
Abstract
Objective
The covered endovascular reconstruction of the aortic bifurcation (CERAB) technique was introduced in 2009 in order to provide an anatomically and physiologically optimal endovascular reconstruction of the aortic bifurcation.
Method
In the current review, all available evidence on this technique was summarized.
Results
In vitro studies have shown a more favorable geometry of CERAB compared to kissing stents, leading to better local flow conditions. The results of CERAB are at least as good as those achieved with kissing stents in a more complex group of treated patients. The mid-term patency rates approach those of surgical reconstruction. Initial data show that the technique can also be used in combination with chimney grafts in order to preserve side branches.
Conclusion
CERAB has proven to be the most optimal endovascular treatment option for aorto-iliac occlusive disease with regard to geometry and flow and is related to promising clinical outcomes. Prospective and comparative trials are necessary to elucidate the most optimal treatment algorithm for patients with aorto-iliac occlusive disease.
Keywords
Introduction
The aortic bifurcation is a predominant location of atherosclerosis and stenosis in this area could lead to the entire spectrum of symptoms of peripheral arterial occlusive disease. Historically, surgery, by means of an aorto-bi-femoral graft or endarterectomy, has been the preferred treatment option when an intervention was indicated. Surgery is related to good long-term outcomes with patency rates up to 90%.1,2 However, it has also been associated with an early mortality rate of about 4%. In addition, early complications arise in 5–10% of cases and about 10% will eventually develop an incisional hernia. 3 These morbidity and mortality rates highlight the desire for less invasive strategies, aiming to provide a similar long-term patency rate. In recent years, there has been a dramatic shift towards an endovascular first strategy for most stenotic and occlusive lesions in the iliac artery. In a review of literature, it was shown that in patients with severe lesions, technical success rate above 90% can be achieved with a primary patency at one year of 87% for TASC-C and 90% for TASC-D lesions, respectively. 4 Primary stenting was associated with a better primary patency rate in these lesions. In a randomized trial, comparing bare metal stents with covered stents, it was shown that the use of covered stents is related to an improved outcome with regard to patency and target lesion revascularization rates up to five-year follow-up. 5 The largest difference was observed in TASC-C and TASC-D lesions, supporting the use of these devices in complex lesions.
When the aortic bifurcation is involved in the pathology, other strategies are indicated, and the most frequently used technique is the kissing stent configuration. In an individual-participant meta-analysis on 605 patients, it was recently shown that this technique is related to a high technical success rate and five-year assisted-primary and secondary patency rates of, respectively, 73% and 89%. 6 These results could be considered as acceptable but are still inferior to those achieved with surgery, emphasizing the need for improved techniques. The covered endovascular reconstruction of the aortic bifurcation (CERAB) technique was designed to achieve a more optimal anatomical and physiological reconstruction in order to improve the results of endovascular treatment of the aortic bifurcation. 7 In the current paper, the current view on technique itself is described and the available evidence, from its first-in-human in February 2009 until September 2019, is summarized.
Method
A systematic review was conducted on the results obtained using the CERAB technique. The interface used for searching the Pubmed database. Medical Subject Headings (MeSH) terms included “CERAB”, “Covered Endovascular Reconstruction of the Aortic bifurcation”, “Aortoiliac occlusive diseases”, or “AIOD” combined with “Covered stents”. Cross-referencing was performed. Articles were included from the start of the databases until August 2019, excluding review articles. The search identified 15 papers on CERAB of which two reviews were excluded. In total, 152 unique patients were described of which five were treated with self-expanding stents instead of balloon-expandable covered stents. In addition, 96 patients were reported that were treated with an EndoVascular Aneurysm Repair (EVAR) device for this indication. There were four in vitro studies and two technical papers.
Technical background
There is considerable evidence that the local geometry of kissing stents is a driving factor for re-stenosis and occlusion. Radial mismatch, defined as the still perfused dead lumen space around the stents, is thought to be one of the reasons for flow disturbances and the consequent failure. 8 This is further emphasized by a recent study which showed that a protrusion of kissing stents more than 20 mm into the distal aorta is a significant determinant factor for the occurrence of in-stent restenosis. 9 The position of the stents may also be of influence as stents in a crossing position were described to have an inferior outcome to those that are not crossing. 10 The hemodynamic changes, due to the geometrical mismatches, may lead to the presence of immature mesenchymal tissue, intimal hyperplasia, and organizing thrombus not only in the space created inferior to the vertex of the opposing stents but also within the stents and the free floating portions of the stents. 11
Consequently, a reduction of mismatch, consequently optimizing flow conditions, is the main objective of CERAB. 7 After access is acquired to both common femoral arteries, using two short 6 Fr introducer sheaths, heparin is administered. Subsequently, the lesion is crossed, using regular techniques from both sites. In some cases, a brachial access may be indicated to achieve this. After recanalization, stiff wires are positioned and two long introducer sheaths are inserted with a diameter of 6 or 7 Fr (depending on the brand of covered stent used) and 9 Fr, respectively, an angiography is made (Figure 1(a)). A 12 mm balloon-expandable covered stent with the appropriate length is then introduced through the 9 Fr sheath. After identifying the proper location, the stent is expanded in the distal aorta approximately 15 mm above the bifurcation (Figure 1(b)). The already expanded covered stent is then cannulated from the contralateral site. After confirming the position in the covered aortic stent, a stiff wire is placed and a larger balloon, typically 16 mm in diameter, is inserted. The covered aortic stent is then proximally adapted to the aortic diameter, by positioning the distal balloon marker about 15 to 20 mm proximal to the distal stent margin (Figure 1(c)). The distal stent part has then become funnel-shaped. It is important to emphasize that the distal portion should remain 12 mm in diameter in order to minimize mismatch after inserting the iliac limbs. This is also the reason why the use of larger stents is not advocated for this technique. Then, the covered aortic stent is cannulated from the contralateral side and a stiff wire is introduced. Caution should be taken in every phase where the covered aortic stent is passed as catheters and balloons could induce a proximal migration of the covered aortic stent, particularly in those patients with a patent aorta. When this may happen, repositioning of the covered aortic stent using a 16-mm balloon is often feasible. Two iliac covered stents, typically 8 mm, are then placed in the 12 mm segment of the covered aortic stent and simultaneously inflated (Figure 1(d)). Both covered stents are now making a very tight combination with the covered aortic stent as were they molded together, simulating a new bifurcation with the hemodynamic aspect of a flow splitter (Figure 1(e)). If indicated, the stents can be extended distally with additional balloon-expandable or self-expanding covered stents. Control angiography is performed angiography to assess patency and the outflow (Figure 1(f)). In some cases, contrast may be seen outside the stents through the mismatch area (or gutters). In contrast to EVAR, this is not harmful, but even potentially beneficial as they may provide flow to lumbar arteries or the inferior mesenteric artery.
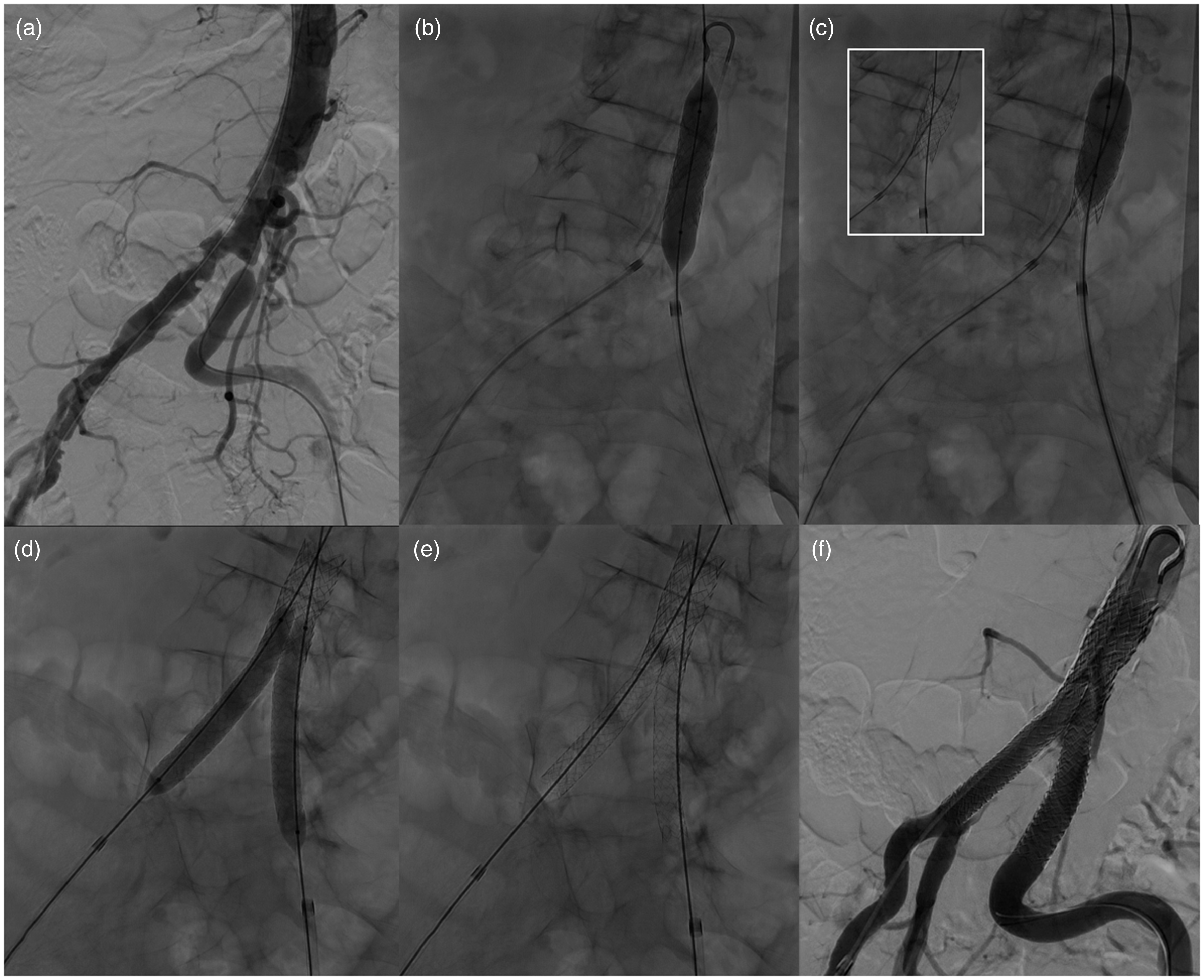
Procedural images of an 84-year-old female patient with right-sided Rutherford 5, based on emboli originating from a lesion in the aortic bifurcation. (a) Angiography showing a bilateral stenosis of the common iliac artery extending into the distal aorta. (b) Deployment of a 12 × 39 mm BeGraft Aortic balloon-expandable stent (Bentley InnoMed GmbH, Hechingen, Germany). (c) Flaring of the aortic stent with a 16 mm angioplasty balloon (Cristal Balloon, Balt Extrusion, Montmorency, France). (d) Deployment of two 8 × 57 mm BeGraft Peripheral balloon-expandable stents. (e) Final geometry of the CERAB reconstruction. (f) Completion angiography showing a patent reconstruction with a good outflow.
The technique can be combined well with other techniques. As appropriate outflow is important to achieve optimal results, an endarterectomy of the common femoral artery can be performed to assure outflow to at least either the deep of the superficial femoral artery. When planning a CERAB case, a computed tomography of the entire aorta is pivotal for several reasons. When a brachial access appears to be indicated, information on this access and thoracic aorta is imminent. Moreover, it is important to be informed on the quality of the visceral vessels. In case of a diseased superior mesenteric artery and/or celiac trunk with a patent inferior mesenteric artery, a chimney configuration of the latter should be considered to decrease the risk on bowel ischemia. In cases where the occlusive disease is close the renal arteries, various strategies could be followed. A period of 12–24 h of thrombolysis could reduce the thrombus load in the infrarenal aorta but may not always be successful. Protection balloons in the renal arteries are indicated in cases where the disease is close to the renal arteries. As the balloon of the covered aortic stent is longer than the stent itself, the shoulder could otherwise dislodge thrombus in the renal arteries. Additional chimneys in the renal arteries are also feasible, but evidence on the outcome is limited.
At the time of introduction of CERAB in 2009, the Atrium Advanta V12 LD balloon-expandable covered stent (Getinge AB, Wayne, NY, USA) was used as the aortic stent for this indication.7,12 Unfortunately, this stent has not been available during the last years, but others became available. Anecdotally, it is know that all of them have been used with technical success for CERAB. Most of these stents are made of stainless steel (Atrium Advanta V12 LD, Gore Viabahn® VBX (W.L. Gore and Associates, Flagstaff, AZ, USA) and the LifeStream (Bard Peripheral Vascular, Tempe, AZ, USA)), whereas others are made of cobalt chromium (BeGraft Aortic (Bentley InnoMed GmbH, Hechingen, Germany)) or platinum–iridium Cheatham Platinum (CCP) stent (NuMED Inc., Hopkinton, NY, USA). It is important to emphasize that the design of these stents differs significantly. Also the way the covering material is applied differs from Polytetrafluoroethylene (PTFE) on both sides of the stent (Atrium Advanta V12 LD (Gettinge AB), Gore Viabahn VBX (W.L. Gore and Associates) and the LifeStream (Bard Periferal Vascular)) by an external layer only (BeGraft Aortic (Bentley InnoMed GmbH), CCP stent (Numed Inc.)). Overexpansion is described in the instructions for use of most of them but evidence on the impact of flaring of a part of the stent on long-term stent integrity is lacking (Table 1). The impact of flaring on the PFFE integrity of aortic stents has also not been studied so far. However, for covered stents that are used for side branches of fenestrated endografting, the flaring does not seem to affect the integrity of the stent struts or the PTFE. 13
Available 12 mm balloon-expandable covered stents that can be used for CERAB.
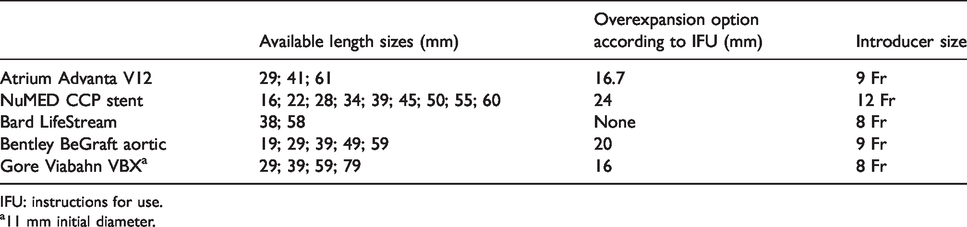
IFU: instructions for use.
11 mm initial diameter.
Proof of concept
The geometry of CERAB has been studied in both an in vitro and a clinical study. In the in vitro study, the CERAB configuration was compared to kissing self-expanding bare stents and to kissing balloon-expandable covered stents. 14 This study showed that the mismatch areas as well as their volumes were much lower in CERAB when compared to both kissing stent configurations, even though the stent conformation of self-expanding stents is higher supporting the hypothesis that the CERAB configuration is the most anatomical option. In addition, this study demonstrated that deployment of the limbs above the 12 mm portion of the covered aortic stent increases the mismatch area, confirming that no bigger stent should be used for this technique and that attention should be paid to the tapering of the covered aortic stent and the positioning of the limbs in order to get the most optimal result. The difference in mismatch area between CERAB and kissing stents was later confirmed in a clinical study comparing CT scans of matched patients treated with either technique. 15
The impact of the difference in mismatch area was studied in an in vitro model using laser particle image velocimetry in a phantom with a physiological flow with blood-mimicking fluid. 16 It was observed that beneficial flow patterns were present at the inflow section of both CERAB and self-expanding bare kissing stents, with normal wall shear stress values kissing covered stents, however, had a zone of recirculation and stasis of blood at the entrance resulting in low average wall shear stress value and high oscillatory shear index. The self-expanding bare kissing stents had an area of persistent low flow throughout the cardiac cycle in the area between the anatomic bifurcation and neo-bifurcation. This is the area where mesenchymal tissue, intimal hyperplasia, and organizing thrombus has been observed. 11 The beneficial geometrical outcomes for CERAB and the resulting optimized flow patterns confirmed the concept of CERAB.
CERAB, however, may have other implications for flow and wall shear stress. In another experimental study, it was observed that a hemodynamic significant outflow stenosis is related to a two-fold decrease in peak outflow velocity and a three-fold decrease in time-averaged wall shear stress in both CERAB and control models. 17 In CERAB, however, the time-averaged wall shear stress was two-fold lower compared to the control model, independent of the lesion severity. As a low wall shear stress is related to progression of atherosclerosis, this indicates that outflow stenosis after CERAB may have a higher tendency to progress in time and warrant surveillance and potentially early treatment.
Clinical evidence
The clinical evidence on CERAB is still limited so far to case series. In 2018, Taeymans et al. described the mid-term outcome in a series of 130 consecutively electively treated CERAB patients, including the first in human. 18 This was an update from the earlier published one-year data on a smaller cohort. 12 Chimney procedures were excluded from this analysis. The mean age in this cohort was 61 and 53% were male. A previous intervention in aorto-iliac area was performed in 41% of patients, including open surgery in 7 and an endovascular treatment in 46 patients. Intermittent claudication, not responding to conservative treatment, was the indication in 66% and the remaining were treated for critical limb ischemia. The lesion was classified as TASC-D in 89% of patients. After CERAB, the ankle–brachial index significantly increased from 0.65 ± 0.22 to 0.88 ± 0.15. The 30-major complication rate was 8% and there was no 30-day mortality. These complications consisted of a stent collapse in one of the limbs in three patients of which two were salvaged endovascular. There was one re-operation needed for a failing closure device, two early occlusions of the CERAB were successfully treated by thrombectomy (n = 1) or thrombolysis (n = 1), and one patient had a deterioration of renal function without dialysis requirement. The early stent collapses are of particular interest. The reason for these early collapses is not elucidated to date, but could indicate that the stent design is still not optimal to overcome the often heavily calcified lesions. Unfortunately, in these patients a completion angiography was made only in the anterior–posterior plane. A suboptimal deployment during the procedure may therefore also have caused these complications, rather than a recoil after the procedure. Proper completion imaging therefore would require an angiography in two directions or a cone beam computed tomography. The median hospital stay was two days. At one year and three years of follow-up, 94% and 96% of the patients clinically improved at least one Rutherford category. Limb salvage rate was 98% at one year and 97% at three years of follow-up. Primary, primary assisted, and secondary patency rates were 86%, 91%, and 97% at one year; 84%, 89%, and 97% at two years; and 82%, 87%, and 97% at three years, respectively. Freedom from clinically driven target lesion revascularization was 87% at one-year follow-up and 86% at both two-year and three-year follow-up. When we compare these data with the previously mentioned individual-participant meta-analysis on the treatment of kissing stents, it seems that the CERAB group included more complex patients with more critical limb ischemia, more TASC-C and TASC-D lesions and more previously performed reinterventions (Table 2).6,18 Yet at 24-months, the primary and secondary patency rates were better in the CERAB cohort, suggesting that indeed with CERAB better results could be achieved. A prospective comparative trial on this subject, however, is warranted.
Outcomes of endovascular treatment of aorto-iliac occlusive disease using CERAB, kissing stents, and the AFX Unibody (Endologix, Irvine, CA, USA).

NR: not reported.
As an alternative for balloon-expandable stents, the use of self-expanding stents in a y-configuration has been suggested, with the aortic stent placed though the brachial artery over two 0.014″ guidewires, one to each femoral artery.19,20 This technique avoids the cannulation of the aortic stent that could be challenging during CERAB.
As an alternative for CERAB, devices have been used that are designed for aneurysms of the abdominal aorta. In 2005, a series of five patients with TASC-C or TASC-D iliac occlusions was described that were successfully treated with the Gore Excluder Endoprosthesis (W.L. Gore and Associates). 21 More recently, Maldonado et al. reported a series of 91 patients treated with the AFX Unibody Endograft (Endologix, Irvine, CA, USA). 22 The groups were comparable with the CERAB series with regard to clinical state and TASC classification. The patency results of both techniques are close (Table 2).18,22 Nevertheless, the larger profile and the mode of positioning of the AFX Unibody (the device should be pulled onto an occluded or stenosed bifurcation) could render the choice for this option less favorable compared to CERAB. On the other hand, when the infrarenal aorta is dilated to a diameter larger than that can be achieved with the balloon-expandable covered stents, this may be a good alternative, as well as in countries where the large diameter covered stents are not available.
The technique of CERAB is applicable after previous interventions in this area, including the placement of kissing stents or a surgical bypass.12,18,23 Recently, the technique was described to recanalize an occluded EVAR device. 24 In the series of Taeymans et al., the CERAB procedures that were performed after earlier interventions tended to have a lower primary patency. 18
In another case series, the combination of CERAB with chimneys was described (Figure 2). 25 A total of 15 chimney grafts were used in 14 patients. Eleven were male with a mean age of 61.2 years. Chimneys were placed in the inferior mesenteric artery (n = 8) and renal arteries (n = 7). The technical success rate was 100% and after a median follow-up of 12 months (range 6–24), the patency of the CERAB was 100% and of the chimney graft was 93%.
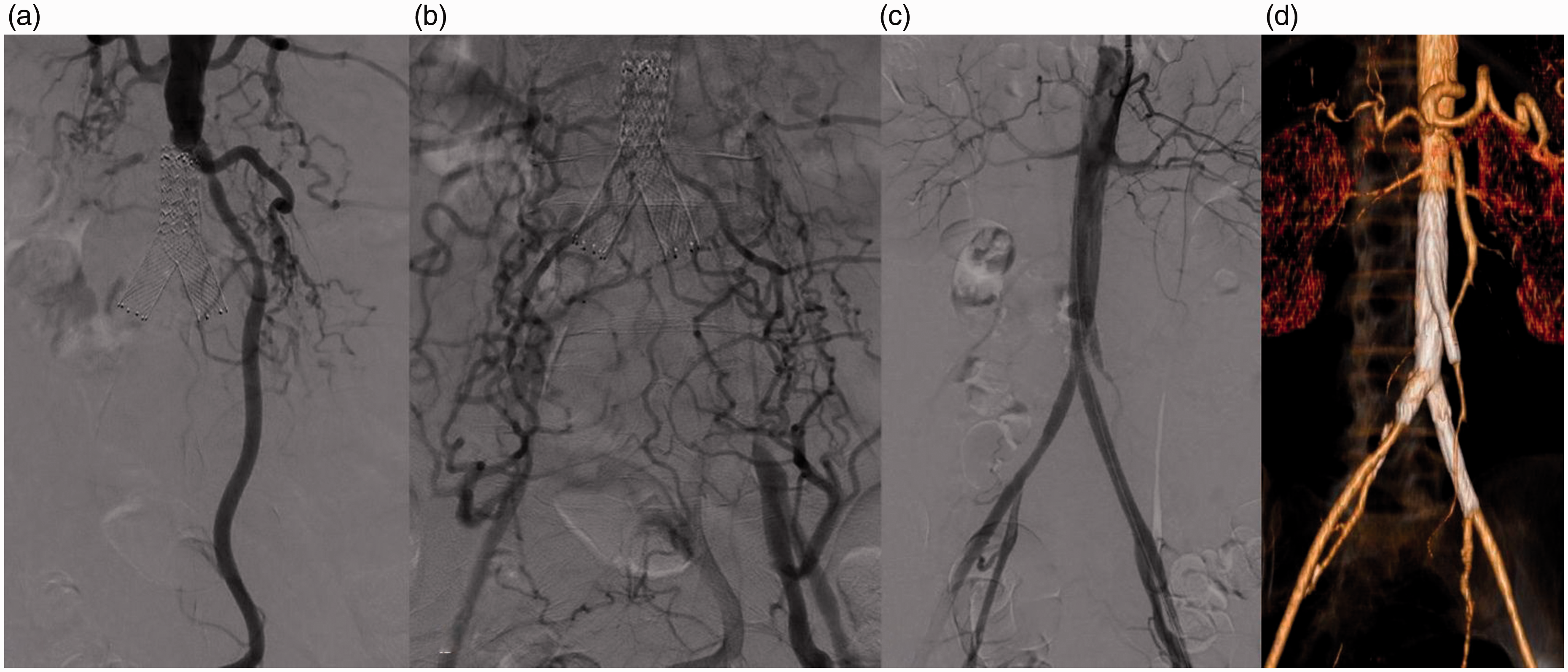
Procedural images of a 52-year-old female patient suffering from bilateral Rutherford 4. She was previously treated with bare metal kissing stents that got occluded. (a,b) Procedural angiography showing a bilateral occlusion of the common iliac artery, including the kissing stents, extending into the distal aorta up to the lower level of the patent inferior mesenteric artery. (c) Completion angiography after the CERAB reconstruction (12 mm × 41 mm Atrium Advanta V12 LD balloon-expandable covered stent as aortic body combined with 8 mm Atrium Advanta V12 balloon-expandable covered stents as iliac limbs (Getinge AB, Wayne, NY, USA)), including a chimney graft in the inferior mesenteric artery (6 mm × 59 mm Atrium Advanta V12 balloon-expandable covered stent), showing a patent reconstruction with good outflow in both iliac arteries and the inferior mesenteric artery. (d) Three-dimensional reconstruction of the chimney-CERAB reconstruction.
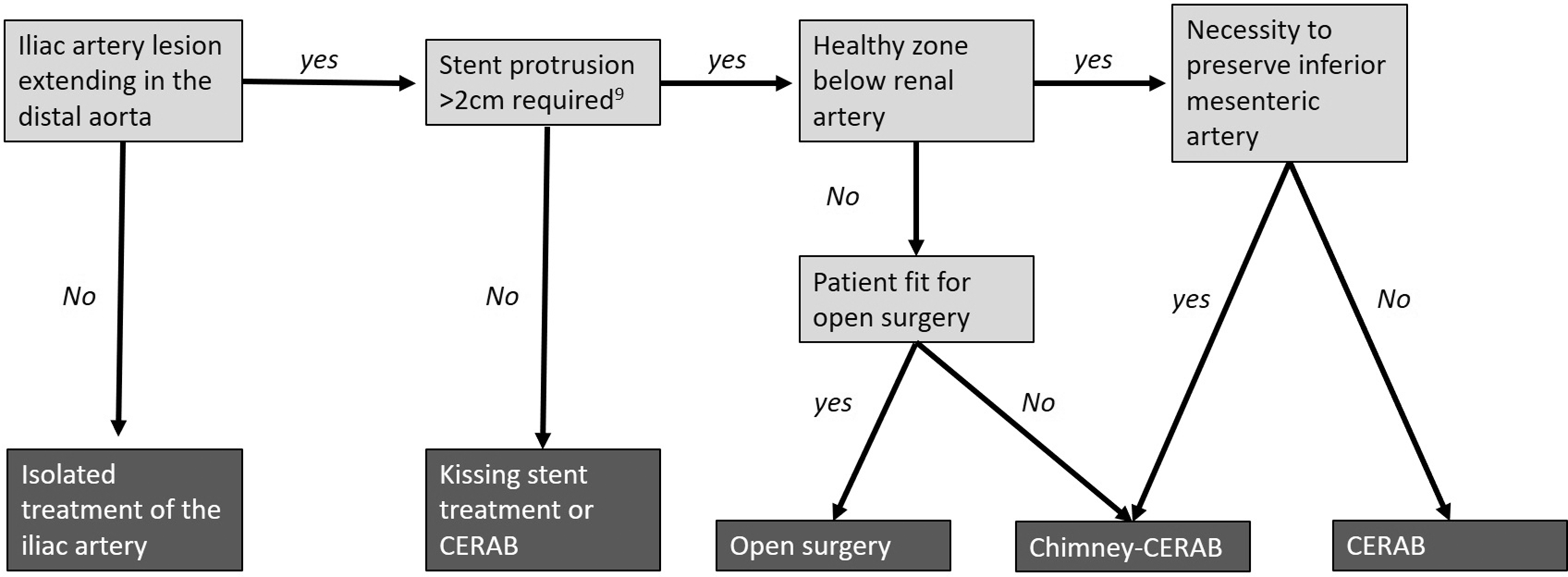
Example of a treatment algorithm of patients with aorto-iliac occlusive disease requiring an intervention.
Discussion
In the current paper, the available evidence on the CERAB reconstruction was summarized. In vitro data have shown that, when compared to the kissing stent configuration, the geometry of CERAB is superior.14,15 This, in turn, leads to more favorable flow conditions that could positively affect the outcome. 16 When comparing the three-year clinical outcome with surgical outcome, it is evident that the patency is approaching those that have been described for open surgery.1,2,18 When comparing them with the endovascular alternative, the kissing stents and the results at two-year are at least equal, with a clear trend to be better, in a more complex group of patients.6,18 It should be taken into account that the CERAB series is likely biased by a learning curve, as the first patients ever treated with this technique were included in this series. Obviously, comparative trials would be needed to come to a final conclusion on the most optimal treatment algorithm for aorto-iliac occlusive disease. Very likely there will be a place for all three techniques but selecting the right technique for the right patient is still difficult. Kissing stents could be used effectively as long as they do not protrude too far in the distal aorta. 9 The threshold when CERAB will start to outperform kissing stents is yet unknown. Surgical treatment may also remain to have a role in this area. The CERAB technique can be used in disease up to, or even above, the renal arteries with the use of protection balloons or chimneys. 25 Nevertheless, in a young and fit patient, the surgical option may be better, as the long-term outcome of chimneys is unknown.
A potential disadvantage of the use of covered stents is the overstenting of collateral arteries, as this might deteriorate the clinical state in cases of occlusion. So far this has not been studied in the aorto-iliac artery, but a previous study in the femoral artery showed not such an effect. 26 The inferior mesenteric artery is regularly overstented in EVAR cases and as such it seems reasonable to assume that this is the same in case of occlusive disease. The state of the superior mesenteric artery and celiac trunk, however, should always be assessed. Often it is feasible to preserve a patent inferior mesenteric artery by placing the covered aortic stent below it. Another disadvantage is the requirement of a larger sheath that is needed for the aortic cuff.
A limitation to the data so far is that they consist of retrospective series of a small group of experienced hospitals. It is unclear how these data would reflect in common clinical practice. Prospective studies on the CERAB technique are clearly indicated. As there are design differences between the various balloon-expandable covered stents each device should demonstrate its own efficacy. So far, only data on CERAB using the Atrium Advanta V12 balloon-expandable covered stent ((Gettinge AB) are available.
Being a new technique, CERAB is still in development. During the last years, the proximal anatomical border has been challenged with chimneys in the renal artery, whereas distally is has been used all the way to the common femoral artery in combination with an endarterectomy. Based on the information from aneurysm studies, the preservation of the hypogastric artery appears to be important to prevent ischemic complications. In cases with a patent hypogastric artery and a fully diseased common iliac artery, different strategies could be chosen. The orifice could be overstented with a covered stent, but this may induce buttock claudication. The use of a bare stent in this part, preserving flow to the hypogastric artery, is an alternative, but vulnerable for restenosis. As a third option, a CERAB like reconstruction could be made in the iliac bifurcation as well. To date, no literature is published on this subject but anecdotal information on the feasibility is available.
Given the minimally invasive character of CERAB and the requirement of an intensive care unit after open surgery, it is likely that CERAB will be cost effective. When comparing with kissing stents, the opposite is likely true due to the addition of the aortic stent. The development of a proper evidence-based treatment algorithm on aorto-iliac occlusive disease, also taking into account the cost effectiveness, is a challenge for the future. An example of a possible treatment algorithm is provided in Figure 3. Another challenge is the selection of an appropriate medical strategy after treatment. Statins and anti-platelets are indicated and very likely a period of double platelet inhibitors is better. Evidence is emerging that patients may respond different to different platelet inhibitors and not all patients respond well to every drug. A double anti-platelet regime for at least three months is advocated, but not supported by evidence in this area.
In conclusion, CERAB is a more anatomical and physiological method to reconstruct the aortic bifurcation compared to kissing stents. The concept is supported by experimental studies, and the first clinical data are promising and seem to outperform the kissing stent configuration. Prospective comparative trials with both surgery and the kissing stent configuration are necessary to elucidate the most optimal treatment algorithm for patients with aorto-iliac occlusive disease.
Supplemental Material
VAS896197 Supplemental Material - Supplemental material for Update on covered endovascular reconstruction of the aortic bifurcation
Supplemental material, VAS896197 Supplemental Material for Update on covered endovascular reconstruction of the aortic bifurcation by Michel MPJ Reijnen in Vascular
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.