
Abstract
Background
Elective abdominal aortic aneurysm (AAA) repair is advocated in patients where risk of rupture exceeds the risks of peri-procedural morbidity and mortality. Chronic obstructive pulmonary disease (COPD) is a known risk factor for AAA and increased operative morbidity in general. Since literature on the correlation between the clinical classification of COPD and morbidity following endovascular infrarenal AAA repair (EVAR) is scarce, assessment per individual remains a challenge.
Objective
To analyse the pulmonary and all-cause morbidity and mortality in patients with documented COPD and relate this to their GOLD classification.
Methods
Sixty-eight patients with COPD, documented by a lung function test, who underwent elective EVAR between July 2002 and July 2018 were retrospectively reviewed. The primary endpoint was the incidence of 30-day pulmonary adverse events. Procedural characteristics, length of hospital stay, pulmonary and all-cause morbidity including major adverse events (MAEs) during follow-up and five-year survival divided per GOLD classification were the secondary endpoints.
Results
There was no statistically significant difference in the incidence of pulmonary adverse events between GOLD I/II and GOLD III/IV patients. There was neither procedural nor 30-day mortality in either group. Through 30 days and 1 year, there was no difference in pulmonary and all-cause morbidity between groups. Three MAEs occurred in the GOLD I/II group versus 2 MAE in the GOLD III/IV group during the first postoperative year. The five-year survival was 66.0%, 60.9% and 61.9% for patients with GOLD I, GOLD II and GOLD III, respectively. Three of four GOLD IV died within the first year after EVAR.
Conclusion
EVAR can be safely performed in patients with COPD, with low 30-day morbidity and mortality rates. Although severe co-morbidity should be taken into account, EVAR seems to be justified in patients with COPD with a GOLD classification I, II or III. Further research should focus on optimising the pulmonary condition in patients selected for EVAR.
Keywords
Introduction
Patient selection for endovascular abdominal aneurysm repair (EVAR) of abdominal aortic aneurysms (AAA) is based on a comprehensive assessment of risks and benefits. This concerns the risk of aneurysm rupture versus the risk of perioperative morbidity and mortality, as well as the patients’ life expectancy and quality of life.
A positive association between chronic obstructive pulmonary disease (COPD) and the prevalence of AAA has been established. Between 7% and 11% of patients with COPD will eventually develop an AAA. 1 COPD is considered to be a risk factor for both AAA growth and rupture and also increases the operative risks.1–4 In a review of literature, it was shown that COPD leads to higher 30-day/in-hospital mortality after open surgical repair (OSR) and higher all-cause mortality during follow-up, regardless of the type of treatment. 5 Compton et al. retrospectively compared OSR (N = 20) with EVAR (N = 24) in a group with oxygen (O2)-dependent COPD. They reported no 30-day mortality, but the morbidity was significantly higher after OSR. Survival did not differ between groups and after 42 months almost half of the patients were still alive. Compton et al. compared their results to an untreated 6 cm AAA cohort with a survival of 20% at 34 months, suggesting that EVAR should be preferred over a conservative treatment in patients with O2-dependent COPD. Still, COPD has been related to a prolonged hospital stay compared to standard-risk patients. 6 In addition, O2 dependency resulted in an increased incidence of pulmonary complications, major adverse events as well as a reduction in early extubation and a lower five-year survival.
The aforementioned studies were unable to correlate the state of disease with standardised lung function tests. 7 To optimise the individual required approach for AAA repair, complications of EVAR in patients with COPD should be categorised according to their clinical classification. Nowadays, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification is widely accepted to classify patients with COPD. The 2007 classification system was adapted in 2011 and further refined in 2017 (Figure 1). The 2007 strategy classified COPD based on airflow limitation measured with spirometry. Airway obstruction is diagnosed with a fixed forced expiration volume/forced vital capacity ratio (FEV1/FVC) below 0.7. In 2011, the GOLD strategy was refined. Risk assessment was no longer purely based on spirometric grade, but on a combined assessment of severity of obstruction and exacerbation history, using the modified Medical Research Council Dyspnoea symptoms scale (mMRC) or the COPD Assessment Test (CAT). 8 In 2017, the GOLD strategy, spirometry is solely used for diagnosis of airway obstruction. Exacerbation history and current symptoms provide the risk assessment dividing patients in categories A, B, C and D (Figure 1). In literature, the 2017 ABCD categorisation has not proven to be superior to the 2007 and 2011 GOLD strategy in predicting hospitalisation, all-cause and respiratory mortality.
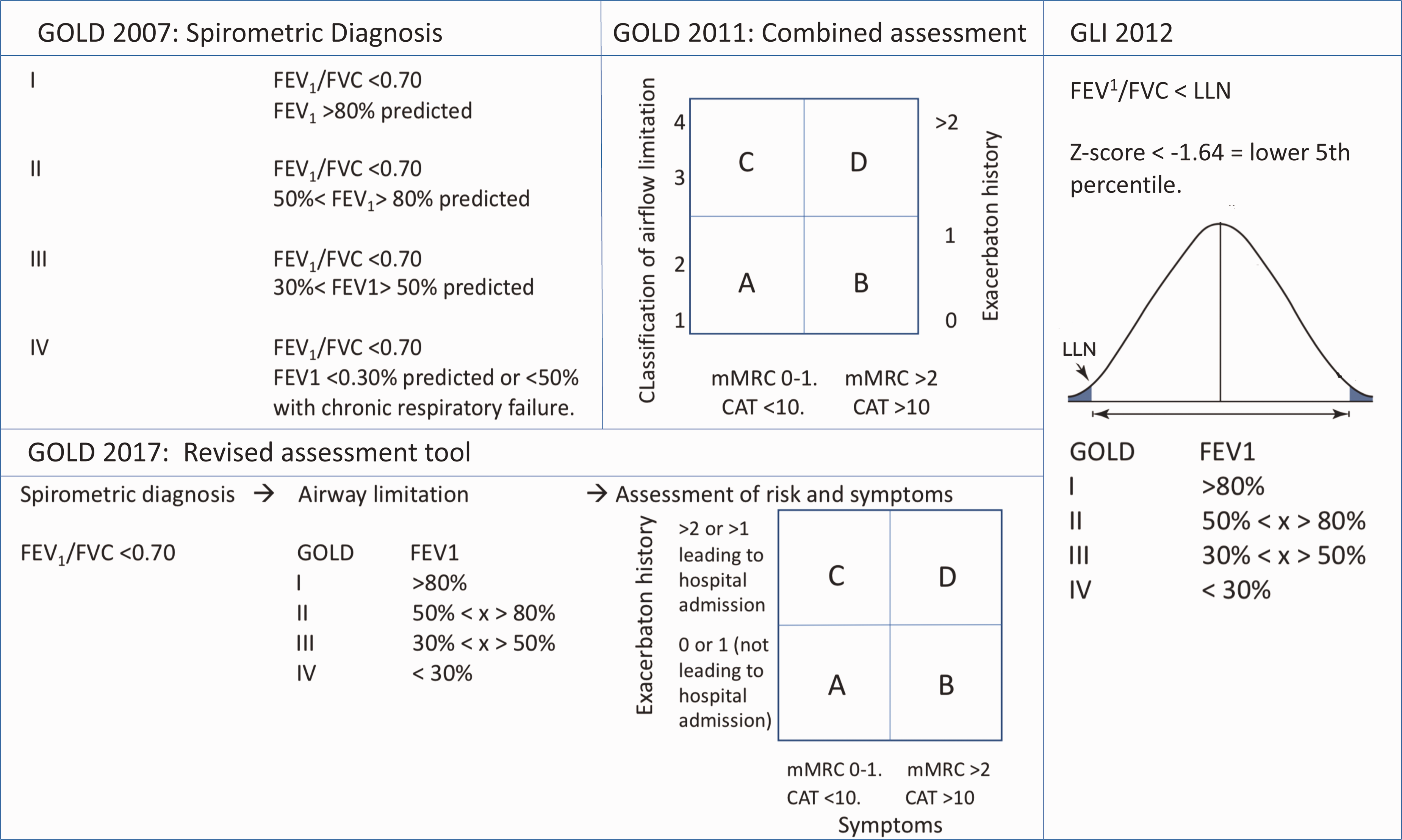
Overview of COPD classifications used. GOLD: Global Initiative for Chronic Obstructive Lung Disease; GLI: Global Lung Initiative; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; LLN: lower limit of normal; mMRC: modified Medical Research Council; CAT: COPD Assessment Test.
In all of the GOLD strategies mentioned above, airway obstruction is set by a fixed ratio. It has been demonstrated that this fixed ratio may lead to age-, height-, and sex-related bias. 9 Therefore, the Global Lung Initiative (GLI) proposed a different definition of airflow limitation where COPD is defined by spirometry with an FEV1/FVC ratio below the fifth percentile of this ratio derived from the general population; the lower limit of normal (LLN), instead of a fixed percentage. Categorisation would still be according to the GOLD I–IV categories derived from the 2007 guideline. 10 In the Netherlands, COPD management was according to this GLI 2012 guideline until 2018, when the burden of disease was included in the risk management as described in Figure 1.
The aim of this study was to evaluate the early complications, especially of pulmonary origin, and survival rate following elective EVAR for an infrarenal AAA in patients with documented COPD. Additionally, the association between these complications and COPD classification was evaluated.
Method
Study design
Approval for the study was obtained by the Medical Ethics committee (a waiver was obtained (2017–1057; NL26327.091.09) and the local institutional review board to perform this retrospective study.
All patients diagnosed with COPD GOLD I, II, III or IV by a pulmonologist, and documented by a lung function test, who underwent endovascular elective infrarenal abdominal aortic repair between July 2002 and July 2018 were retrospectively reviewed from the local abdominal aneurysm database. An infrarenal aneurysm was defined by having a segment (≥10 mm) of non-aneurysmal aorta between the renal arteries and its origin. Patients with a ruptured or symptomatic AAA, a juxtarenal AAA (origin less than 10 mm distal from renal artery), an iliac artery aneurysm requiring an iliac branched device and patients with a follow-up of less than one month were excluded. Patients with reported COPD in the absence of a lung function test were excluded. The inclusion process is displayed in Figure 2.
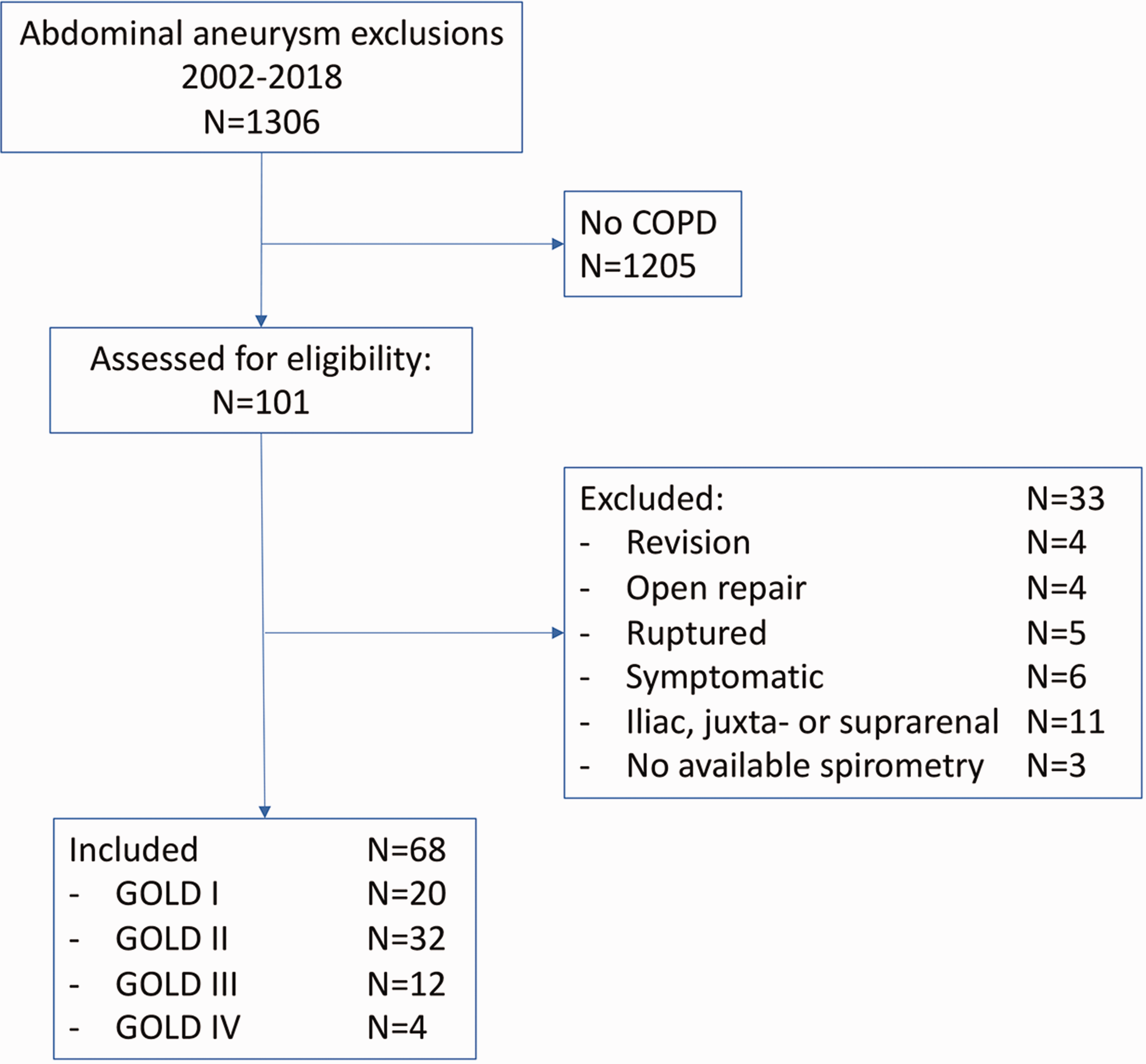
Inclusion flow chart. COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Obstructive Lung Disease.
Baseline patient characteristics including co-morbidities, hospitalisation, type of procedure, per- and postoperative complications, and pulmonary and vascular follow-up details up to 12 years were recorded in a validated online database with audit trail (‘The research manager’, Deventer, the Netherlands).
Preoperative optimisation of pulmonary condition through the use of inhalation therapy prior to surgery was evaluated by assessing hospitalisation records.
Definitions
In 2011, 2012 and 2017 the definition of COPD changed falling within our study period. 11 In this study, we have classified the patients using the original GOLD 2007 definition (Figure 1). The reason for choosing the original classification was the absence of the LLN in most patients that were diagnosed before 2011. Similarly, the use of mMRC and CAT questionnaires was not common practice in the Netherlands during our study period. Furthermore, the 2017 GOLD classification has not proven to be superior in predicting morbidity, mortality and complications compared to the GOLD 2007 and 2011 guideline.
In addition, the impact of the GLI definition, with the use of the LLN, on the outcome was assessed.
Endpoints
The primary endpoint was the incidence of 30-day pulmonary adverse events. Secondary study endpoints included procedural characteristics, length of hospital stay, pulmonary and other complications during follow-up and survival, divided per GOLD classification. Major adverse events (MAEs) at one month and one year were assessed and are categorised as: bowel ischemia, myocardial infarction, paraplegia, renal failure, respiratory failure, secondary endovascular procedure, stroke, procedural blood loss ≥1000 mL or death (related or unrelated to the procedure). Procedural blood loss was estimated by combining the suctioned blood volume and weight of the gauzes used.
Endpoints were defined according to the reporting standards of the Society of Vascular Surgery (SVS), revised in 2018. 12 Co-morbidities that were scored are diabetes, hyperlipidemia, hypertension, renal insufficiency, renal function and cardiac co-morbidity. 12 Co-morbidities were scored according to the SVS co-morbidity scale. 13
Pulmonary adverse events were an upper respiratory tract infection, pneumonia, bronchitis, pneumonitis, exacerbation COPD, lung embolism, pneumothorax or lung cancer.
Statistical analysis
Continuous variables are presented as mean and standard deviation or median and interquartile range (IQR) if applicable. Categorical data are presented as number followed by percentage. Normality was tested using the Kolmogorov–Smirnov test. The procedural characteristics were not normally distributed; hence a nonparametric independent sample test was performed for the procedural type, access type, type of anaesthesia used and the presence of an endoleak.
Since the number of patients included was not normally distributed over the two categories, postoperative complications were also compared using a nonparametric independent sample test.
Survival was analysed using Kaplan–Meier analyses including censoring for patients lost to follow-up and differences between groups tested using the log-rank test.
Two-sided p value < .05 was considered significant. Statistical analyses were performed using IBM SPSS Statistics (SPSS version 25.0 for windows, IBM Corporation, Armonk, NY, USA).
Results
A total of 101 patients with documented COPD underwent EVAR for an infrarenal AAA between July 2002 and July 2018. Thirty-three patients were excluded for various reasons. Sixty-eight patients eventually met the inclusion criteria, divided over GOLD I (N = 20), GOLD II (N = 32), GOLD III (N = 12) and Gold IV (N = 4).
Baseline characteristics divided by COPD I or II patients and COPD III and IV patients are displayed in Table 1.
Baseline characteristics of 68 patients divided in GOLD I/II or GOLD III/IV classification.
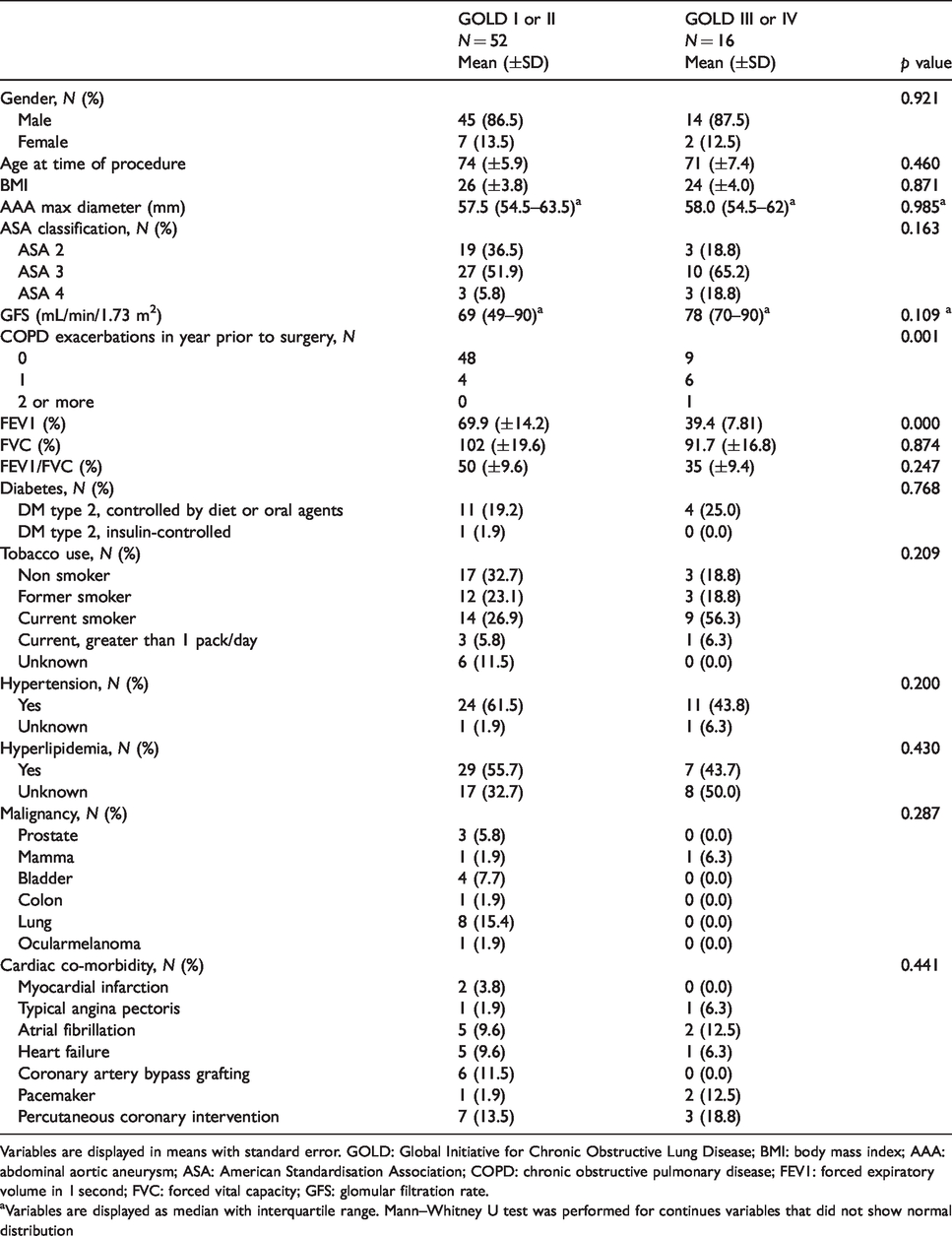
Variables are displayed in means with standard error. GOLD: Global Initiative for Chronic Obstructive Lung Disease; BMI: body mass index; AAA: abdominal aortic aneurysm; ASA: American Standardisation Association; COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; GFS: glomular filtration rate.aVariables are displayed as median with interquartile range. Mann–Whitney U test was performed for continues variables that did not show normal distribution
There were no statistical differences in baseline characteristics between groups. The FEV1 was significantly lower in the COPD GOLD III/IV patients compared to those with GOLD I/II and they did have more exacerbations of COPD in the year before EVAR.
In both groups, most patients were treated under spinal anaesthesia: 29 (56.0%) in the GOLD I/II group and 11 (68.8%) in the GOLD III/IV group. One patient with GOLD I/II (1.9%) and 2 in the GOLD III/IV group (12.5%) were treated using local anaesthesia. Three patients (18.8%) with GOLD III/IV were treated under general anaesthesia, compared to 21 with GOLD I/II (40.3%) (p = 0.097). Forty-four patients (84.6%) with COPD GOLD I/II were treated with regular EVAR compared with 14 (87.5%) with GOLD III/IV (p = 0.776).
Procedural characteristics are displayed in Table 2.
Procedural characteristics of 68 patients divided in GOLD I/II or GOLD III/IV classification.
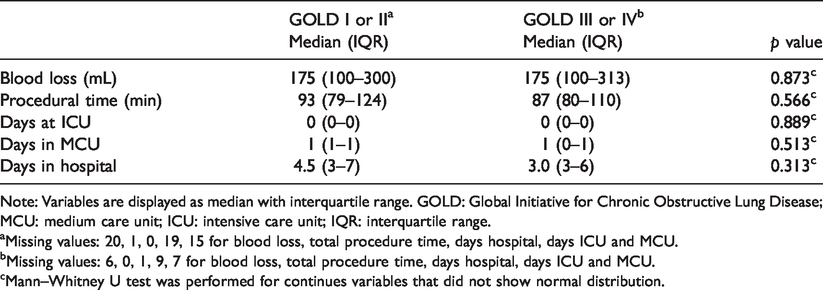
Note: Variables are displayed as median with interquartile range. GOLD: Global Initiative for Chronic Obstructive Lung Disease; MCU: medium care unit; ICU: intensive care unit; IQR: interquartile range.
aMissing values: 20, 1, 0, 19, 15 for blood loss, total procedure time, days hospital, days ICU and MCU.
bMissing values: 6, 0, 1, 9, 7 for blood loss, total procedure time, days hospital, days ICU and MCU.
cMann–Whitney U test was performed for continues variables that did not show normal distribution.
There were no differences in procedural characteristics and duration of hospitalisation between GOLD I/II and GOLD III/IV. There was no 30-day mortality in either group. The complications within 30 days and through 1 year are displayed in Table 3.
Pulmonary and all-cause complications and major adverse events within one month and one year divided in GOLD I/II or GOLD III/IV classification.

Note: Complications are displayed as number and percentage of total complications within one arm. COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Obstructive Lung Disease; MAE: major adverse events.
The 30-day pulmonary complication rate was 4.4% with an overall complication rate of 26.5%. Through 1 year, the overall pulmonary event rate was 29.4%, without differences between groups at any time point.
Two major adverse events occurred within 30 days; one patient with GOLD II suffered from an out of hospital cardiac arrest and another, with GOLD IV from a duodenal obstruction, which was treated by a gastric feeding tube placed beyond Treitz. After three months, a cerebrovascular accident occurred in both groups. Furthermore, a ruptured aneurysm occurred in a patient with GOLD II and emergency open aneurysm repair was successfully performed. Overall, through one year, 3 (5.8%) MAEs (excluding death, which is described below) happened in the GOLD I/II group versus 2 (12.5%) MAE in the GOLD III/IV group (p = 0.584).
Figures 3 and 4 display the Kaplan–Meier survival curves of patients with COPD who underwent EVAR.

Kaplan–Meyer survival curves for GOLD I/II and GOLD III/IV. The table displays the numbers at risk and survival estimates each year. GOLD: Global Initiative for Chronic Obstructive Lung Disease.
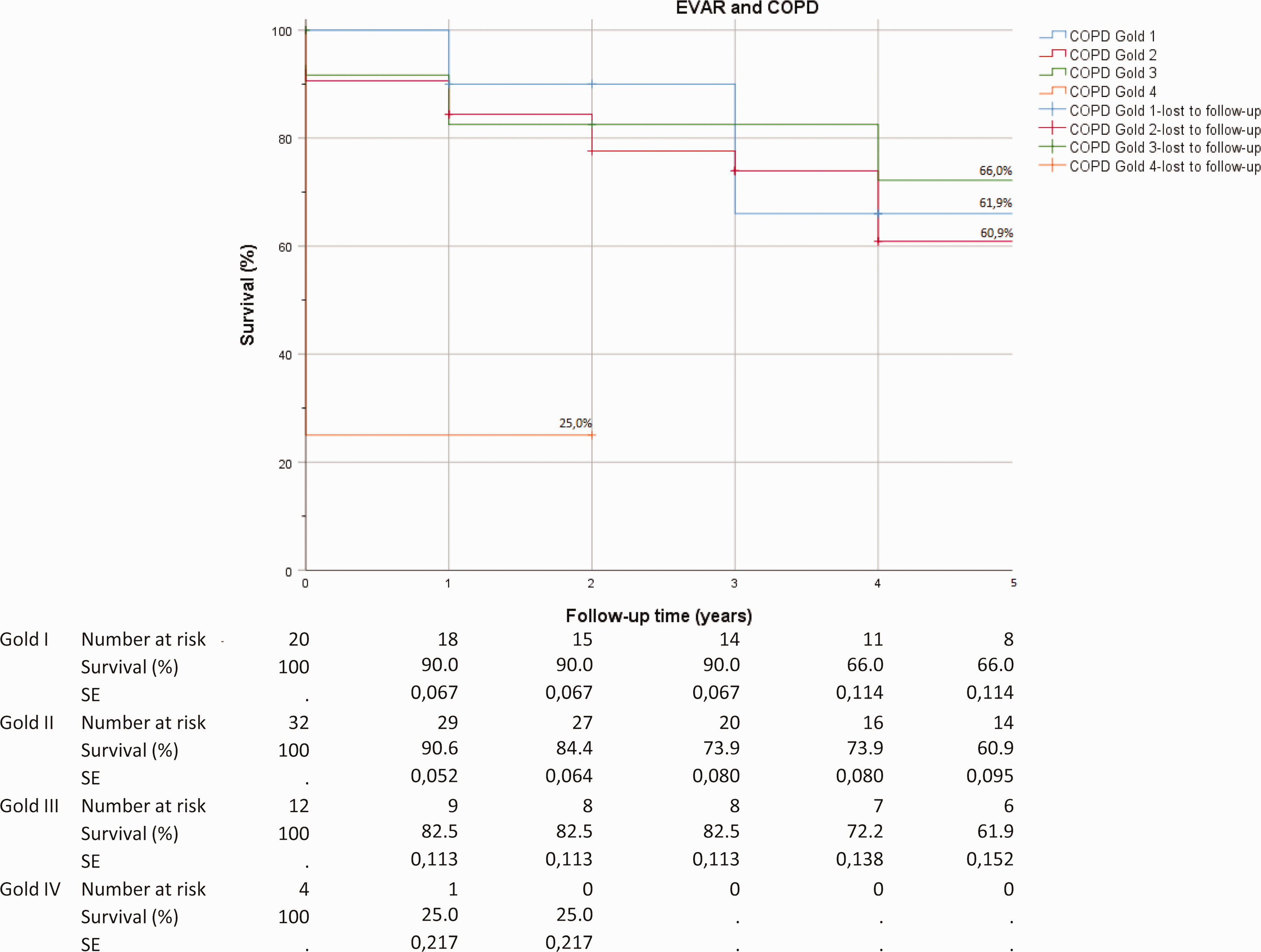
Kaplan–Meyer survival curves for each COPD GOLD classification separately. The table displays the numbers at risk and survival estimates each year. GOLD: Global Initiative for Chronic Obstructive Lung Disease.
The overall five-year survival was 62.3%. The five-year survival was 66.0%, 60.9% and 61.9% for patients with GOLD I, GOLD II and GOLD III, respectively. When the GOLD classification was analysed separately, a statistically significant difference was found between the gold IV class and the other classes (p = 0.003). Three out of four patients with GOLD IV died within four months after EVAR. One died of respiratory failure due to COPD and congestive cardiac failure, two others died of oncological co-morbidities. The fourth was lost to follow-up after two years. The overall estimated survival was 6.3 years (95% confidence interval (CI): 4.5–8.2 years) in GOLD I, 5.4 years (95% CI: 4.1–6.8 years) in GOLD II, 7.2 years (95% CI: 4.5–9.8 years) in GOLD III and 0.5 year (95% CI: 0–1.3 years) in GOLD IV, respectively. Main causes of death were dyspnoea in end-stage COPD, end-stage congestive heart failure and malignancies.
Discussion
In this study, we found that EVAR can safely be performed in patients with COPD with a GOLD classification I, II and III, with a low pulmonary and major adverse event and an acceptable survival rate. A GOLD III classification did not increase the early or late morbidity rates compared to mild COPD, GOLD I or II, nor did it increase admission time on the intensive care unit or in the hospital. An early benefit on survival was observed in patients with GOLD I/II, but this was lost after three years of follow-up. The early survival of patients with COPD GOLD IV was very low. With the very small sample size, however, a hard statement of patients with GOLD IV cannot be made and clinical relevance of elective EVAR in these patients remains subject to debate. Previous studies also observed decreased survival and increased morbidity rates in severe COPD compared to mild or moderate COPD. In these cases, severe COPD was defined by O2 dependency instead of pulmonary function tests.6,7 In most states of America as well as most European countries, stratification of disease severity is based upon the degree of airflow limitation in four stages set forth in the GOLD strategy, either with COPD diagnosed with a fixed percentage or an LLN for the FEV1/FVC ratio. To support generalisation, it is therefore favourable to compare the morbidity and mortality rates after EVAR in patients with COPD according to this stratification. In our study, the original COPD classification of 2007 was used. When we would re-categorise our cohorts into the GLI 2012 guideline, only one patient within in the GOLD I or II group, would not have been diagnosed with COPD using the LLN. As a consequence, our results would not change when we would have applied the GLI 2012 classification system.
Only one other study used spirometry in analysing morbidity and mortality rates in patients with COPD after EVAR. Ohrlander et al. found that, in a combined medical severity index, GOLD grade 3 (hazard ratio (HR): 2.06; 95% CI: 1.24–3.42) and grade 2 (HR: 1.45; 95% CI: 0.99–2.10) were independently associated with long-term mortality and higher short-term morbidity. 14 In contrast, we did not observe a difference in perioperative morbidity and mortality following EVAR between the different GOLD classifications. Within 30 days, more minor (pulmonary) adverse events occurred in patients with GOLD I/II compared to GOLD III/IV. Surprisingly, in the latter group, no pulmonary adverse events occurred. This difference might be explained by a combination of factors. Relatively, more patients with GOLD I/II received general anaesthesia (p = 0.097), though the three patients with COPD gold III who did undergo general anaesthesia did not experience a pulmonal complication within 30 days. The results however do suggest that (loco)regional might be the preferred method for anaesthesia in patients with COPD, to limit influence of general anaesthesia on pulmonary complications.
Another factor which could have affected the difference in short-term pulmonary adverse events is the potential bias that patients with severe COPD may have been monitored more closely and could have been treated more frequently with physical therapy to improve lung clearing. Unfortunately, we could not confirm this reliably from the case files.
Also, within one year, there was no difference in pulmonary complications between GOLD I/II or GOLD III/IV, p = 0.691. It is very likely that the high morbidity rate in gold I/II might be partly attributed to oncological co-morbidity. Moreover, 15.4% of patients with gold I/II who received an EVAR previously had lung cancer, compared to 0% of patients with gold III/IV. Long-term morbidity and survival following EVAR is largely dependent on non-aneurysm related events, but due to complications of severe co-morbidity. 15 Surgical management should therefore be considered carefully in patients with severe co-morbidity like malignancy or chronic diseases of other origin.
The observed five-year survival rates in this study tend to be higher compared with those described by Ohrlander et al. 15 Also, previous research by Compton et al. with O2-dependent COPD showed a lower survival rate of 42%. Compton et al. did however not stratify for the type of aneurysm exclusion or correlate this to a GOLD classification. The survival rates described by Compton et al., Ohrlander et al. and our survival rates were significantly lower than the natural course of survival of COPD patients. 16
In the literature, 30-day mortality after elective EVAR for infrarenal AAA exclusion is 1.3–1.6%, with a pneumonia being the most common pulmonary complication with a prevalence of 3.8% within 30 days. 12 The mean five-year survival rate following elective EVAR is 68%. 17 In our study, we observed a 30-day mortality of 0%, an overall incidence of pneumonia of 3.8% and an overall five-year survival of 62.3%. These data thus appear to be in line with the numbers within a general population. 17
There are a number of other factors that might explain the different findings of Ohrlander’s study and ours. Ohrlander did not display the amount of missing data per variable, although in retrospective research, missing data are very likely to occur. Another explanation might be pulmonary rehabilitation prior to surgery. Ohrlander et al. stated that preoperative assessment of lung function with spirometry and arterial blood gas analysis is common practice at their institution. 14 However, they did not mention whether patients were admitted and started inhalation therapy in preparation for surgery. In our hospital, it is common practice to start inhalation therapy with salbutamol/ipratropium in patients with COPD the night prior to surgery to optimise the pulmonary status. Unfortunately, exact numbers and doses of inhalation steroids are missing due to insufficient documentation. We are unable to make any statement regarding this issue. Preoperative optimisation might have differed within our cohort, leading to bias.
Currently, a new type of pre-habilitation is studied extensively in patients with COPD who will undergo surgery, especially for lung cancer. Pre-habilitation is a concept umbrella heralding the preoperative optimisation of nutritional and functional status. Although an exact definition lacks, frequently used techniques include aerobic exercises, through walking/cycling, resistance training and deep breathing exercises for several weeks prior to surgery. In a systematic review, preoperative exercise training resulted in a decrease of postoperative pulmonary complications (relative risk: 0.33, 95% CI: 0.17–0.61) and a shorter length of hospital stay (−4.23 days, 95% CI: −6.14 to −2.32). The quality of evidence in the included studies was low and bias high. Further research is needed to determine the effect of pre-habilitation on postoperative mortality and morbidity after endovascular aneurysm exclusion.
This study has limitations. Due to the retrospective character of this study design, there are missing data on a number of variables which could have influenced the outcomes. Besides this, our study was not powered to perform a multi-variate regression analysis to measure the influence of mechanical ventilation during general anaesthesia or device and access type on the peroperative, short-term and long-term morbidity and mortality following EVAR. To be able to quantify this effect, a larger study population will be necessary.
Also, we did not include a control group without COPD, for the simple reason that it is not common practice to perform spirometry before elective EVAR in otherwise healthy patients, and therefore asymptomatic mild obstructive lung disease cannot be ruled out in a control group.
Moreover, during the study period, a substantial portion of chronic health care in COPD patients in the Netherlands has shifted from hospitals to general practitioners. Most of the patients with mild pulmonary obstruction, GOLD I and II, only visit hospitals in case of an exacerbation or no satisfying disease control in the first line setting. Due to the absence of a nationwide electronic patient system, we might have missed some minor adverse events that happened without the interference of a pulmonologist and therefore were not recorded.
Finally, since it was common practice in the Netherlands to follow the GLI 2012 guideline in COPD management within our study period and thereby diagnose patients with the use of an LLN and categorise them in GOLD I–IV stages, we were not able to correlate our variables to the risk assessment set out in the GOLD 2011 and 2017 strategy. The numbers for subgroup analysis are low and in Kaplan–Meier analysis standard errors exceeded 10%; therefore, the results have to be interpreted with caution and no robust conclusions can be drawn. Further studies are needed to elucidate this issue.
Conclusion
EVAR can be safely performed in patients with COPD, with low 30-day pulmonary adverse event, SAE and mortality rates. Although pulmonary complications are common during the first year after EVAR, the procedure seems to be justified as the five-year survival of patients with COPD GOLD I, II and III is in line with those described for patients without COPD. Further research should focus on optimising the preoperative pulmonary condition of patients selected for elective EVAR.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.