward stepwise procedure were used to assess the association of MMP-9 with different parameters. All stepwise selection models used a p < 0.05 level for entry and a p < 0.10 for removal, and variables to be included in these models were based on the previous simple regression analyses. Potential confounders were adjusted using partial correlation. To investigate the strength of the association between the circulating levels of CyPA, MMP-9, and the susceptibility to CAD, unconditional logistic regression analyses were performed. The strength of the association was measured by crude odd ratio (OR), adjusted OR, and their corresponding 95% confidence interval (CI). To determine the diagnostic value of CyPA as well as MMP-9, receiver operating characteristic (ROC) curve analysis was performed. All p-values were two-sided, and a p-value <0.05 was considered statistically significant. Analyses were performed using SPSS version 20.0 (IBM Corp, NY, USA).
Results
Demographic and clinical data of the studied groups
The general demographic and clinical characteristics of the subjects in addition to the medication history of the patients are presented in Table 1. There was no statistically significant difference between all subjects in age, sex distribution, smoking habits, and diastolic blood pressure. Compared to the control group, CAD patients with and without T2DM had significantly higher WC, WHR, and BMI (p < 0.001). Moreover, they had significantly higher WC (p < 0.001 and p = 0.014, respectively), WHR (p = 0.001 and p = 0.005, respectively), and BMI (p = 0.001 and p = 0.003, respectively) in comparison with T2DM patients. Regarding HC, CAD patients without T2DM had significantly higher measurements compared to controls only (p = 0.009). On the other hand, CAD patients with T2DM showed a significantly elevated systolic blood pressure in comparison with control group (p = 0.007).
General characteristics of the studied groups.
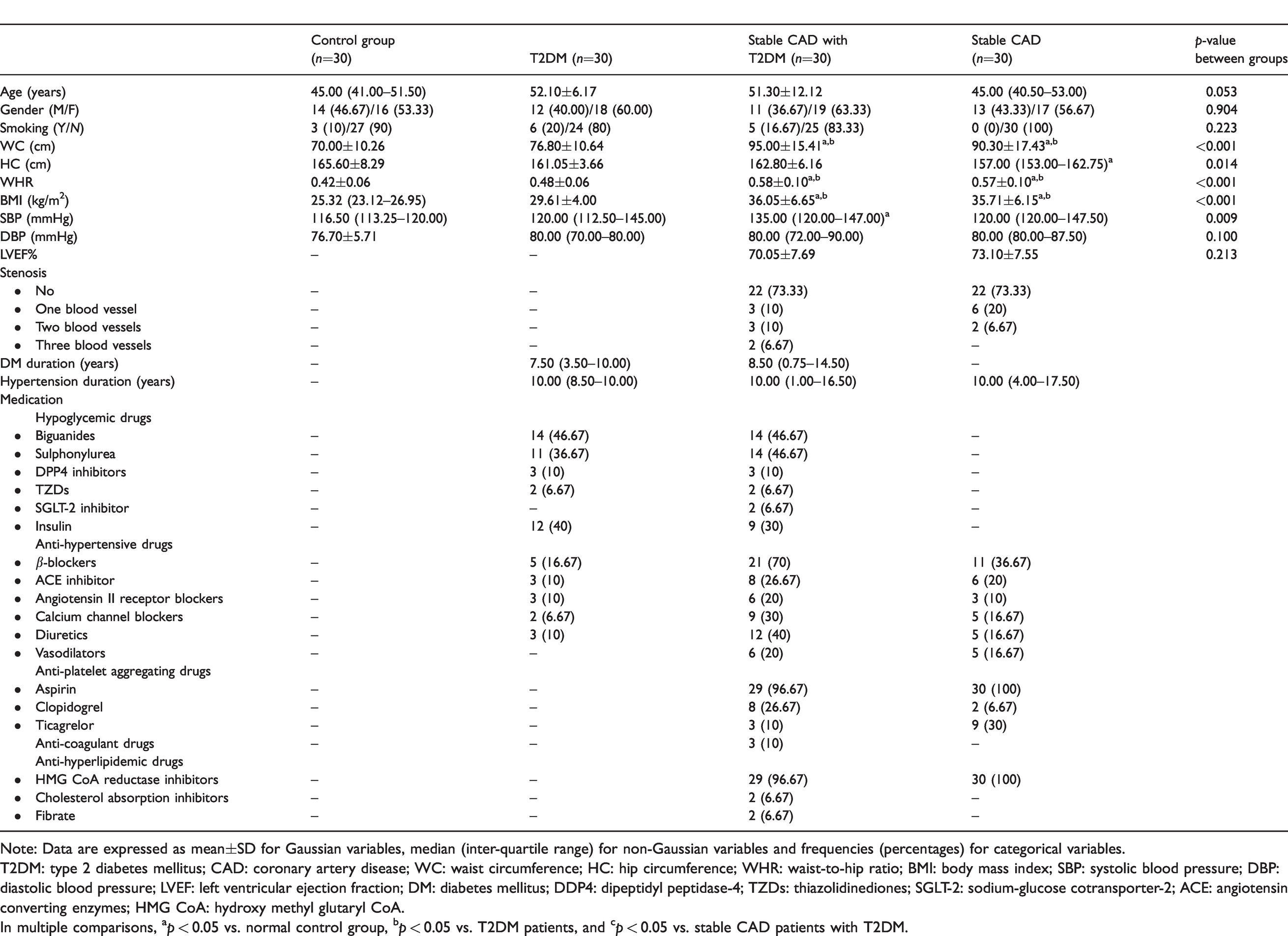
Note: Data are expressed as mean±SD for Gaussian variables, median (inter-quartile range) for non-Gaussian variables and frequencies (percentages) for categorical variables.
T2DM: type 2 diabetes mellitus; CAD: coronary artery disease; WC: waist circumference; HC: hip circumference; WHR: waist-to-hip ratio; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; LVEF: left ventricular ejection fraction; DM: diabetes mellitus; DDP4: dipeptidyl peptidase-4; TZDs: thiazolidinediones; SGLT-2: sodium-glucose cotransporter-2; ACE: angiotensin converting enzymes; HMG CoA: hydroxy methyl glutaryl CoA.
In multiple comparisons, ap < 0.05 vs. normal control group, bp < 0.05 vs. T2DM patients, and cp < 0.05 vs. stable CAD patients with T2DM.
Levels of some biochemical parameters, CyPA and MMP-9
The comparison of various biochemical parameters, CyPA and MMP-9 levels between the studied groups is shown in Table 2. For serum lipids, T2DM patients showed significantly higher levels of TC and TG compared to the control group (p = 0.016, and p = 0.009, respectively). Further, CAD patients with T2DM had a significantly elevated TG level in comparison with healthy controls and T2DM patients (p < 0.001 and p = 0.010, respectively), while their TC level was only borderline significantly higher compared to controls (p = 0.059). Moreover, TC and TG levels were significantly elevated in CAD patients without T2DM compared to healthy controls (p < 0.001), while they had a significantly elevated LDL-C level as compared to controls and CAD patients with T2DM (p = 0.025). Regarding HDL-C, a significantly lower level was noted in T2DM patients in comparison with healthy controls and CAD patients with T2DM (p = 0.002, and p = 0.003, respectively).
Serum levels of hsCRP, CyPA, MMP-9 and some biochemical parameters in the studied groups.
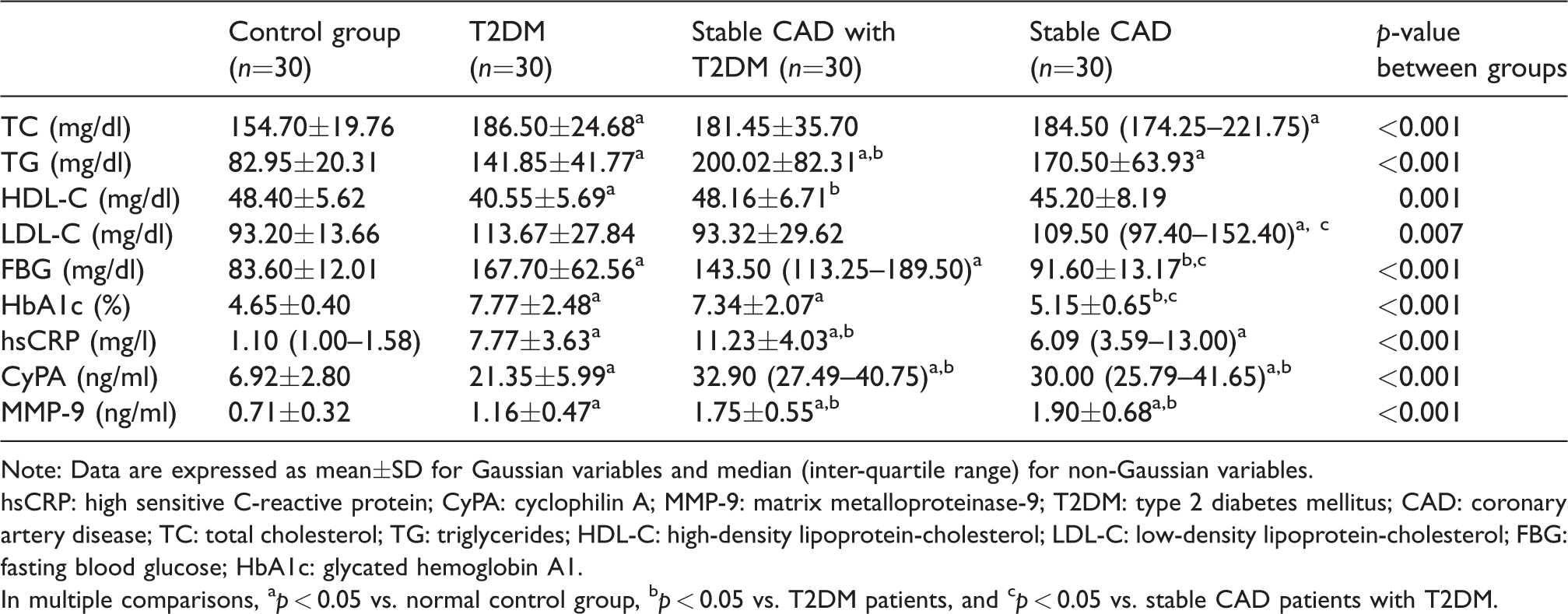
Note: Data are expressed as mean±SD for Gaussian variables and median (inter-quartile range) for non-Gaussian variables.
hsCRP: high sensitive C-reactive protein; CyPA: cyclophilin A; MMP-9: matrix metalloproteinase-9; T2DM: type 2 diabetes mellitus; CAD: coronary artery disease; TC: total cholesterol; TG: triglycerides; HDL-C: high-density lipoprotein-cholesterol; LDL-C: low-density lipoprotein-cholesterol; FBG: fasting blood glucose; HbA1c: glycated hemoglobin A1.
In multiple comparisons, ap < 0.05 vs. normal control group, bp < 0.05 vs. T2DM patients, and cp < 0.05 vs. stable CAD patients with T2DM.
The glycemic results including FBG and HbA1c were significantly higher in T2DM patients and CAD patients with T2DM, as expected, compared to healthy controls and CAD patients without T2DM (p < 0.001).
Compared to controls, serum hsCRP level was significantly elevated in T2DM patients and in CAD patients with and without T2DM (p < 0.001). Meanwhile, CAD patients with T2DM had a significantly higher hsCRP level as compared to T2DM patients (p = 0.019) and a borderline significant increase compared to CAD patients without T2DM (p = 0.052).
When considering serum CyPA, T2DM patients and CAD patients with and without T2DM demonstrated significantly elevated levels compared to healthy controls (p = 0.001 and p < 0.001, respectively). Further, CAD patients with and without T2DM had significantly higher levels compared to T2DM patients (p < 0.001).
With regard to serum MMP-9, significantly elevated levels were observed in T2DM patients and CAD patients with and without T2DM compared to controls (p = 0.037 and p < 0.001, respectively). Further and compared to T2DM, CAD patients with and without T2DM had significantly higher levels (p = 0.003 and p < 0.001, respectively).
Association of different parameters with serum MMP-9 level
When a significant crude correlation was found, multiple linear regression models with a subsequent backward stepwise procedure were used to assess the association of MMP-9 with different parameters. Table 3 shows the initial model, an intermediate model, and the final model of multiple linear regression models. The final model revealed just one relationship; it was a positive relationship between MMP-9 and CyPA and explained the 24.9% variance in MMP-9. The appropriate sample size and power calculations for regression analysis were carried out using the G*Power software version 3.1.9.2 (Düsseldorf University, Germany); calculations showed that our sample size can give as high as 95% power at the level of α error probability = 0.05.
Backward stepwise multiple regression models with MMP-9 as a dependent variable.
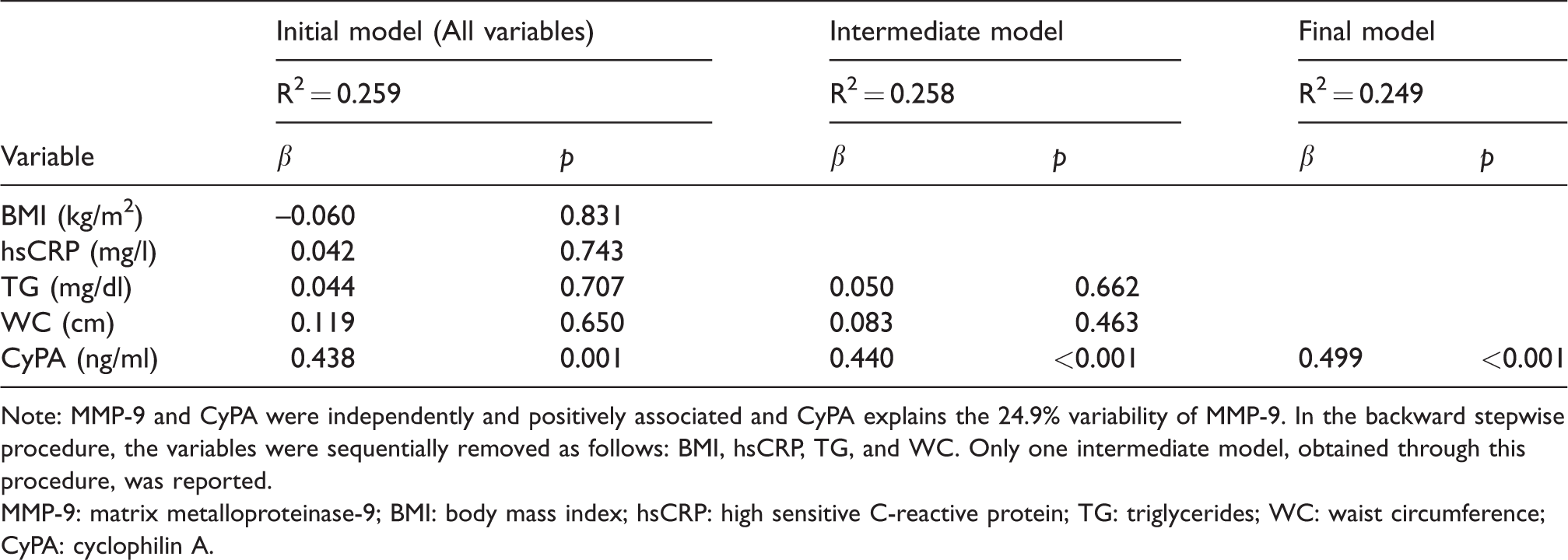
Note: MMP-9 and CyPA were independently and positively associated and CyPA explains the 24.9% variability of MMP-9. In the backward stepwise procedure, the variables were sequentially removed as follows: BMI, hsCRP, TG, and WC. Only one intermediate model, obtained through this procedure, was reported.
MMP-9: matrix metalloproteinase-9; BMI: body mass index; hsCRP: high sensitive C-reactive protein; TG: triglycerides; WC: waist circumference; CyPA: cyclophilin A.
To adjust for age, sex, smoking, BMI, systolic blood pressure, diastolic blood pressure, TC, TG, LDL-C, hypoglycemic drugs, and anti-hypertensive drugs as potential confounding factors, partial correlation of serum levels of MMP-9 with serum levels of CyPA was carried out. The relationship was persisted after adjusting for the potential confounders (r= 0.382, p = 0.001).
CyPA and MMP-9 as risk factors for stable CAD
Table 4 shows the results of the binary logistic regression analyses which were performed to test the associations of hsCRP, CyPA, and MMP-9 circulating levels with stable CAD risk, regardless with or without T2DM. The results demonstrated that serum levels of the three parameters were associated with an increased risk of stable CAD. However, after adjusting for age, sex, smoking, BMI, systolic blood pressure, diastolic blood pressure, TC, TG, and LDL-C as potential confounders, the results remained significant for only CyPA and MMP-9.
Binary logistic regression analysis of hsCRP, CyPA, and MMP-9 as factors possibly affecting stable coronary artery disease.

hsCRP: high sensitive C-reactive protein; CyPA: cyclophilin A; MMP-9: matrix metalloproteinase-9; OR: odd ratio; 95% CI: 95% confidence interval.
aAdjusted for age, sex, smoking, BMI, systolic blood pressure, diastolic blood pressure, TC, TG, and LDL-C as potential confounders.
Efficacy of hsCRP, CyPA, and MMP-9 as potential diagnostic biomarkers for stable CAD
Figure 1 illustrates the ROC curves of hsCRP, CyPA, and MMP-9 serum levels to diagnose stable CAD, whether with or without T2DM. The figure shows that CyPA had the strongest diagnostic value for CAD with an area under curve (AUC) of 0.954 (95% CI: 0.912–0.955, p < 0.001) and an optimal cut-off point of 23.69 ng/ml that associated with the parameter’s corresponding validity of 96.67% sensitivity and 85% specificity. However, the AUC of MMP-9 was 0.888 (95% CI: 0.812–0.964, p < 0.001) at a cut-off point of 1.27 ng/ml, which could yield sensitivity and specificity of 85%. On the other hand, hsCRP showed the lowest diagnostic efficacy among the three parameters with AUC of 0.812 (95% CI: 0.720–0.903, p < 0.001) that can give as high as 96.67% sensitivity and 56.67% specificity at a cut-off point of 2.93 mg/l.
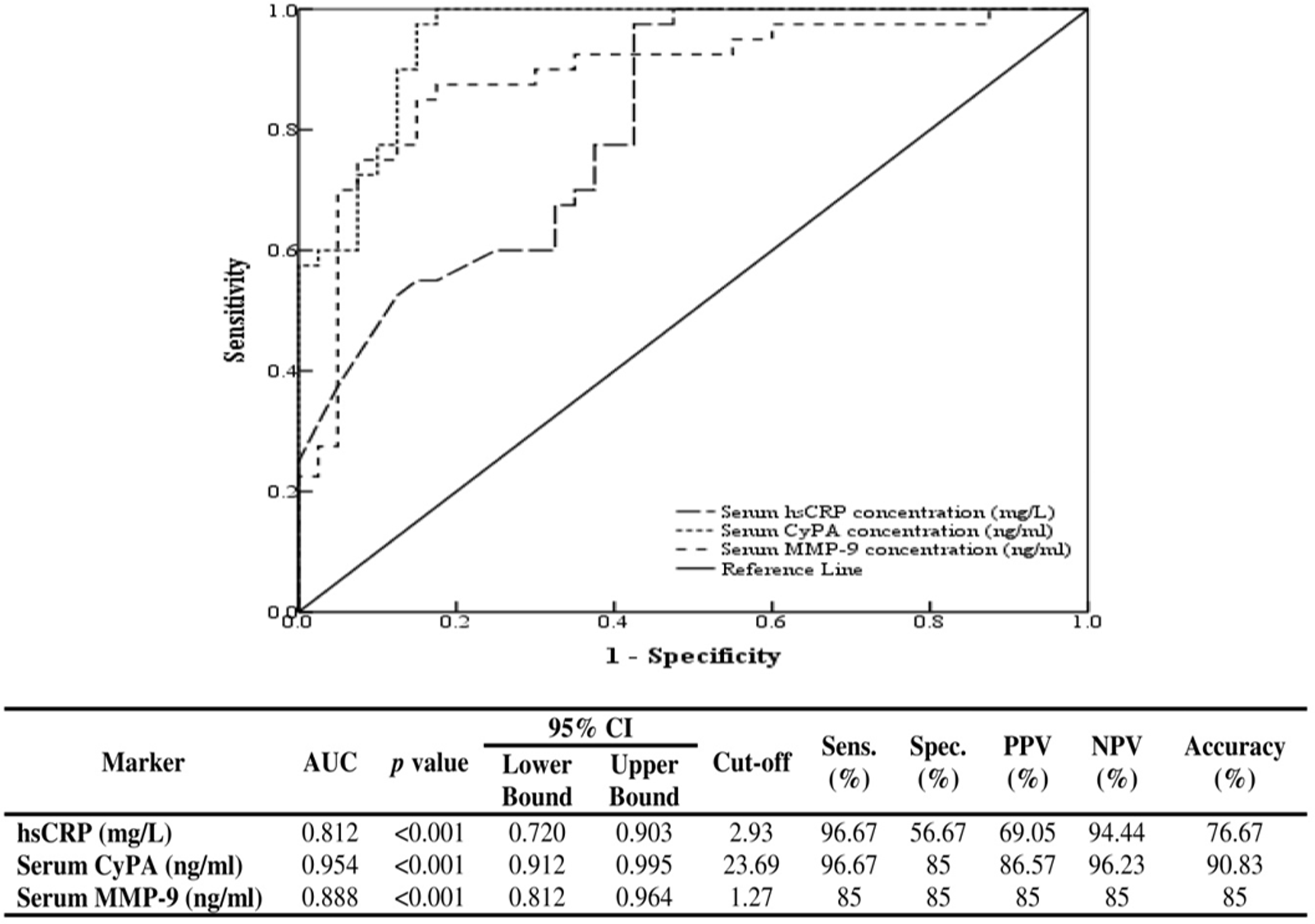
Receiver operating characteristic (ROC) curves of high sensitive C-reactive protein (hsCRP), cyclophilin A (CyPA) as well as matrix metalloproteinase-9 (MMP-9) for discriminating coronary artery disease patients with and without diabetes mellitus from healthy controls and type 2 diabetic patients.
Discussion
The interactions among endothelial cells (ECs), vascular smooth muscle cells (VSMCs), and adventitial inflammatory cells play an important role in regulating vascular function. CyPA is secreted from ECs and VSMCs in response to ROS, where it initiates the expression of adhesion molecules in ECs and serves as a chemo-attractant for inflammatory cells.23–26 Additionally, MMPs are secreted by several cell types of the vessel wall, including macrophages, ECs, and VSMCs.27,28 Accordingly, this study aimed to assess the relationship between serum levels of CyPA and MMP-9 in stable CAD patients with and without T2DM, in addition, to identify their association with the risk/cause of the disease, and finally to test their potential diagnostic value.
Results of circulating CyPA level in stable CAD patients is inconclusive; in the present work, CAD patients, irrespective of whether they had T2DM, showed a considerably elevated serum CyPA level compared to subjects without CAD in concordance with the results of Ramachandran et al. who found that CAD patients did not differ from patients with CAD and DM, but they were distinctly different, with higher levels of CyPA, from normal controls as well as DM patients. 11 In contrast, a study by Yan et al. revealed a non-significant difference in the circulating level of CyPA between patients with SA and control group. 29
The significant elevation of the circulating CyPA levels observed in sera of stable CAD patients with and without T2DM could be attributed to the production of vascular intracellular ROS which has been widely recognized to be implicated in the pathogenesis of CVD. 30 This production is stimulated by mechanical stretch, pressure, shear stress, hypoxia, and growth factors, all of which activate the RhoA/Rho-kinase system 31 leading to CyPA secretion by vascular cell components as a ROS-responsive protein.7,32
Regarding MMP-9 levels, there are conflicting data about its circulating level in stable CAD patients; Zeng et al. 33 and Hamed and Fattah 34 reported a significantly elevated level of circulating MMP-9 in patients with SA compared to controls. This appears to be in agreement with the results of the current study, which demonstrated a significantly higher serum MMP-9 level in stable CAD patients with or without T2DM compared to controls and T2DM patients. On the other hand, Yan et al. 29 and Jönsson et al. 35 demonstrated that the levels of MMP-9 in sera did not differ between patients with SA and controls.
In this study, the increased level of serum MMP-9 showed only a positive relationship with serum CyPA in the final model of the regression analysis; the relationship was persisted after adjusting for age, sex, smoking, BMI, systolic blood pressure, diastolic blood pressure, TC, TG, LDL-C, hypoglycemic drugs, and anti-hypertensive drugs as confounding factors. CD147 is thought to be the main cell surface receptor mediating CyPA signal transduction, and there is accumulating evidence suggesting that extracellular cyclophilins, probably via the interaction with CD147, may contribute to MMPs production. 36 Secreted CyPA mediates the production of ROS through the extracellular signal-regulated kinase (ERK1/2), AKT, and Janus kinase (JAK) signaling pathways via positive feedback.5,37 Further, studies showed that a high concentration of CyPA induced the expression of adhesion molecules via signaling pathways involving ERK1/2 and nuclear factor kappa B (NF-κB).37,38 The expression of MMP-9 from macrophages requires the activation of ERK1/2, which initiates inhibitor of kappa B (Iκ-B)/NF-κB. 39 Therefore, we can speculate that the cascade CD147-ERK1/2-NF-κB may be the main signaling pathway for CyPA-induced MMP-9 up-regulation resulting in the elevation of MMP-9 level in the sera of stable CAD patients with and without T2DM.
This seems to be consistent with the results of several previous studies; in multiple myeloma cells, CyPA over-expression increased the MMP-9 expression in a concentration- and time-dependent manner. 40 In the same context, MMP-9 was found to be regulated by CyPA using oligo-microarray, and the results were confirmed by RNA interference assay in hepatocellular carcinoma cells. 41 Qian et al. 42 found the same results in non-small cell lung cancer. Further, the presence of a cyclophilin inhibitor, NIM811, hindered the up-regulation of MMP-9 during foam cell differentiation process, while the presence of CyPA enhanced the secretion of MMP-9 by mature foam cells. 21 Moreover, CyPA increased the in vitro production and activation of MMP-9 in monocytes/macrophages derived from rheumatoid arthritis synovial fluid. 43
Stable CAD is a syndrome of recurrent, transient episodes of chest pain reflecting a supply–demand mismatch in myocardial perfusion. 44 Many lipid-laden monocytes/macrophages, also known as foam cells, characterize the early atherosclerotic lesion. After settling under the endothelium, quantities of monocytes differentiate into macrophages that endocytose lipid and accumulate under the vascular endothelium to form fatty streaks. As they become larger, foam cells place pressure on the intimal layer, which encroaches on the lumen of the vessel and impedes flow. 45 CyPA contributes to the formation of foam cells and the up-regulation of NF-κB-related proteins such as MMPs. These proteins are released from foam cells and are among the main causes of acute cardiovascular events. 46 Additionally, CyPA stimulates migration and proliferation of VSMCs, expression of adhesion molecules in ECs, and chemotaxis of inflammatory cells. 37 Studies on cyclophilin knockout mice models have clearly indicated its role in vascular disease progression. Mice lacking both apolipoprotein E (ApoE−/−) and CyPA (CyPA−/−) appeared to be protected from atherosclerosis development due to the decreased levels of inflammation mediated by the absence of CyPA. 47 In the same context, MMPs play a part in VSMCs migration and neointima formation after localized vascular injury,48,49 and studies using knockout mice have suggested that MMP-9, among other MMPs, is implicated in plaque development and burden. After temporary carotid artery ligation, MMP-9 deficiency led to significantly diminished intimal hyperplasia in ApoE−/− mice. 50 This is supported by the results of the current work which showed that high circulating levels of CyPA and MMP-9 in this study population were associated with an increased risk of developing stable CAD after adjusting for age, sex, smoking, BMI, systolic blood pressure, diastolic blood pressure, TC, TG, and LDL-C as potential confounders.
Further, the diagnostic values of hsCRP, CyPA, and MMP-9 to discriminate between stable CAD patients with and without T2DM and subjects without CAD were examined. The results showed that CyPA and MMP-9 have superior diagnostic efficacy over hsCRP, and to the best of our knowledge, this is the first study that reports such hypothesis. However, previous studies reported the diagnostic value of CyPA as a diagnostic marker in inflammatory cardiomyopathy and MMP-9 in acute coronary syndrome.51,52
In conclusion, this work sheds the light on the relationship between the circulating levels of CyPA and MMP-9, indicating that serum CyPA might be a determinant factor of MMP-9 level and the increase in the level of the latter appears to be associated with the high level of the former in sera of stable CAD patients with and without T2DM. Moreover, our results pointed out that high levels of CyPA and MMP-9 are associated with higher susceptibility to stable CAD. Thus, lowering the levels of both CyPA and MMP-9 may provide novel approaches for the treatment of stable CAD; further studies are required to verify this hypothesis. Finally, CyPA and MMP-9 appear to be good candidates as biomarkers in clinical practice to diagnose stable CAD patients with and without T2DM.
Study limitation
Several limitations should be acknowledged in this study. First, the control subjects and T2DM patients were not angiographically examined, and thus the possibility of subclinical atherosclerosis cannot be excluded. Further, we could not provide follow-up or prognostic data concerning this patient collective due to the design of the study. Our study primarily intended to evaluate whether there is a relation between the levels of CyPA and MMP-9 in sera of stable CAD patients. Moreover, this was an observational cross-sectional study which makes it possible to show the associations but not the causal relationships between parameters. Finally, because this was a single-center study, there are likely selection bias and limitation of the generalizability of the findings, and for that, multicenter studies with larger sample size are needed to confirm the results of the present work.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.