
Abstract
Background
The major mechanisms of arteriovenous graft (AVG) failure due to intimal hyperplasia (IH) are smooth muscle cell proliferation and inflammation. Therefore, carvedilol may improve AVG primary patency because of its anti-proliferative and anti-inflammatory activities.
Methods
The data of end-stage renal disease patients receiving regular hemodialysis were collected from the National Health Insurance Research database. The end point was the first percutaneous transluminal angioplasty (PTA) for AVG failure or death during a follow-up period of two years or the end of 2013. The analysis was calculated with Cox proportional hazard model.
Results
There were 3028 patients treated with carvedilol and 13,704 patients not treated with carvedilol. According to a univariate analysis, the carvedilol group was younger, received more anti-hypertensive medications and platelet aggregation inhibitors, and had higher rates of diabetes mellitus and hyperlipidemia but had lower rates of hypotension and smoking. According to a multivariate analysis, after controlling for covariates, the use of carvedilol for more than 84 days reduced the probability of a first PTA for AVG failure by 9% compared with no use of carvedilol (p = 0.021), but the use of carvedilol for 1 to 84 days did not.
Conclusion
The results of this study indicate that the use of carvedilol for more than 84 days improves the primary patency of AVGs, but the use of carvedilol for less than 84 days does not.
Introduction
Among the alternatives used to ensure vascular access for hemodialysis, arteriovenous grafts (AVGs) have a higher rate of failures, including critical stenosis or occlusion, than native arteriovenous fistulas (AVFs). 1 Such failures are usually caused by the intimal hyperplasia (IH) at a vein-to-graft anastomosis or a draining vein. Therefore, inhibiting IH should be effective in improving AVG primary patency (the interval from AVG placement to first AVG failure).
In terms of pathology, IH is usually caused by smooth muscle proliferation and migration. 2 Among the anti-hypertensive medications, carvedilol has previously been found to be effective in inhibiting vascular smooth muscle proliferation and migration.3–5 Moreover, inflammation is also associated with IH,2,6 and carvedilol has been shown to have strong anti-inflammatory effects.7–9 Therefore, it is reasonable to infer that carvedilol may reduce the risk of AVG failure.
Past research has demonstrated that platelet aggregation inhibitors (PAIs), calcium channel blockers (CCB), angiotensin-converting enzyme inhibitors (ACEIs), and angiotensin receptor blockers (ARBs) are associated with reduced risks of arteriovenous shunt failure.10–12 However, past studies of carvedilol have usually investigated the association between carvedilol and the reduction of mortality in dialysis or heart-disease patients while seldom examining the relationship between AVG failure and carvedilol. Therefore, this study aimed to determine whether carvedilol could improve the primary patency of AVGs.
Material and methods
Data source
It should be noted that a single-institution review might adopt incorrect times for the first interventions for AVG failures since some patients may have received the first such interventions at other hospitals. Therefore, in order to avoid such errors, we analyzed data sourced from a nationwide database.
All of our patients’ data were retrieved from the National Health Insurance Research Database (NHIRD) for Taiwan. The database was established for Taiwan’s National Health Insurance (NHI) system in March of 1995, and according to the 2012–2013 annual report, the NHI system covered 99.5% of Taiwan’s population at that time, with 92% of all the hospitals and clinics in Taiwan having contracts with the system. In the database, the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis code is used to encode patients’ diagnoses, and the ICD-9-CM procedure code is used to encode patients’ procedures.
Besides, since our NHI system is based on a charge system, in addition to providing a database of all procedures, the system provides a calculation cost mechanism for surgical codes (Table 1), and, in this study, the code was named surgery NHI code. To clarify, different ICD-9-CM procedure codes may reference the same surgery NHI code. It is also possible that a given surgery NHI code have a corresponding ICD-9-CM procedure code. At the time of harvesting surgical data from the NHIRD, we used the surgery NHI code to reference ICD-9-CM procedure code.
Surgery codes and their corresponding treatments and points.
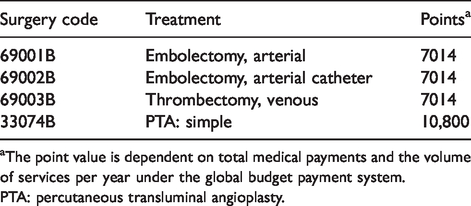
aThe point value is dependent on total medical payments and the volume of services per year under the global budget payment system.
PTA: percutaneous transluminal angioplasty.
Because these patient data were de-identified before being released, this research did not require that informed consent be obtained from the patients whose data were used. The protocol for this retrospective study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (CGMF IRB No. 201801631B1).
Inclusion and exclusion criteria
Because the NHIRD does not include examination or surgical details, and because patients’ data must be harvested through the codes, the design of inclusion and exclusion criteria must be strict to decrease selection error. For example, interventions for one patient’s AVG failure and for another patient’s peripheral artery occlusive disease may have the same surgical code (usually percutaneous transluminal angioplasty (PTA), surgery NHI code: 33074B), and the two patients may coincidently have the same diagnosis of end-stage renal disease (ESRD). Therefore, when obtaining data from the database, it was possible that both of these patients could be enrolled in this study even though they actually had different diagnoses.
For the above reason, all patients’ data were obtained from the Registry for Catastrophic Illness Patients, which is a sub-database of NHIRD. The sub-database contains the patients with catastrophic illness certificates for ESRD. Besides, each of the patients who were enrolled in this study had to fulfill the following criteria simultaneously: having a diagnosis of ESRD (ICD-9-CM diagnosis code: 585) and regularly receiving hemodialysis (ICD-9-CM procedure code: 39.95) for more than three months.
The exclusion criteria were as follows:
Any past use of continuous ambulatory peritoneal dialysis (CAPD), because patients may receive CAPD again after a period of hemodialysis (n = 87); A critical stenosis or occlusion that occurred within one month after surgery, because such issues should be highly related to the surgical technique used, such as the choice of inappropriate (small or fibrotic) vessels (n = 998); The end point occurred before the AVG placement, which may be caused by the incorrect coding of another surgery (n = 8433); and Having a diagnosis of peripheral arterial occlusive disease (ICD-9-CM diagnosis codes: 440.2–440.24, 459.9, 440.4, 447.1, 447.9, 443.9, 445.02) (n = 513) or diabetic foot (ICD-9-CM diagnosis codes: 250.70–250.73, 443.81, 443.89, 249.7, 785.4) (n = 476) during the follow-up period, because these patients may receive surgeries that have the same surgery codes as surgeries for AVG stenosis or thrombosis.
The follow-up period was from the AVG placement (surgery NHI code: 69034 C) until the first PTA for AVG failure or death during a follow-up period of two years or the end of 2013. Because it was difficult to obtain the diagnosis of AVG failure from the NHIRD, it was substituted for by the specific interventions for AVG failure, that is, PTA (surgery NHI code: 33074B) with or without thromboembolectomy (surgery NHI codes: 69001B, 69002B, 69003B). Furthermore, if the main diagnosis for a patient was not ESRD or chronic kidney disease, the data for that patient were also excluded to guarantee that the intervention in question was only for an AVG failure.
Grouping
The patients were classified into a carvedilol group and a no-carvedilol group. In the further classification of the patients in the carvedilol group, the cumulative defined daily dose that was usually used in past NHIRD studies was not used because carvedilol can be excreted by the liver within 24 hours and does not accumulate in patients. 13 Moreover, not only our own clinical experiences but also previous studies have shown that the daily doses of carvedilol actually received by patients are often far less than the defined daily dose (37.5 mg).14,15 Therefore, the total number of days of receiving carvedilol was used for grouping the patients in the carvedilol group for the multivariate analysis. The period of carvedilol used was calculated from one month before an AVG placement to one month before an intervention or completion of the follow-up period. Finally, the patients were further stratified into groups of nonusers of carvedilol, those treated with carvedilol for 1 to 84 days, and those treated with carvedilol for more than 84 days.
Comorbidity and medication selection
The comorbidities and behaviors that were shown to be associated with the risk of IH or arteriovenous shunt failure in past research were included in this study, namely, diabetes mellitus (ICD-9-CM diagnosis codes: 250.00–250.03, 250.80–250.83, 250.90–250.93),16,17 hyperlipidemia (ICD-9-CM diagnosis codes: 272.0–272.4), hypotension (ICD-9-CM diagnosis codes: 458.1 and 458.9), 18 coronary artery disease (ICD-9-CM diagnosis codes: 414.9, 410.9, 411.89, 411.81, 412), hypertension (ICD-9-CM diagnosis codes: 401–405), congestive heart failure (ICD-9-CM diagnosis codes: 428.0, 428.1, 402.9, 425.7), and smoking/smoking-related diseases (ICD-9-CM diagnosis codes: 305.1, 491.2, 492.8, 496, 523.6, and V15.82).19,20
Similarly, medications that may be associated with a decreased risk of arteriovenous shunt failure were included, namely, CCBs (including amlodipine, felodipine, nifedipine, verapamil, diltiazem, isradipine, and nicardipine), ACEIs (including benazepril, enalapril, lisinopril, quinapril, captopril, fosinopril, ramipril, and cilazapril), ARBs (including candesartan, losartan, irbesartan, valsartan, and olmesartan medoxomil), and PAIs (including dipyridamole, acetylsalicylic acid, clopidogrel, and cilostazol). Besides, because marked underestimation of hypotension in the NHIRD was noticed in past research, midodrine, which is usually used to treat chronic hypotension in dialysis patients, was used as a substitute for hypotension in the multivariate analysis. A patient was defined as having used a medication if the patient received the medication for more than 84 days.
Statistical analysis
In the comparison of the patients who took carvedilol and those who did not take carvedilol, the baseline demographic and clinical characteristics were analyzed with Pearson’s chi-square test and Fisher’s exact test. In the further analysis, the Kaplan–Meier method and the log-rank test were performed to analyze the cumulative incidence rates of interventions during the two-year follow-up period. The hazard ratios (HRs) for the carvedilol groups (that is, those treated with it for 1–84 days and those treated with it for >84 days) and the no-carvedilol group were calculated with the Cox proportional hazard model. The analysis was calculated with SAS 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
Data for a total of 26,430 dialysis patients were collected, with 16,732 of those patients being divided into the carvedilol group (3028 patients) or the no-carvedilol group (13,704 patients) (Figure 1). The baseline demographic characteristics indicated that the patients receiving carvedilol were, on average, younger (p < 0.001), had a higher level of urbanization (p < 0.001), and had higher incomes (p < 0.001). With respect to associated medications, the carvedilol group had higher proportions of the use of anti-hypertension medications (that is, CCBs, ACEIs, and ARBs, p < 0.001) and PAIs (p < 0.05) than the no-carvedilol group. In addition, the carvedilol group had higher rates of diabetes mellitus (p < 0.001) and hyperlipidemia (p <0.001) but lower rates of hypotension (p = 0.001) and smoking/smoking-related diseases (p = 0.02). The incidence of significant stenosis or occlusion during the two-year follow-up period was 57.7% in the carvedilol group and 60% in the no-carvedilol group (p = 0.022) (Table 2). Meanwhile, after analyzing our data further, in nonusers and patients treated with carvedilol for 1 to 84 days, the average follow-up time was 417.6 ± 270.8 and 417.1 ±275.2 days, respectively. However, in patients treated with carvedilol for more than 84 days, the average follow-up time was 498.3 ± 229.6 days. This indicates that the patients treated with carvedilol for ≤84 days tended to suffer from AVG critical stenosis or occlusion earlier than the patients who used carvedilol for more than 84 days.
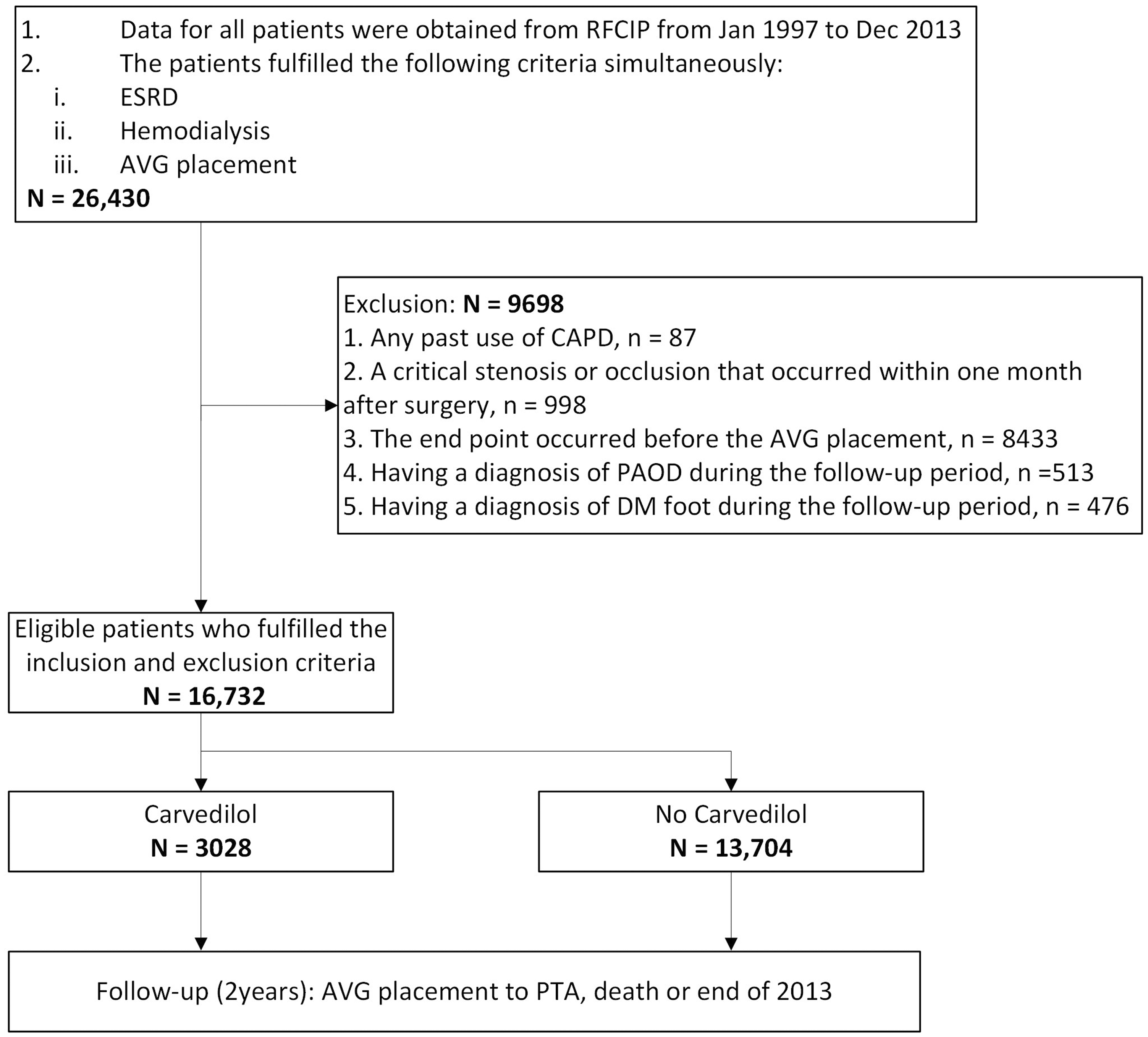
Study enrollment and follow-up.
Baseline demographic and clinical characteristics.
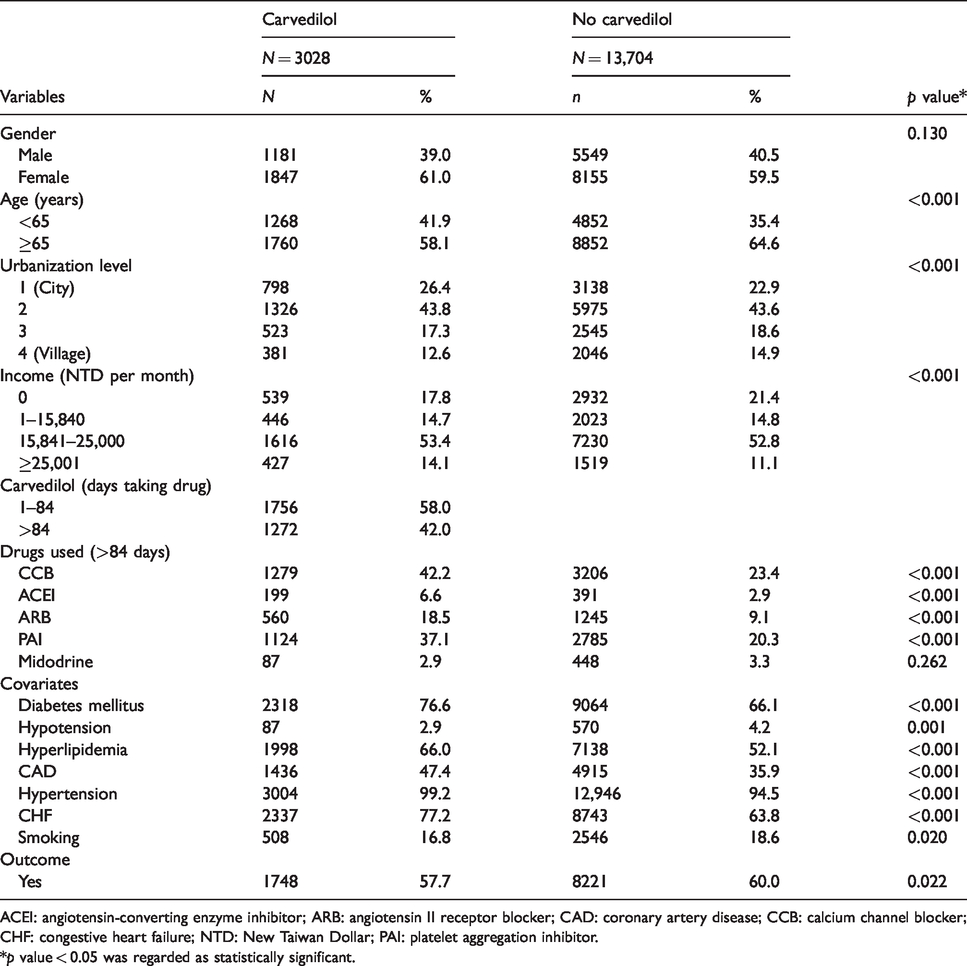
ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; CAD: coronary artery disease; CCB: calcium channel blocker; CHF: congestive heart failure; NTD: New Taiwan Dollar; PAI: platelet aggregation inhibitor.*p value < 0.05 was regarded as statistically significant.
Kaplan–Meier curves indicated that the probability of first PTA for AVG failure was higher in the no-carvedilol group over two years of follow-up (log-rank p = 0.028) (Figure 2). In the multivariate analysis using the Cox model, after controlling for gender, age, urbanization, income, and other medications, the patients receiving carvedilol for more than 84 days had, on average, an 8% reduction in the risk of a first PTA for AVG failure compared to the patients who did not receive carvedilol (nonusers) over two years of follow-up (HR = 0.92; 95% confidence interval (CI) = 0.85–1.00, p = 0.046). However, there was no significant difference between patients receiving carvedilol for 1 to 84 days and nonusers (HR = 1.06, 95% CI = 0.99–1.13; p = 0.076) (Table 3). With superadding adjustment for comorbidities, the direction of the association between the use of carvedilol and the probability of a first PTA for AVG failure did not change, and, similarly, the use of carvedilol for more than 84 days versus nonuse reduced the probability of a first PTA for AVG failure by 9% at any given time for over two years (HR = 0.91, 95% CI = 0.84–0.9; p = 0.021), while the risk for patients receiving carvedilol for 1 to 84 days still was not statistically different from the risk for nonusers (HR = 1.05, 95% CI = 0.98–1.12; p = 0.154) (Table 4).
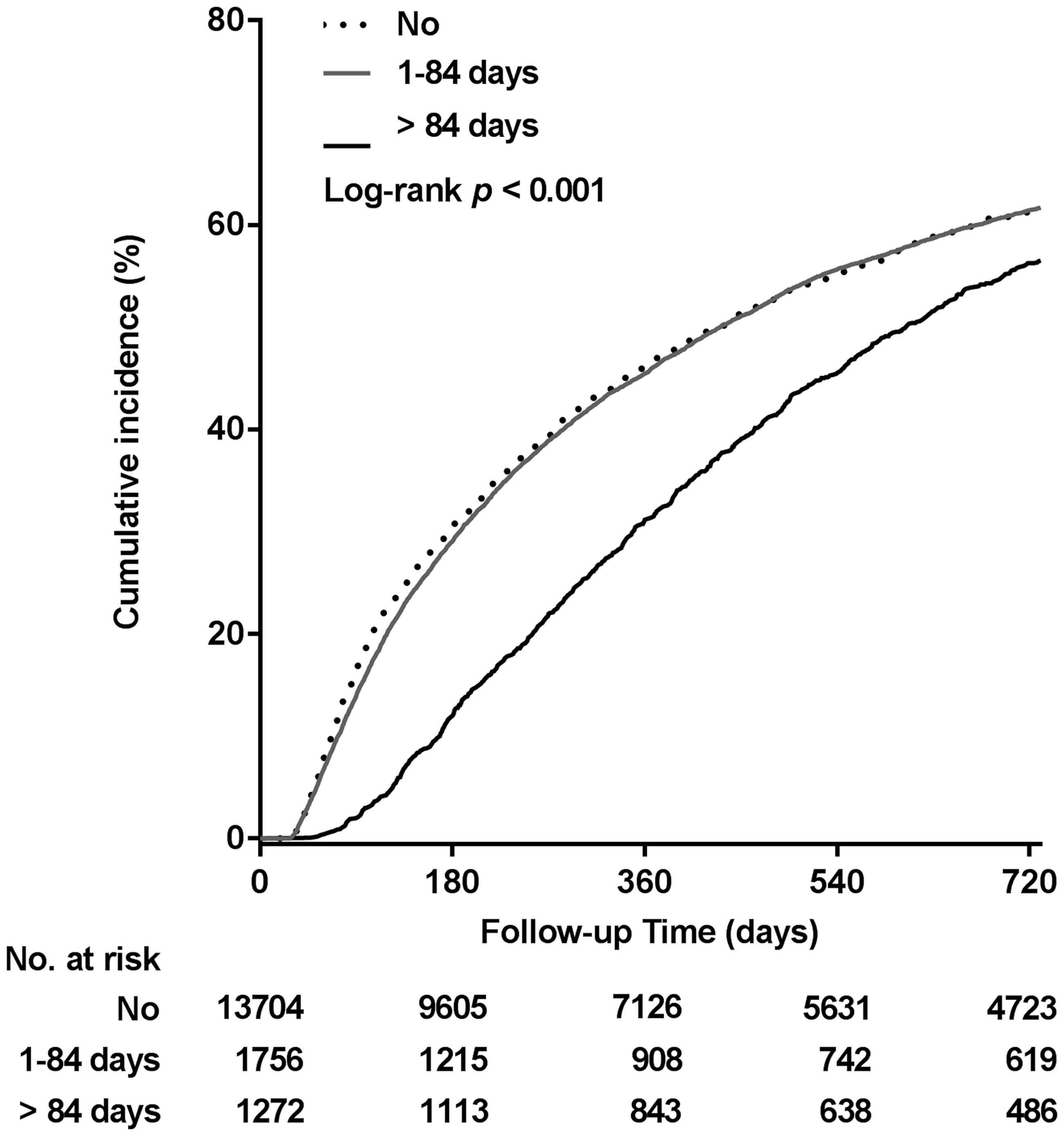
Kaplan–Meier curve of the cumulative incidence of first intervention for AVG failure.
Hazard ratio of patients receiving carvedilol compared with hazard ratio of nonusers, with adjustments for other medications.
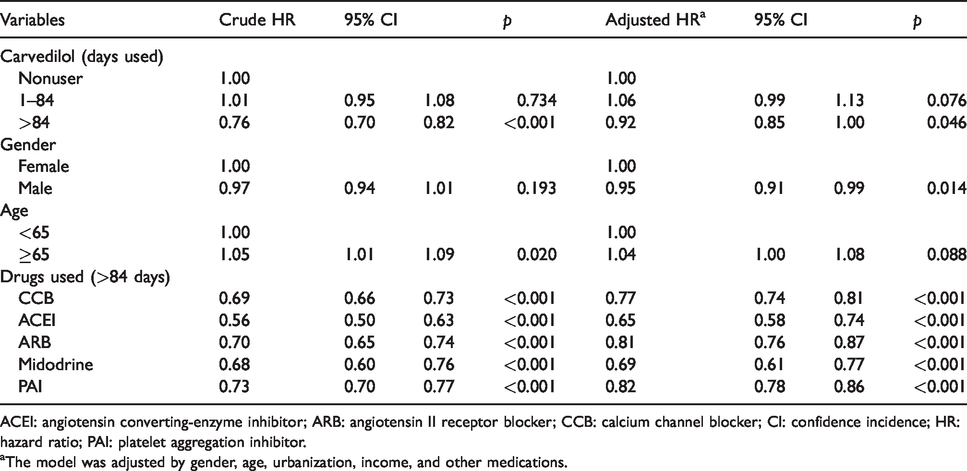
ACEI: angiotensin converting‐enzyme inhibitor; ARB: angiotensin II receptor blocker; CCB: calcium channel blocker; CI: confidence incidence; HR: hazard ratio; PAI: platelet aggregation inhibitor.
aThe model was adjusted by gender, age, urbanization, income, and other medications.
Hazard ratio of patients receiving carvedilol compared with hazard ratio of nonusers, with adjustments for other medications and comorbidities.
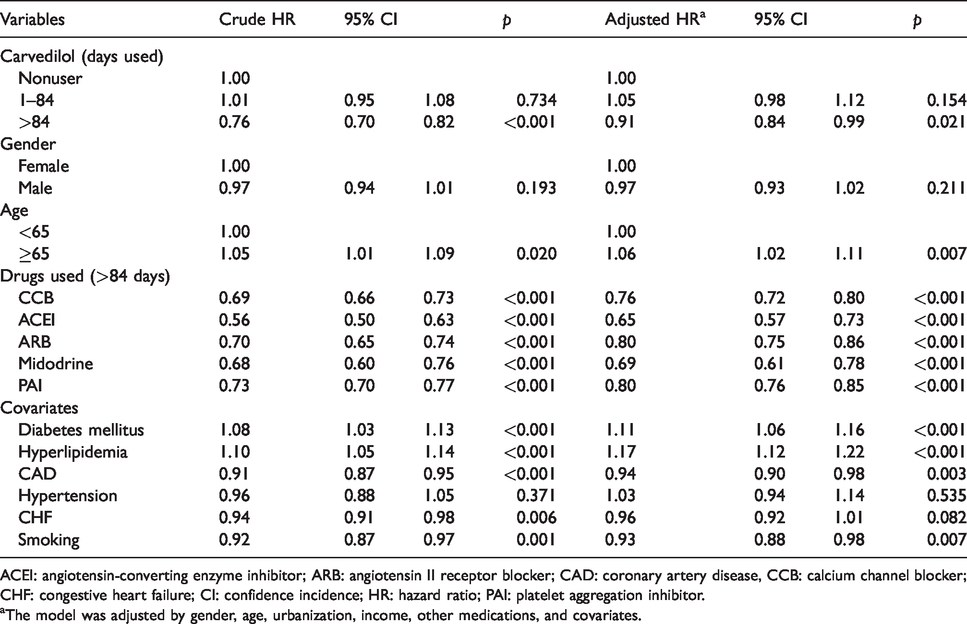
ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; CAD: coronary artery disease, CCB: calcium channel blocker; CHF: congestive heart failure; CI: confidence incidence; HR: hazard ratio; PAI: platelet aggregation inhibitor.
aThe model was adjusted by gender, age, urbanization, income, other medications, and covariates.
Since the two groups had statistical baseline differences in demographics and clinical characteristics, we combined propensity score matching and adjusted for covariates to calculate the HRs again. Similarly, after matching (Supplementary Table 1), the use of carvedilol for more than 84 days versus nonuse reduced the probability of a first PTA with two years by approximate 9% with p = 0.037 (Supplementary Tables 2 and 3).
Discussion
The results demonstrated that the risk of a first intervention for AVG failure was reduced by 9% in the patients who received carvedilol for more than 84 days versus nonusers during a 2-year follow-up period. There were two possible reasons for this result: first, the perianastomotic or draining-vein stenosis was inhibited by the carvedilol due to its effect of inhibiting vascular smooth muscle cell proliferation and migration and its anti-inflammatory effects, or second, the patients who could tolerate long-term carvedilol use potentially also had a lower risk of AVG failure since they usually had hypertension and fair medical compliance.
Patients receiving hemodialysis have higher annual mortality than the general population. 21 After beginning dialysis, the average life expectancy of dialysis patients has been found to be only three to five years. 22 Therefore, prolonging the lifespan of arteriovenous shunts, as the most important life-sustaining tool of dialysis patients, is invaluable to those dialysis patients even though it may only increase their life expectancy by an additional one to two years. Moreover, among the alternatives used to ensure vascular access, arteriovenous shunts have been found to have better long-term outcomes and lower complication rates than cuffed central-venous hemodialysis catheters.23,24 Therefore, massive studies aimed at investigating how to prolong the usage time of arteriovenous shunts have been conducted. Such studies have mainly included three parts: (1) an investigation of the risk factors associated with arteriovenous shunt critical stenosis or occlusion,16,17,19,20 (2) a comparison of different interventional techniques for restoring arteriovenous shunts’ patency,25,26 and (3) an exploration of the medications that could prolong the primary patency of such shunts. However, with respect to the medications that might prolong the primary patency, first, the results of past studies have not been consistent, and second, some medications, such as statins and aspirin, only seem to benefit the patency of AVFs but not AVGs.
Meanwhile, although it is well known that AVGs have shorter longevity and a higher rate of stenosis than other alternatives, 1 they are often the only option for patients with poor vessel quality or a lack of available autogenous vessels. Nonetheless, although carvedilol had previously been shown to be associated with a decreased risk of IH of great saphenous vein grafts in coronary artery bypass grafting, 27 no previous study has mentioned the influence of carvedilol on AVGs’ vein-graft anastomoses neointimal hyperplasia.
On the other hand, in our study, the results of which in this regard were compatible with previous studies,10,28,29 other anti-hypertensive medications, including CCBs, ARBs, and ACEIs, also reduced the risk of AVG failure. These medications may modulate the proliferative response of the vascular wall and suppress neointimal hyperplasia.30–32 Another possibility is that these medications could modify the blood flow velocity of AVGs, which is known to be correlated to perianastomotic stenosis.33,34 Nonetheless, because of the complex mechanisms underlying IH, in the real world, it should be impossible to postpone the occurrence of neointimal hyperplasia through the use of carvedilol alone, and it is therefore reasonable to combine its use with other medications that have been corroborated to decrease the risk of IH.
The most counterintuitive result in this study was the finding that smoking had a protective rather than a harmful effect on AVGs’ primary patency. Although nicotine has been reported to promote IH,35,36 and although it has also been proven that smoking has adverse effects on AVF survival,20,37 it remains uncertain whether or not smoking increases the rate of AVG failure. Valerianova et al. and Girerd et al. revealed that compared to nonsmoking patients, smoking patients had lower AVG thrombosis rates.38,39 Therefore, our result indicating a protective effect of smoking on AVG patency is not unique.
Study limitations
Although the sample investigated in this study was large, the study still had some limitations. First, we could not further group the patients according to the different types of AVGs, such as forearm loop and upper arm bridge AVGs. Nonetheless, the different types of AVGs have different failure rates. Similarly, the surgical techniques and materials used should differ among hospitals and clinics. Second, this study did not consider patients who may have received a new AVG placement after an old AVG had its first occlusion because we supposed that this situation should be very rare. Besides, because of the lack of detailed interventional reports, PTA with or without embolectomy under the main diagnosis of ESRD was used as a substitute for the occurrence of significant stenosis or occlusion of AVGs, so even after excluding other diseases that were also treated with the same procedure as much as possible, there may still have been some patients who were incorrectly enrolled in this study. Finally, as mentioned previously, some diseases may be underestimated in the NHIRD, and this may have caused some inaccuracy in the results. For the above reasons, we struggled to decrease the possible error by applying rigorous inclusion and exclusion criteria. Additionally, since dialysis patients need to receive hemodialysis three times per week at a hemodialysis center, their medical records are usually more complete than those of other patient populations. Therefore, the probability of incorrect estimation should be low.
Besides, because this study was a retrospective cohort study, it was impossible to confirm patients’ compliance with medication intake. However, since the effect of the use of carvedilol >84 days reached a statistically significant difference, even if our patients had a high degree of noncompliance, then the possibility of noncompliance indicated, at most, that we underestimated the effect of carvedilol rather than overestimated it. In other words, the results suggest that carvedilol may improve AVG primary patency even if patients take carvedilol ≤84 days.
Conclusion
The study demonstrated that the use of carvedilol is associated with a lower rate of a first PTA for AVG failure over a two-year period and, more specifically, that the use of carvedilol prolonged the primary patency of AVGs. However, patients had to take carvedilol for more than 84 days to receive this benefit. Nonetheless, the findings of this study have practical implications for the development of medical treatments aimed at delaying the critical stenosis or occlusion of AVGs.
In addition, since carvedilol can improve AVG primary patency, dialysis patients usually have higher rates of hypertension, heart failure, and arrhythmia, and surgery may cause pain, complications (e.g. vascular rupture and graft infection), and considerable expenses; we suggest that those patients should take carvedilol if there is no contraindication. Meanwhile, if a patient has contraindications to the use of carvedilol, there are still other options, such as CCB, ACEI, and ARB, that are also effective for improving AVG primary patency.
Supplemental Material
sj-pdf-1-vas-10.1177_1708538120923886 - Supplemental material for Effect of carvedilol on arteriovenous graft primary patency
Supplemental material, sj-pdf-1-vas-10.1177_1708538120923886 for Effect of carvedilol on arteriovenous graft primary patency by Yuan-Hsi Tseng, Chia-Yen Liu, Chuan-Pin Lee, Meng-Hung Lin and Yao-Hsu Yang in Vascular
Footnotes
Acknowledgments
The authors would like to thank the Health Information and Epidemiology Laboratory (CFRPG6H0021) personnel for their comments and assistance in the data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from Chang Gung Memorial Hospital, Chia-yi Branch, and was based on the National Health Insurance Research Database provided by the Central Bureau of National Health Insurance, the Department of Health, and managed by the National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of the Central Bureau of National Health Insurance, Department of Health, or the National Health Research Institutes.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.