
Abstract
Objectives
Scarring from prior bypass surgery and irradiation may compromise revascularization options in critical ischemia due to underlying occlusive disease. Occlusive disease of the axillo-brachial artery is particularly difficult to revascularize under such hostile conditions.
Method
We present a case of a 58-year-old woman presenting with a painful, pulseless, and cool left upper extremity. The patient had a known history of left upper extremity occlusive disease which was managed by subclavian–axillary artery stenting with re-occlusion and subsequent extra-anatomic left carotid-to-proximal brachial artery prosthetic bypass, which was complicated by stroke. The patient had a history of left mastectomy, axillary node dissection, and external beam radiation therapy. When considering revascularization options, the combination of post-radiation changes and scarring of the conventional operative zones for revascularization posed a high risk for complications. We describe a novel approach for such revascularization, where the inflow source was the terminal brachiocephalic artery, outflow to the upper left brachial artery, with anatomic intrathoracic-to-axillary tunneling through the thoracic outlet after verifying the lack of dynamic extrinsic compression at that level.
Result
The procedure resulted in resolution of the symptoms and the patient continued to do well 2 years later.
Conclusion
This case shows that anatomic tunneling through the thoracic outlet can be a viable option for upper extremity revascularization when hostile conditions preclude other anatomic tunneling routes or extra-anatomic options.
Keywords
Introduction
A hostile operative field can be problematic during redo vascular reconstructions. Scaring from prior surgery particularly those involving prior vascular exposure can result in dense scarring rendering re-exposure difficult. External beam radiation therapy causes an obliterative intravascular response in addition to fibrotic perivascular tissue changes, resulting in fibrotic and noncompliant tissue planes.1,2 This poses a high risk of surgical wound complications including wound breakdown, lymphatic leaks, poor healing, and infections are well described and the risk is particularly higher with prosthetic conduits. The use of non-autogenous conduit further increases the risk of infection and other wound-related complications. Extra-anatomic bypass, where feasible, is usually the preferred option due to a lower risk of vascular injury and infection.1,3–11 Radiation-induced vasculopathy involving the subclavian, axillary, and brachial arteries following multi-modality treatment of breast cancer has been described.2,4,7,9 Radiation is also a known risk factor for progressive atherosclerotic occlusive vascular disease. 12
Case report
A retrospective review of this clinical case was approved by our local IRB. A 58-year-old woman presented to a local hospital with a painful, pulseless, and cool left upper extremity. The patient had a prior history of subclavian–axillary artery stenting for occlusive disease elsewhere 13 months prior to the current presentation. Shortly after, the stents became occluded, and she underwent left carotid-to-proximal brachial extra-anatomic prosthetic bypass which was also reportedly complicated by an intraprocedural stroke. Her past medical history is significant for breast cancer treated with left mastectomy, axillary node dissection, and radiation therapy 4 years earlier. She also has a 40-year one pack per day smoking history. CT angiogram showed occlusion of the bypass with reconstitution of the proximal brachial artery (Figure 1). Flow in the vertebral artery was antegrade as the occlusion was distal to its origin. Examination showed a pale and cold hand with diminished sensation and motor function.
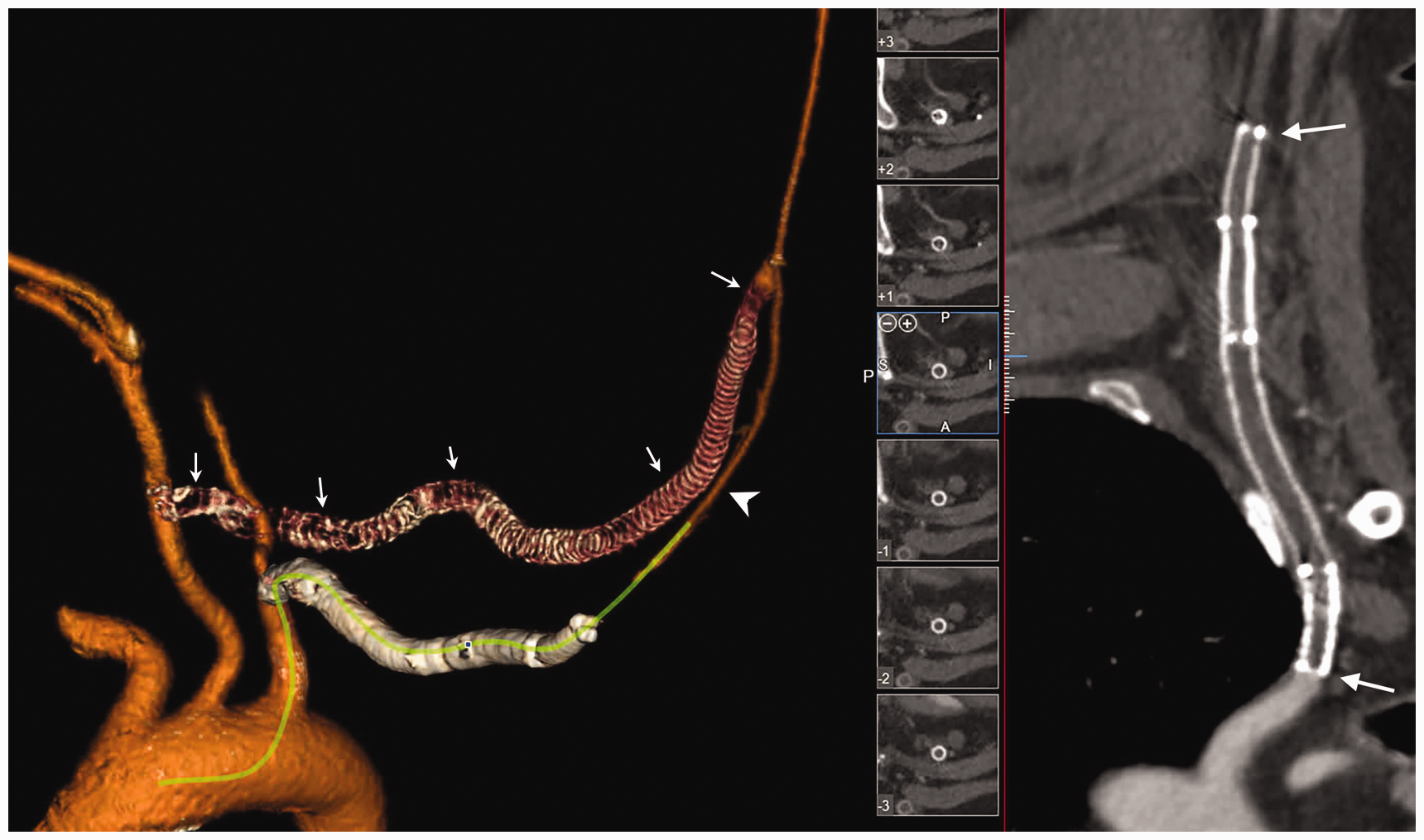
Preoperative imaging of the occluded stents (arrows), prosthetic graft, and reconstituted brachial artery (arrowhead).
Various options for revascularization were considered but we felt that the neck, supraclavicular area, and axilla would be hostile due to prior radiation therapy and surgical procedures. We thus opted to use an intrathoracic great vessel as inflow for the bypass, tunneling it anatomically to the upper arm through the thoracic outlet.
A partial upper median sternotomy and manubriotomy was performed. Through this, the innominate vein was identified and protected by reflecting it caudad. The pericardium was then divided, and the innominate artery and the proximal segments of its two branches were then mobilized and isolated. After examining the course and configuration of the exposed great vessels, we decided to base the proximal anastomosis of the bypass on the junction of the terminal innominate artery and proximal right subclavian artery, which we felt minimized the risk of kinking. A brachial incision was performed along the medial upper arm. The caudal end of the stent was identified by palpation, and a patent segment was selected to perform the distal anastomosis.
A tunnel was then developed using an aortic clamp from the upper arm tunnel with the assistance of a digit from the chest. The thoracic outlet was reached with the digit by palpating the anterior margin of the first rib and establishing proximity to the medial clavicle. The anterior scalene muscle was divided carefully from an intrathoracic approach with caution using scissors and real-time nerve-stimulator monitoring to avoid injury to the phrenic nerve. The developed tunnel was then inspected digitally during a variety of thoracic outlet stress positions, confirming ample caliber to accommodate the additional conduit without dynamic compression at the thoracic outlet. A non-reversed cryopreserved greater saphenous vein (CryoLife, Kennesaw, GA, USA) was selected for conduit due to the lack of autogenous conduit. Proximal anastomosis was constructed onto the terminal innominate artery straddling the proximal right subclavian artery which was isolated using a side-biting clamp. The vein was then pressurized and valvulectomized retrogradely. The aortic clamp passed through the thoracic outlet was used to retrieve the fully pressurized vein through the tunnel, with caution used to make sure that there were no kinks or twists in the conduit. The distal anastomosis was constructed in the usual manner. Reperfusion restored a robust pulse in the brachial artery and good triphasic signals and the ulnar and radial vessels. The sternotomy was closed, and a drain was left in the mediastinum.
The patient recovered well after the procedure. Her ischemic symptoms resolved with restoration of normal upper extremity perfusion on non-invasive imaging, and CT angiography with 3D reformatting demonstrated a smooth, non-compressed course of the bypass with ample room at the thoracic outlet (Figure 2). She was maintained on dual antiplatelets therapy. Follow-up, 2 years later, showed the patient continues to do well and CT angiography showed a widely patent bypass (Figure 3).
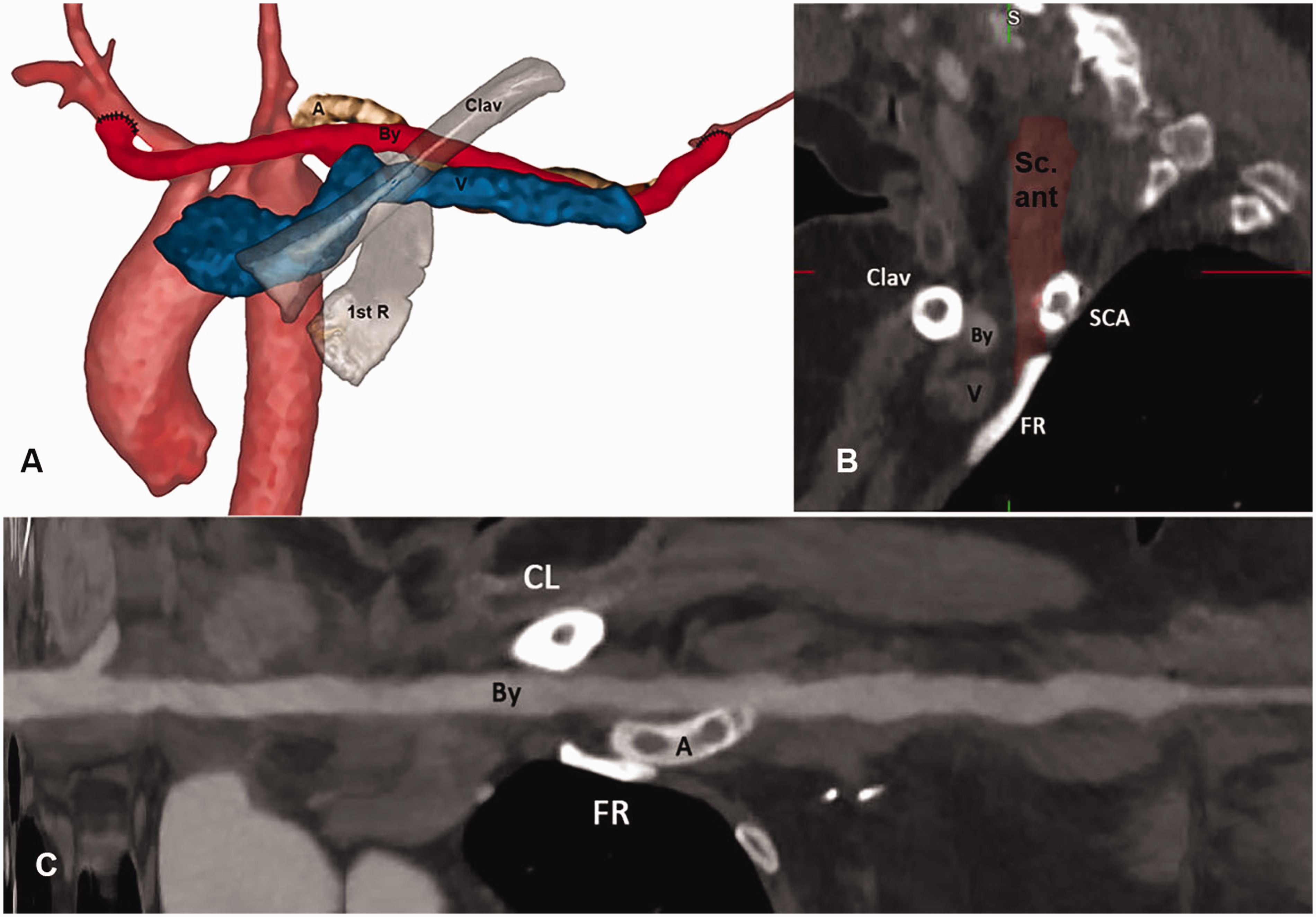
(a, b) Postoperative CTA with 3D reconstruction demonstrating the relationship between the By, V, and the occluded/stented subclavian–axillary artery (A). (c) Centerline reformatting demonstrates the uncompressed, anatomic course of the tunnel.
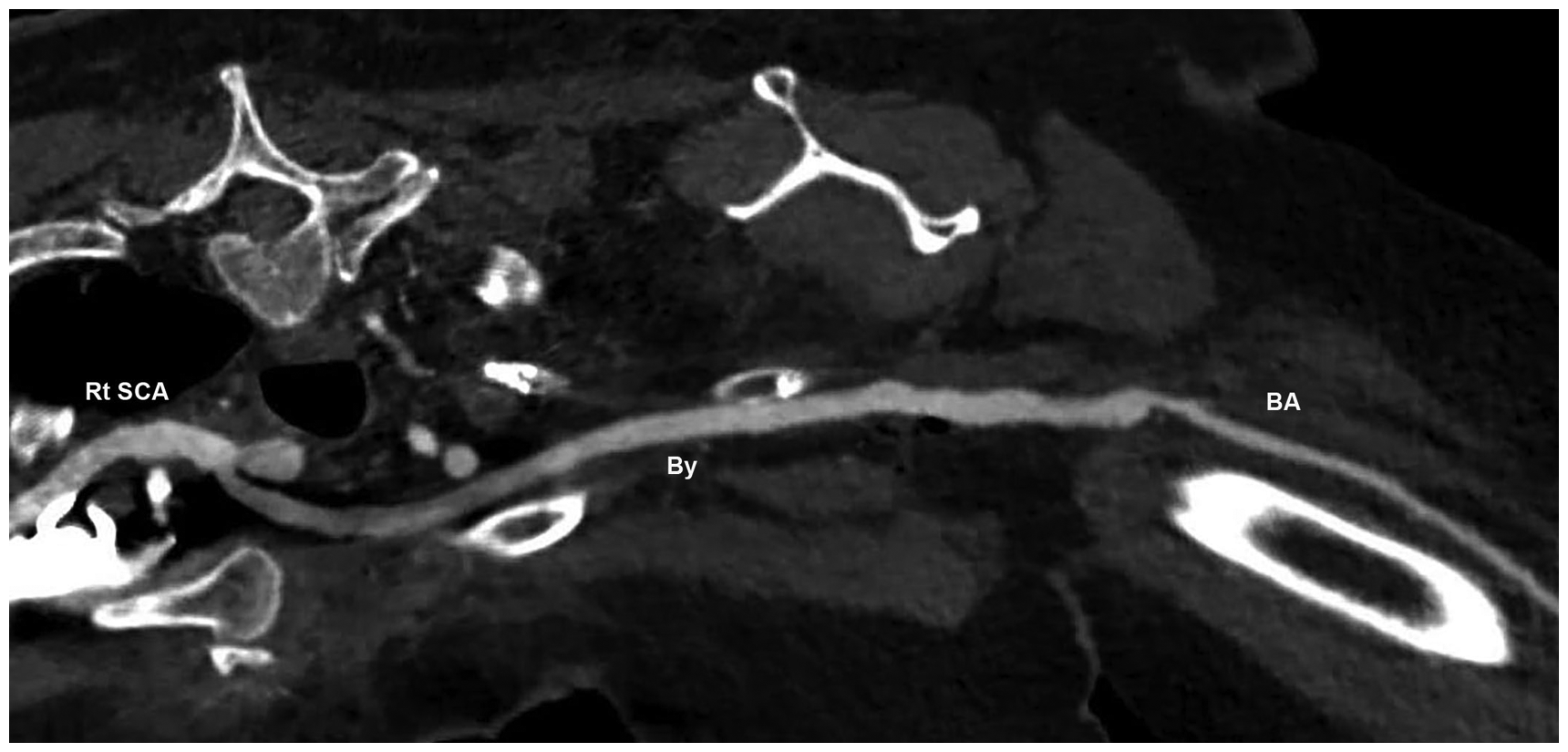
Follow-up imaging of the bypass obtained 2 years after the procedure shows a widely patent bypass without compression through the thoracic outlet.
Discussion
Reoperative vascular surgery can be challenging, especially when coupled with additional risk factors such as prior irradiation and previous stenting.13,14 Moreover, post-radiation arteritis is frequently implicated in occlusive disease of the proximal upper extremity.2,9 Commonly, as in this patient, radiation-related occlusive disease of the proximal upper extremity is associated with radiation therapy as an adjunct in the treatment of breast cancer. Such prior radiation adds to the hostility of the operative field and potentially increases the risk of infection. 1
The pathogenesis of irradiation-induced occlusive disease in large arteries, such as the subclavian and axillary arteries, involves three processes: (1) endothelial injury and disruption of the internal elastic lamina, (2) followed by intimal fibrosis and plaque formation, and (3) occlusion of the vasa vasora which results in both fibrosis of the media and constrictive periarterial fibrosis which results in extrinsic constriction of the artery. Fibrotic occlusion of the irradiated artery is a more delayed process, usually up to 10 years later.12,15
Traditionally, brachial artery revascularization due to axillary–subclavian occlusion could be managed by an extra-anatomic bypass from the carotid to the brachial artery or via endovascular means as both were tried in this case. In our patient, a customized approach had to be considered, given multiple treatment failures and hostility of the surgical field.
Intrathoracic anatomic tunneling was decided upon for the procedure because of suboptimal conventional routes due to prior surgery, radiation therapy, and stenting. It also provided access to intact tissue planes, less radiation damage, non-diseased inflow, and no neurovascular risk. This novel technical approach allowed us to achieve the desired target vessel revascularization while avoiding the hostile features noted previously. The challenge was creating a satisfactory tunnel anatomically through the thoracic outlet with a nonreinforced conduit. The tunnel was carefully created and examined digitally to assure it would accommodate the bypass without compression.
The principle advantage of this technique lies in its avoidance of the hostile operative field and sparing the carotid artery further manipulation in the face of a prior stroke. However, it is a more invasive operation requiring a ministernotomy, and the potential technical difficulty in tunneling the graft needs to be considered. The latter consideration can be overcome with meticulous technique and potentially the addition of a thoracic outlet decompression if necessary.
Footnotes
Acknowledgements
This paper has been presented at the 42nd Annual Meeting of the Midwestern Vascular Surgical Society, St Louis, MO, September 2018.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.