
Abstract
Objectives
While the use of protamine sulfate as a heparin reversal agent has been extensively reviewed in patients undergoing carotid endarterectomy and coronary artery bypass grafting, there is a lack of literature on protamine’s effects on lower extremity bypasses. The purpose of this study was to determine the risk of protamine sulfate dosing after tibial bypass on thrombotic or bleeding events, including early bypass failure.
Methods
We performed a retrospective review of our institutional database for patients undergoing primary distal peripheral bypass from January 2009 through December 2015 (contralateral bypass was considered to be a new primary bypass). Primary endpoints include composite thrombotic events (myocardial infarction, stroke, amputation at 30 days and patency less than 30 days) and composite bleeding events (bleeding or transfusion).
Results
A total of 152 tibial or peroneal bypasses in 136 patients with critical limb ischemia were identified. Of these, 78 (57.4%) patients received protamine sulfate intraoperatively and 58 (42.6%) did not. There were no differences in composite thrombotic or hemorrhagic outcomes. Protamine use had no effect on the rates of perioperative MI (9.0% versus 3.5%, p = 0.20), stroke (1.3% versus 1.7%, p = 0.83), or perioperative mortality (5.1% versus 3.5%, p = 0.64). There was no significant difference in composite post-operative bleeding events (20.7% versus 14.1%, p = 0.31) or composite thrombotic events (17.2% versus 18.0%, p = 0.91). Patients who received protamine undergoing bypass with non-autogenous conduit had significantly higher-recorded median operative blood loss (250 mL versus 150 mL, p = 0.0097) and median procedure lengths (265 min versus 201 min, p = 0.0229). No difference in 30-day amputation-free survival was noted (91.0% versus 91.4%, p = 0.94). Follow-up Kaplan–Meier estimation did not demonstrate a difference in 30-day patency (91.7% versus 88.5%, p = 0.52).
Conclusions
Heparin reversal with protamine sulfate after tibial or peroneal bypass grafting is not associated with higher cardiovascular morbidity, bypass thrombosis, amputation, or mortality. Additionally, there was no statistically significant difference in post-operative bleeding or thrombosis complications for patients who did not receive protamine, although the findings are suggestive of a potential difference in a more adequately powered study. Our results suggest that protamine sulfate is safe for intraoperative use without increased risk of thrombotic complications or early tibial bypass graft failure.
Introduction
Protamine sulfate is used variably in vascular surgery for the reversal of systemic heparin anticoagulation. The decision to administer protamine is often based on the subjective assessment of intraoperative bleeding weighed against risk of thrombosis or adverse reaction from the medication itself. These measures are often extremely subjective and based on physician preference or anecdotal experience. 1
In patients undergoing carotid endarterectomy, protamine sulfate has been shown to be associated with a reduction in bleeding complications without increasing the risk of major thrombotic events such as stroke, myocardial infarction (MI), or death.2–4 However, its use in peripheral tibial bypass has not been thoroughly assessed. Importantly, it has not clearly been determined whether protamine sulfate use in peripheral vascular procedures, particularly involving small tibial vessels, may place a bypass at increased risk for thrombotic complications.
We therefore examined whether protamine sulfate was associated with hemorrhagic or thrombotic complications following lower extremity bypass to the tibial or peroneal vessels. We hypothesized that protamine sulfate administration would not increase thrombotic complications or affect graft patency and amputation-free survival. Rather, we suspected that its use would lead to lower bleeding complications.
Methods
We retrospectively queried a prospectively collected institutional database for all patients who underwent primary distal peripheral bypass from January 2009 through January 2014 by vascular-trained surgeons. Patients were selected using Current Procedural Terminology codes during admission. The distal peripheral bypass codes included bypass graft with vein (including in-situ bypass) and with other than vein from both femoral and popliteal inflow vessels (35566; 35571; 35587; 35666; and 35671). Patients were excluded from the analysis if they presented with acute limb ischemia or traumatic need for revascularization. Re-operative bypasses were also excluded from the analysis, although new primary contralateral bypass did not exclude patients from the study. Bypass procedures were divided into two groups: intraoperative protamine administration and no intraoperative protamine administration. Protamine use was decided intraoperatively by surgeon discretion.
Heparin was given prior to arterial clamping at a dose of 50–100 U/kg. Baseline activated coagulation time (ACT) was measured followed by routine intra-operative ACT monitoring during the procedure with a target level of 250–300 s. Upon completion of the index procedure, hemostasis was obtained using hemostatic agents including thrombin-impregnated gelfoam, oxidized regenerated cellulose, and topical thrombin spray according to operator preference.
Categorical variables evaluated included race, sex, coronary artery disease (CAD), chronic kidney disease (CKD), end stage renal disease (ESRD) requiring hemodialysis (HD), congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), diabetes mellitus (DM), hypertension (HTN), peripheral arterial disease (PAD), indication for distal bypass (severity of vascular disease including claudication, gangrene, non-healing ulcer, rest pain), and American Society of Anesthesiologists (ASA) classification. These were identified through ICD-9 diagnosis codes and verified with manual chart review. Continuous variables evaluated included age, total procedure duration, estimated blood loss, inpatient length of stay, and body mass index. Conduit patency was determined by duplex ultrasound exam.
Primary end points included composite thrombotic events (MI, stroke, amputation at 30 days, and patency less than 30 days) and composite bleeding events (bleeding or transfusion). Secondary outcomes included MI, stroke, graft occlusion, reoperation for bleeding after bypass or amputation, post-operative bleeding and transfusion, and 30-day graft patency. MI was defined as a troponin elevation; electrocardiogram with new Q waves, ST segment, or T-wave changes; or documentation by clinical criteria, echocardiogram, or other imaging modality. Postoperative stroke was defined by new onset neurologic findings including neurologic assessment or radiologic imaging. Bleeding after distal bypass was captured as return to the operating room within 30 days for bleeding.
A univariate analysis was conducted using chi-squared test, Fisher’s exact text, and Wilcoxon rank-sum tests, as appropriate. Kaplan–Meier curves were generated to evaluate 30-day graft patency over time and were compared with log rank test. Perioperative deaths were excluded from Kaplan–Meier analysis. Statistical significance (α) was set at p ≤ 0.05. All statistical analyses were conducted in SAS 9.4 (Cary, NC). The study protocol was approved by the Institutional Review Board of Montefiore Medical Center (IRB# 12–10-364), and given the retrospective nature, informed consent was not required.
Results
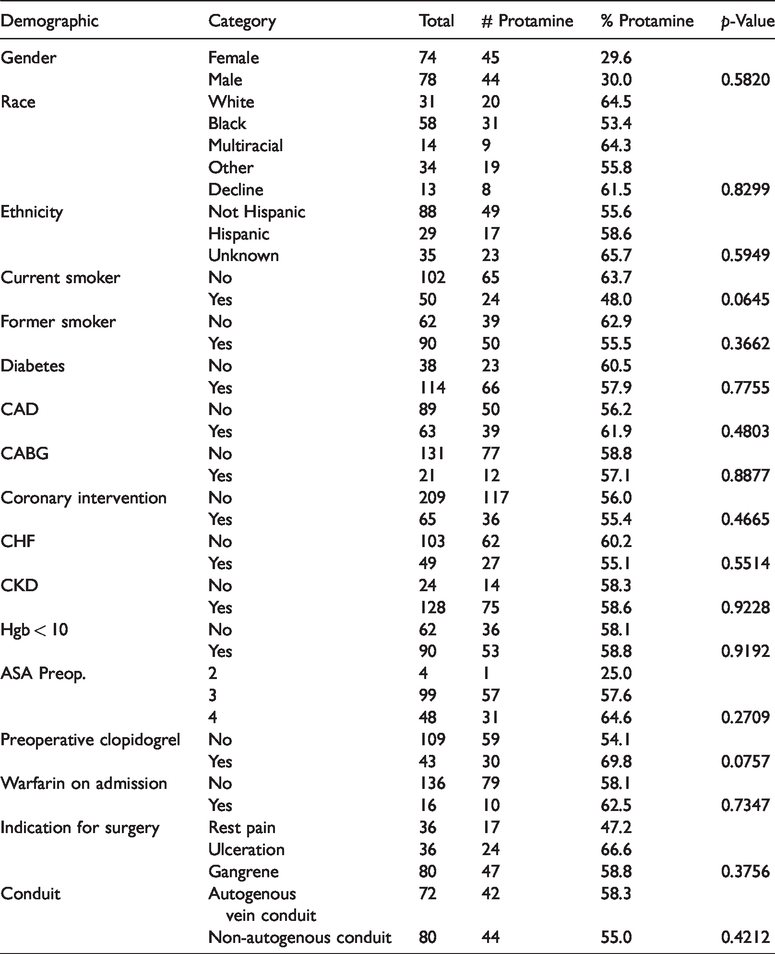
There were 152 distal peripheral bypasses performed in 136 patients from January 2009 to January 2014. Among the study patients, critical limb ischemia was the primary indication for peripheral bypass. Patients were relatively equally distributed with 78 (57.4%) patients receiving protamine sulfate intraoperatively for heparin reversal and 58 (42.6%) not receiving any systemic reversal agent. Inflow was from the external iliac artery (3.9%), superficial femoral artery (39.5%), popliteal artery (5.3%), and the common femoral artery (51.3%). The patient populations were similar in terms of age, sex, race, weight, American Society of Anesthesiology Classification, and preoperative risk factors (Table 1).
Demographics table.
Among patients who received protamine sulfate during tibial bypass, the composite bleeding outcome occurred in 14.1% compared to 20.7% (p = 0.3108), and the composite thrombotic outcome occurred in 18.0% compared to 17.2% (p = 0.9148). When evaluating the individual outcomes, 6.4% had post-operative bleeding events compared with 5.2% of patients who did not receive protamine (p = 0.7616). Blood transfusion was required in 11.5% in patients who received protamine compared to 17.2% of patients who did not receive protamine (p = 0.3427).
No differences were observed overall in operative time and estimated blood loss in the two groups. However, patients who received protamine undergoing bypass with non-autogenous conduit had significantly higher-recorded median operative blood loss (250 mL versus 150 mL, p = 0.0097) and median procedure lengths (265 min versus 201 min, p = 0.0229). No difference for saphenous vein conduit bypasses was noted.
Protamine use had no effect on the rates of’ perioperative mortality (3.5% versus 5.1%, p = 0.6371). There was no effect on rates of MI (3.5% versus 9.0%, p = 0.1998), stroke (1.7 versus 1.3, p = 0.8332), amputation at 30 days (8.6% versus 9.0%, p = 0.9427), units transfused (average 0.27 versus 0.36 U, p = 0.4856), length of stay (9.3 versus 10.7 days, p = 0.5116), reintervention within 30 days (12.1% versus 11.5%, p = 0.9243), or patency at 30 days (84.5% versus 85.9%, p = 0.8178). Additionally, wound healing rates were also similar between patients receiving protamine and those who did not (43.8% versus 41.3%, p = 0.7642). None of the patients receiving protamine experienced an adverse event related to drug administration.
Follow-up Kaplan–Meier estimation (Figure 1) did not demonstrate any long-term difference in 30-day patency overall (91.7% versus 88.5%, p = 0.34) or for saphenous vein conduit (92.1% versus 88.1%, p = 0.57). However, in patients undergoing bypass with non-autogenous conduit, primary patency at 30 days was 95.4% for the protamine arm and 82.1% in patients who did not receive protamine. This difference approached statistical significance with p = 0.093.
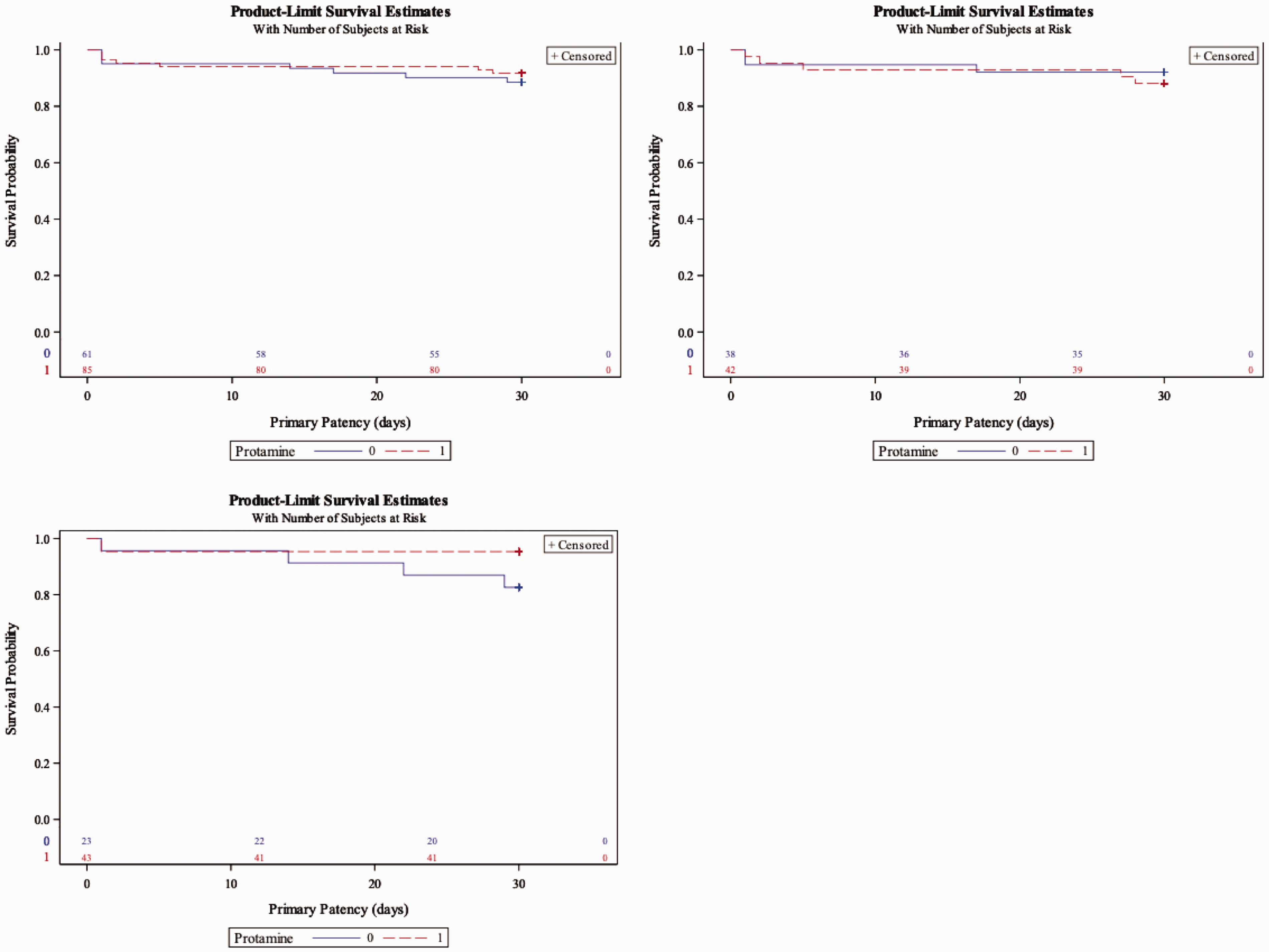
Kaplan–Meyer patency at 30 days comparing protamine versus no reversal in distal bypasses: top left – overall; top right – saphenous vein conduit only; bottom – non-autogenous conduit.
Discussion
Heparin reversal with protamine sulfate is used in a variety of vascular and cardiac procedures. However, the reversal of heparin in peripheral vascular surgery is not fully described. While the use of protamine sulfate has been studied in some procedures, there have been varied conclusions. There are apprehensions that protamine sulfate use may be associated with early thrombosis or decreased patency as well as the possibility of allergic reactions. 5 Similarly, it has been stated that protamine sulfate in peripheral vascular surgical procedures may have harmful effects related to maintaining vessel patency during and after operation because of an abbreviated heparin effect. 6 We observed the opposite trend in patients undergoing non-autogenous conduit tibial bypass.
It is interesting to note that similar concerns were voiced regarding the use of protamine sulfate in carotid endarterectomy and its potential as a catalyst for perioperative stroke. These hesitations were laid to rest after the Vascular Study Group of New England published seminal multicenter results clarifying that protamine in fact reduces bleeding complications and is not associated with an increased risk of stroke. 4 Still, protamine sulfate use has not been extensively studied in patients undergoing other peripheral vascular procedures, specifically tibial vessel bypass. This is especially important given recommendations not to discontinue dual antiplatelet therapy prior to peripheral lower extremity revascularization, 7 and therefore the role of protamine sulfate and the associated risks must be understood.
The overall usage of protamine sulfate in lower extremity tibial bypasses is varied and often dependent on physician experience and preference.8–10 McPhee et al., 11 through propensity matched analysis of all lower extremity bypass patients, have shown that protamine use was not associated with a decrease in bleeding complications or a loss of patency. 11 However, they did not specifically analyze protamine usage in the tibial vessels and the risk for early thrombosis. Importantly, they did note a decrease in the use of protamine in infrapopliteal bypasses due to physician preference. While Farber et al. 5 noted an increase in early thrombosis in arteriovenous fistulas for dialysis access after protamine use, they also noted that stiff, noncompliant feeding arteries were associated with a lower frequency of thrombosis.
The results of our study suggest that heparin reversal with protamine sulfate does not increase the risk of early thrombosis or decreased patency in distal revascularization operations. However, our study has a small sample size, and with adequate power, a difference may have been detected. Certainly, there may be a suggestion of lower composite bleeding rates, and this was likely driven by the rates of transfusion. MI and LOS may potentially reveal differences in an adequately powered study as well. At the least, we demonstrate that administration of protamine does not appear to be inferior to a strategy without protamine administration.
Interestingly, we found that in the protamine reversal group specifically for non-autogenous conduit, patients exhibited a higher blood loss and operative time. This may be reflective of a decision to administer protamine reversal in patients who exhibited higher blood loss or who had non-hemostatic wound beds during surgery and closure. As protamine sulfate use was decided during the procedure by the physician, longer and potentially more difficult cases may have resulted in a tendency of the surgeon to use protamine. Alternatively, surgeons may have waited for completion of protamine infusion prior to wound closure in patients that exhibited poor hemostasis of the general wound bed, thereby increasing the operative time. The exact temporal relationship is difficult to elicit based on our retrospective review. Similarly, increased blood loss was seen with the protamine group in a comparison of protamine use for open repair of abdominal aortic aneurysms (AAA). This study found that in “repair of AAA, total surgical blood loss … and blood loss for the period after study drug administration … was also significantly greater in the protamine group.” 6
While Stone et al. 4 revealed that use of protamine sulfate in carotid endarterectomy may decrease bleeding complications, we found no difference in post-operative bleeding complications for patients who did not receive protamine. We did not find the expected reduction in bleeding events either, which may be due to a difference in the algorithm for management of post-operative bleeding after carotid endarterectomy versus a distal bypass. Bleeding after carotid surgery may lead to airway complications that lead to a lower threshold for reoperation, while bleeding after a bypass may only result in an inconsequential hematoma. Such hematomas may be difficult to identify even with detailed chart review given that often, if inconsequential, they may not be described in the record or even recognized if very small. Importantly though, there is no difference in the need for reoperation in the group receiving protamine reversal as compared to the one that did not.
The use of adjunctive hemostatic agents is another important consideration at the time of surgery. As these hemostatic agents improve, there may be a decreased role for protamine administration. Challenging suture line bleeding can be minimized with fibrin sealant and other topical agents.12,13 While their safety and usefulness have been demonstrated, they may only serve as an adjunct to hemostasis in the heparinized patient. Additionally, the adjunctive administration of desmopressin may aid hemostasis in the uremic patient with platelet dysfunction. Given the infrequency of its use, we are unable to determine the presence of any statistical effect.
Our study’s low incidence of early thrombosis makes it difficult to define the role of protamine in distal tibial bypass. At the least, protamine sulfate administration does not seem to increase thrombotic complications. We did not find any increase in the rates of early graft failure or amputation. Use of protamine in the absence of any clear benefit, while safe, may in fact increase cost, although it is not a particularly expensive medication ($23.29 for 250 mg at our center).
Limitations
We are aware of several limitations in this study, including the selection bias associated with patients undergoing this procedure. Additionally, the sample size is low. While differences in the rates were observed, our study lacked power to detect a statistical difference. We were unable to perform random effect modeling which limits the ability to discern if the null results are driven by individual practitioners. Additionally, the sample size is insufficient to perform a multivariable model; hence the true magnitude of the effect of protamine administration independent of other covariates cannot be quantified. Other limitations of our study include the retrospective nature and lack of randomization regarding protamine administration. Additionally, we were not always able to determine if adjunctive topical and alternative hemostatic agents were used intraoperatively. Finally, WIFi staging could not be performed given the limited granularity of the data available.
Conclusion
Heparin reversal with protamine sulfate after tibial or peroneal bypass grafting does not appear to be associated with any statistical difference in hemorrhagic or thrombotic outcomes. Additionally, we observed a clinically significant but not statistically significant finding of improved 30-day patency when using protamine in patients undergoing non-autogenous conduit tibial bypass. While it was surprising that no clear benefit regarding bleeding complications was noted regarding the use of protamine in heparin reversal, this is likely related to small sample size which along with the selection bias previously mentioned is a limitation in this study. Protamine sulfate reversal also did not exhibit any increased risk of thrombotic events including early graft failure or MI, although with a larger sample size, a statistical difference in MI rates may be identified. The low cost is not necessarily prohibitive of its continued use, especially given absence of any complication related to medication administration. Overall, this study certainly is hypothesis-generating, and further investigations should evaluate the safety and efficacy of protamine administration.
Footnotes
Acknowledgements
The article is presented at the Society of Clinical Vascular Surgery 45th Annual Symposium: ePoster.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.