
Abstract
Objectives
Vascular access site complications after percutaneous transfemoral cardiovascular procedures remain a common cause of morbidity and mortality. We evaluated the SiteSeal® VCD for achieving hemostasis following diagnostic cardiac catheterization.
Methods
We conducted a prospective case control single center study to assess the safety and efficacy of SiteSeal® VCD compared to standard manual compression following diagnostic cardiac catheterization. Forty patients were enrolled in study to receive either SiteSeal® device or manual compression (20 in each group).
Results
Patients in the SiteSeal® group achieved hemostasis in a significantly shorter time (4 ± 2.4 vs. 19 ± 2.4 min, P < 0.001), had shorter time from hemostasis to ambulation (95 ± 44 vs. 388 ± 63 min, P < 0.001) and significantly earlier device deployment to discharge time compared to the manual compression group (4.7 ± 1.1 vs. 8.9 ± 4.8 h, P = 0.001). There was one non-major bleeding event in the SiteSeal® group which occurred >24 h after discharge from the hospital and was managed conservatively. In the remaining device patients, there was no clinical or Doppler ultrasound evidence of major or minor vascular complication with good overall patient comfort at discharge, 7 days and 30 days follow-up.
Conclusions
In this first clinical experience, the SiteSeal® VCD achieved safe and efficient hemostasis, allowed for earlier ambulation and faster discharge compared to manual compression.
Keywords
Introduction
Approximately 7 million invasive cardiovascular procedures are performed worldwide each year, 1 and this number is expected to increase with the aging population. The modified Seldinger technique for arterial puncture and sheath insertion has become the standard method for invasive cardiovascular procedures. 2 Most of these procedures are performed via femoral arterial access (FA). 3 Risks associated with FA include access site bleeding and major vascular complications, which are associated with a risk of subsequent morbidity, mortality, and increased cost.4,5 Effective arterial hemostasis techniques are essential to improve patient comfort and reduce morbidity and mortality.
Manual compression has been considered the traditional “gold standard” technique to achieve closure of the percutaneous arteriotomy site. Most sheath removal protocols require 15–30 min of firm pressure to be applied to the access site after sheath removal depending on sheath size, followed by bed rest for 4–6 h. This process often results in significant patient discomfort, and delays the time to discharge for diagnostic procedures.6,7 There is also variability in the skill and experience of the technician holding pressure, which can affect the safety and effectiveness of this approach.
Vascular closure devices (VCDs) are a well-accepted alternative to manual compression after cardiac catheterization. While VCDs have the potential to increase patient satisfaction by improving time to hemostasis, ambulation and discharge,8–13 they have not been shown to reduce the risk of major groin complications.14–20 Another concern with the use of VCDs is that most commercially available devices leave some foreign material behind when the procedure is complete, either in the intravascular or extravascular compartment at the arteriotomy site. These concerns have hindered the even wider adoption of VCDs for achieving hemostasis after invasive cardiac procedures.
The American Heart Association published a scientific statement on arteriotomy closure devices for cardiovascular procedures in 2010. 2 It recommended caution in the use of these devices in some patient populations, while recognizing their role in improving patient comfort. The writing group recommended not using VCDs routinely for the specific purpose of reducing vascular complications in patients undergoing invasive cardiovascular procedures via the FA approach. 1
The “ideal” VCD would be one that would provide prompt and consistent hemostasis, improve patient comfort and satisfaction, and reduce complications without leaving a foreign body within the arteriotomy site. This study was designed to evaluate the safety and efficacy of the Wound Care 360° SiteSeal® (SiteSeal®) VCD. This is a first clinical experience with this new VCD.
Methods
This is a prospective case control single center study, performed at the University of Kansas Medical Center. The institutional research review committees and the human subject research committee approved the study.
Primary efficacy objectives of the study are SiteSeal® device (device is manufactured by EnsiteVascular) deployment success (defined as the ability to deploy the delivery system, deliver the powder, and achieve hemostasis at the femoral artery site), time to hemostasis (defined as the time from placement of SiteSeal® to complete cessation of arterial bleeding), time to ambulation (defined as the time from leaving the catheterization lab to walking), and time to discharge (defined as the time from SiteSeal® deployment or beginning of manual compression to discharge from the facility). Primary safety objectives of the study were assessment of vascular complications (major and minor) prior to leaving the catheterization lab and at 24 h including composite of major vascular complications (defined as device failure, TIMI major bleeding, local infection) and composite of minor vascular complications (defined as need for additional measures to achieve hemostasis like manual pressure, Femostop® use, hematoma >2 cm, analgesic use, femoral neuropathy), patient discomfort at discharge and at 24 h post procedure (1-10 scale with 1 being no pain to 10 being intense pain) and overall patient satisfaction at 7 days and 30 days.
Patients undergoing diagnostic cardiac catheterization via FA were screened for inclusion and exclusion criteria (Table 1). A total of 40 patients were enrolled in the study and randomly allocated to two groups based on methodology for achieving hemostasis (manual compression group or SiteSeal® device group. Twenty patients were enrolled in each group. All subjects gave written informed consent to participate in the study. Demographic data, clinical variables including procedure duration, post procedure monitoring, and outcomes were measured during the hospital stay. All patients were examined and evaluated every 15 min for hemostasis and bleeding complications. The patients receiving SiteSeal® device were also evaluated for comfort level based on a pain scale (1-10 scale with 1 being no pain to 10 being intense pain). A vascular ultrasound was performed in patients who received SiteSeal® device before discharge to assess potential complications, such as hematoma, venous clot formation, arteriovenous fistula, or femoral artery pseudoaneurysm. Clinical follow up was arranged at 7 days and 30 days.
Inclusion and exclusion criteria.
Device and deployment description
Following the diagnostic procedure, a femoral angiogram was performed, confirming that the access point was within the common FA, above the bifurcation of the superficial FA and profunda femoris, and below the inguinal ligament. The device was then deployed.
Device deployment
SiteSeal® is an external pressure device that applies a constant high pressure to the access site but also has a built in “shock absorber” (i.e. the springs) to dampen pressure fluctuation. The SiteSeal® device includes suture material, hemostasis BioSeal® powder with a powder containment device, the SiteSeal® and cover as well as three pieces of clear adhesive film. Deployment of the SiteSeal® is as follows (Supplemental material—Online Video 1): a Z-stitch is placed through the skin into the soft tissue alongside the catheter sheath below and above the access tract (Figures 1 and 2(a) and (b)). The powder containment device is placed over the site and powder is applied over the suture entry site and around the sheath to absorb any exudate. The stitch is tightened to approximate and invert the skin (Figure 2(c)). The skin over the insertion tract inverts and applies pressure over the tract while pulling powder down into the groove. A half-knot holds the inverted skin in place. The device is aligned with the inverted skin, pressed down firmly over the powder, the sheath is pulled, and then the suture ends are tied tightly to the device (Figure 2(d) and (e)). The device has a spring-loaded cross bar that is in a cocked position as the device is tied to the skin. The cross bar is rotated 90°, releasing the springs and putting additional pressure over the insertion site, the tract and the access site. A slightly curved “roof” is placed over the tied-down device, and three pieces of clear adhesive film are sequentially placed on the roof and pulled down tightly before adhering to the skin (Figure 2(f)). The films stabilize the device in the N/S and E/W directions. It is recommended that for 6 F sheaths the device be in place for 60 min.
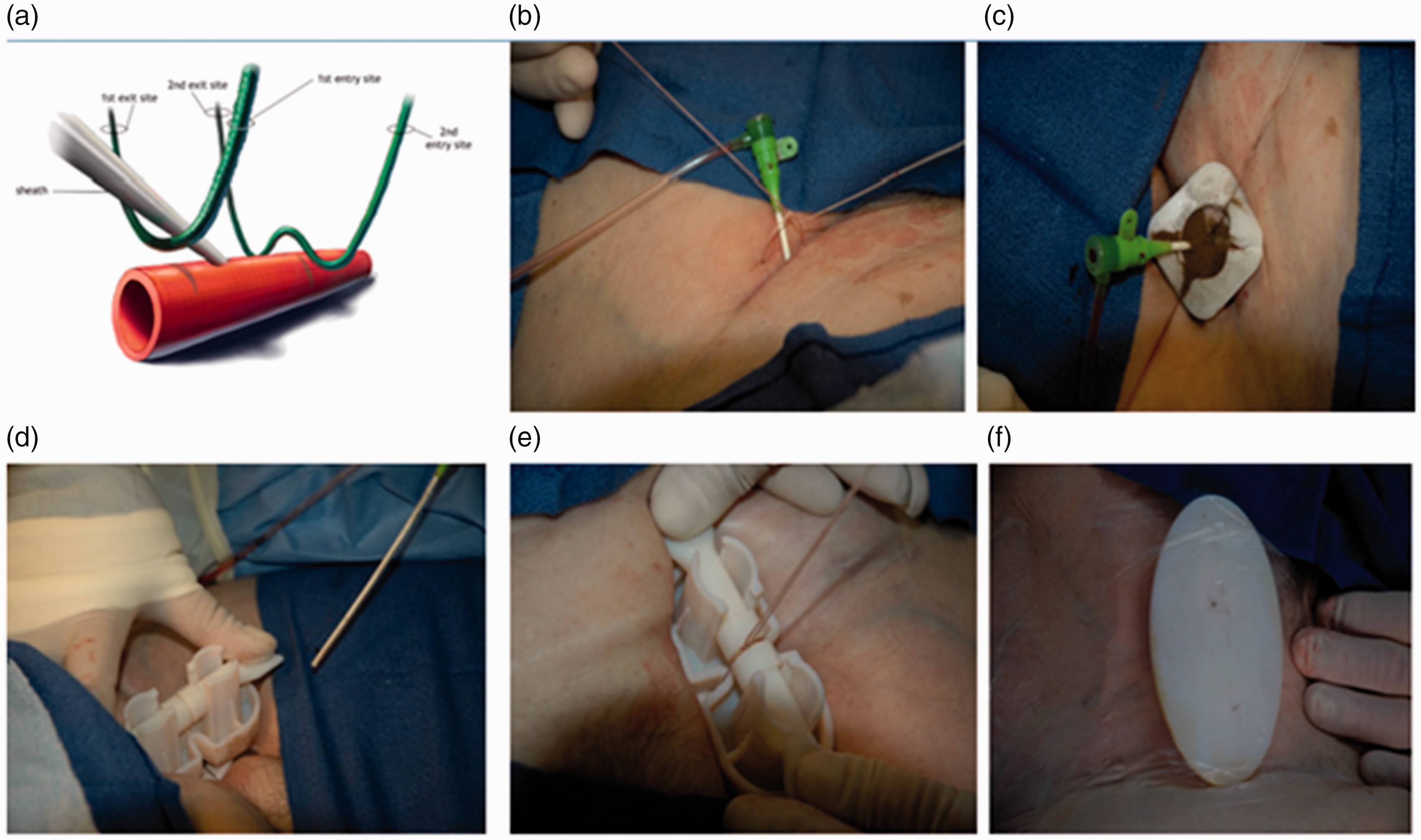
(a) 3D image showing intended Z-Stitch placement in relation to the vessel and sheath; (b) The Z stitch is initially placed and then a half knot is placed converting Z stitch to an X; (c) The suture is pulled tight, closing the X, inverting the skin and pulling powder into the tract. (d) The device is centered over the arteriotomy site and then the sheath is removed. Pressure is held by upward force of the first half knot and downward pressure on the device. (e) The device is pushed into the skin and a securing knot is completed, securing, and immobilizing the device. (f) The roof is placed over the device (Anterior view). The adhesive sheet is pulled tight over the roof maintaining stability.
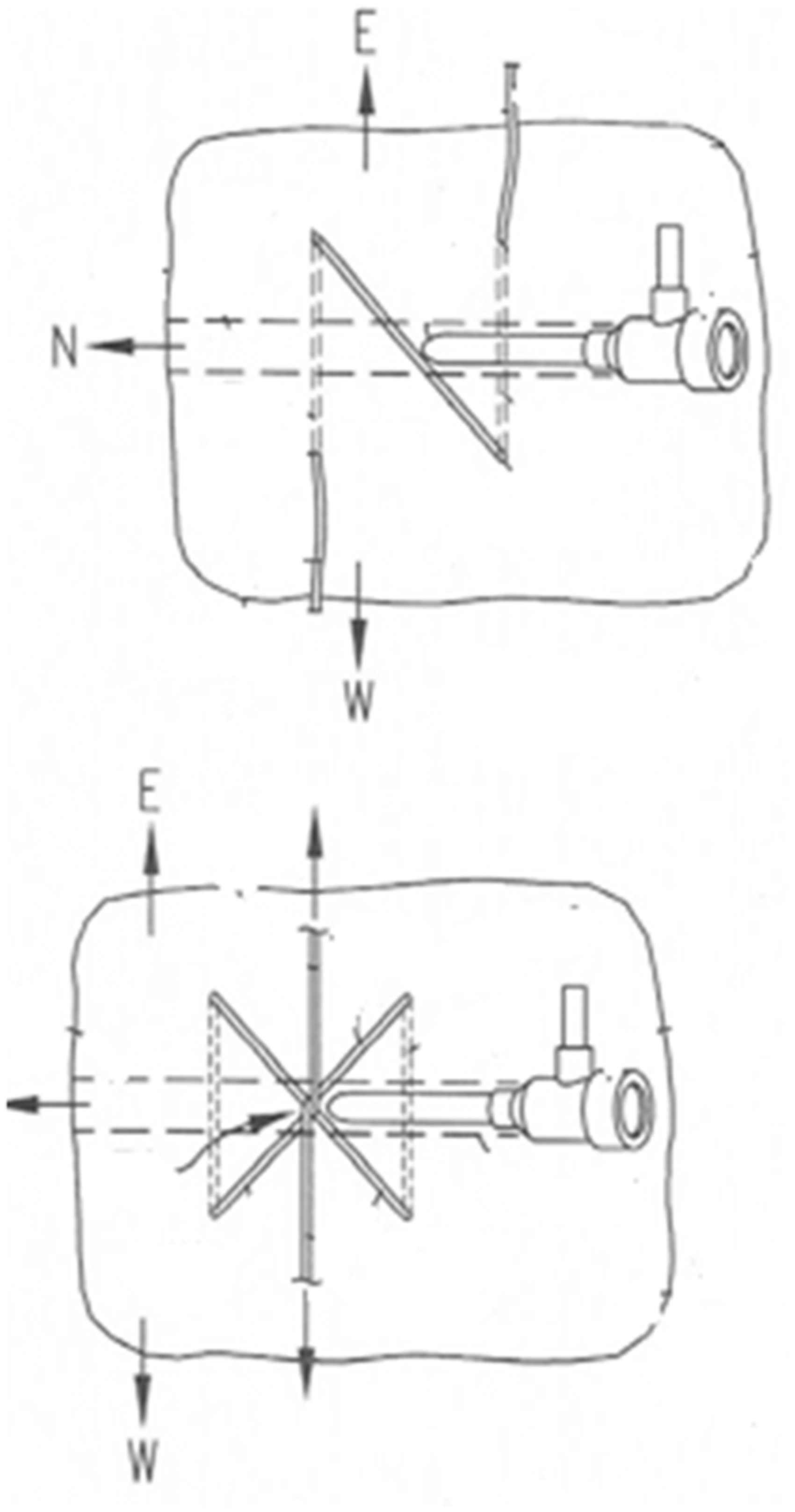
Top picture depicts Z-Stitch in place, bottom shows the Z-Stitch being tied, and pulling the skin together towards the arteriotomy site.
The patient then stays supine for 60 min, though the head can be elevated up to a 30° angulation immediately. At the conclusion of the 60-min rest period, the adhesive strips are removed. The sutures above the first knot are then cut, and the device is removed. Finally, the Z-stitch is removed from the site. Excess powder is patted onto the suture holes and insertion site as needed to absorb exudate. The patient can then ambulate.
Action of the Z-Stitch
Site suturing is used to close the access tract after removal of the sheath that has been placed through the skin into the vessel. The arteriotomy itself is closed indirectly by approximating the soft tissue above the arteriotomy with a Z-stitch. For the SiteSeal, the procedure involves a suture creating two loops under the skin perpendicular to the vessel and sheath. Above the skin the sutures create a “Z” (Z stitch) before the sutures are tied, and create an “X” after tying. The sutures are then pulled tight to purse-string the skin and tissue together, creating an inversion in the tissue beneath the knot in the sutures. This action puts pressure over the hole in the vessel, stopping the bleeding. The role of the suture is to approximate the soft tissue on either side of the puncture to make a wide ellipse narrow (Figure 3). To accommodate the increased force placed upon the suture material the SiteSeal kit includes an Ethicon Coated VICRYL (polygalactin 910) suture.
Action of Z stich.
Action of the powder
BioSeal® powder is an FDA approved topical powder made of a hydrophilic polymer and potassium ferrate. The mechanism of action is a simultaneous two-step action whereby the hydrophilic polymer rapidly dehydrates the blood and absorbs exudate while the potassium ferrate agglomerates the blood proteins, independent of clotting cascade, to create a seal or physical barrier over an access site to keep it dry and intact.
Action of the SiteSeal® device
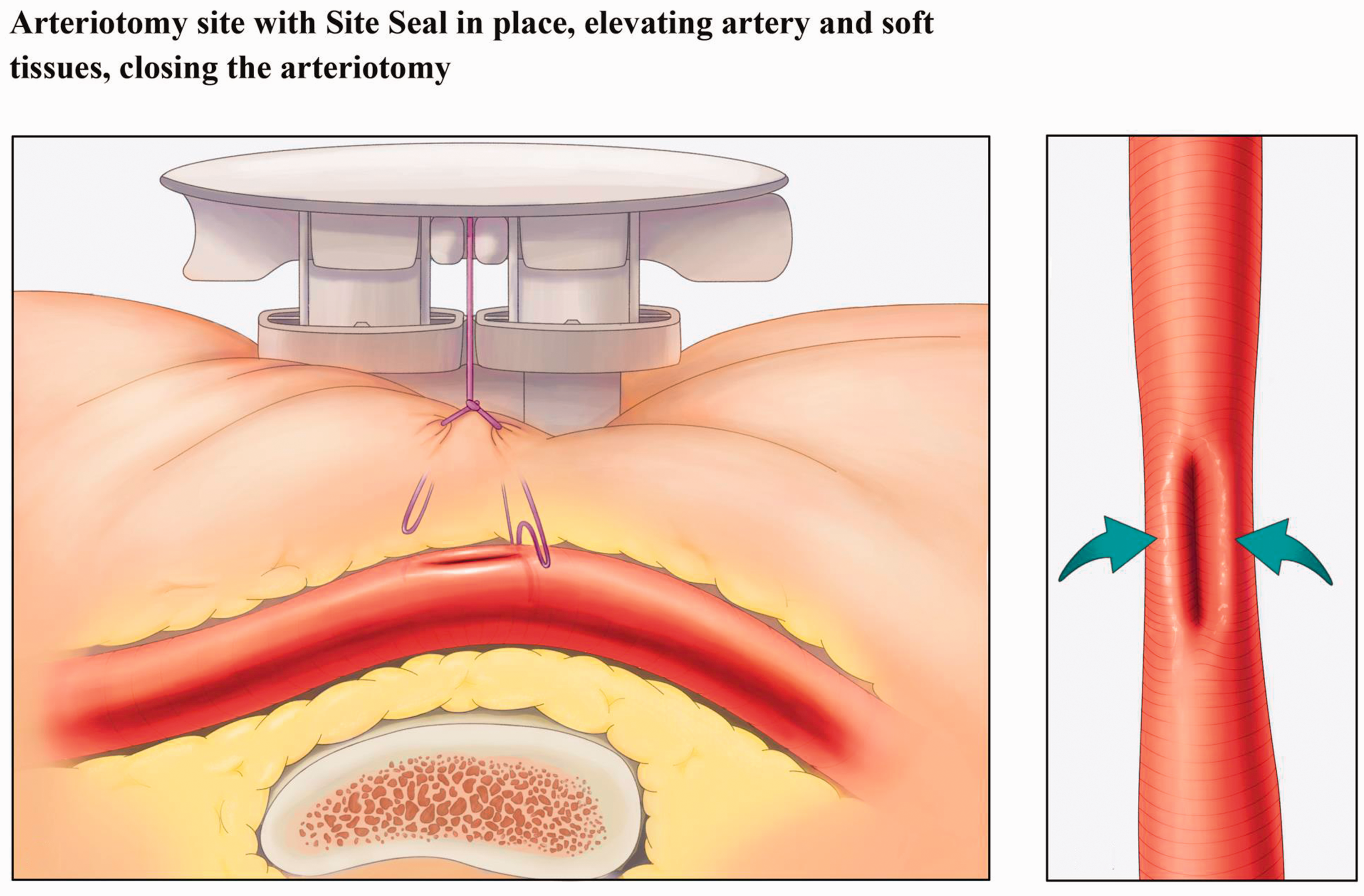
The SiteSeal device is pressed into the soft tissue above the arteriotomy, and the suture ends are tied tightly around the device crossbar (retainer). The retainer is rotated 90° to release the springs. Each spring provides ∼12 pounds force (∼24 total pounds force) to the arteriotomy site.
The SiteSeal® device reduces variation in the constrained vertical plane passing through the puncture site down to the opposite side of the vessel. The device simultaneously increases variation in the unconstrained, un-punctured horizontal plane as the heart beats. This has the subtle effect of reducing flexing of the approximated puncture site as it forms a mature clot. The SiteSeal device skin contact surface is an asymmetric “T”. The cross of the T presses across the intact vessel upstream of the puncture site to reduce downstream blood pressure. The length of the T presses lightly along the vessel on either side of the puncture site (Figure 4).
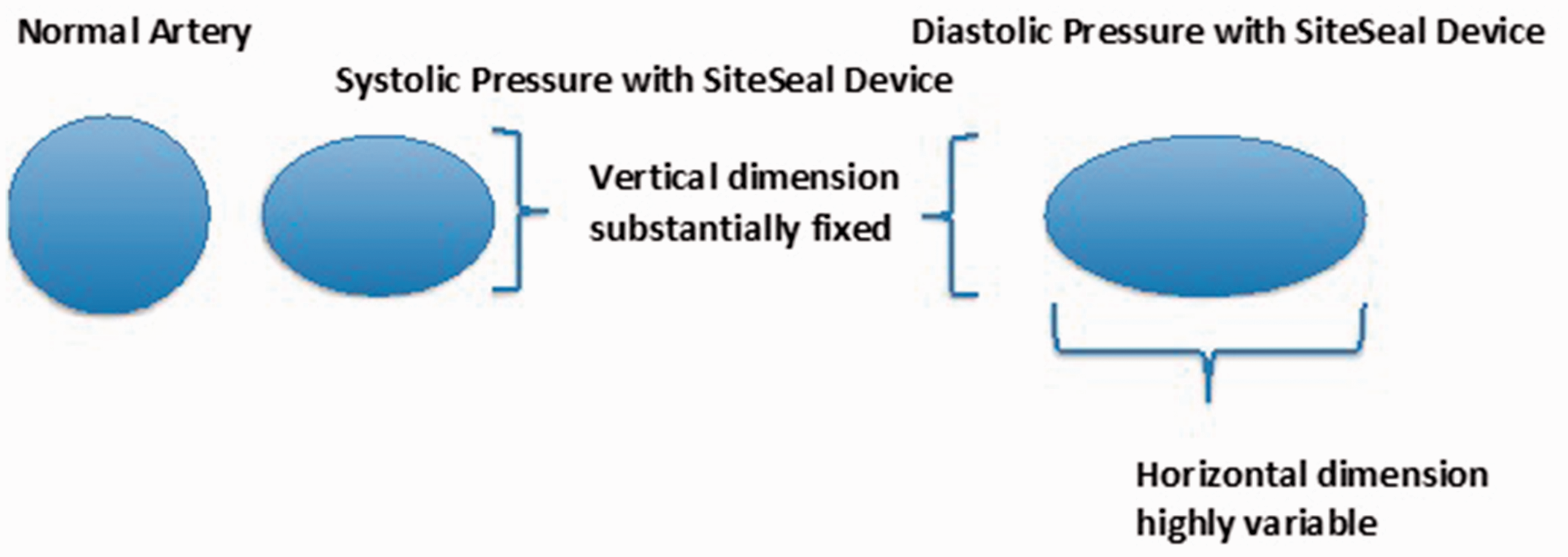
Action of SiteSeal® device.
Action of the adhesive strips
With conventional manual compression, pressure on the access site is released all at once when the fingers are removed. Mechanistically, this causes the pressure-induced horizontal oval-shaped vessel to become round and the immature clot is squeezed on both sides with every heartbeat and with any ambulation movement. The effect is exaggerated with larger French size sheaths. Larger diameter clots have increased cross-sectional bending moments, resulting in failure of immature clots. In most cases, patients are advised to lie still for 4–6 h to let the clot mature. SiteSeal® allows the clot to mature while pressure on the site is held invariant and the cross-sectional bending moment is small. The adhesive strip stabilizes the impressed device by adhering to both sides of the thigh. The strip pulls up on the thigh’s soft side tissue as it simultaneously pushes down on the device. The roof of the device, the curvature of the thigh and the adhesive strip create a “triangle”. There is a vertical upward force vector on the thigh skin and a horizontal vector into the thigh on both sides. In combination with the Z-stitch, the horizontal vectors force the vessel into a vertical narrow cross section.
Statistical analysis
Statistical analysis was performed using the statistical program for social sciences (version 19.0 SPSS Inc., Chicago, Illinois). Data was plotted (e.g. histograms and spaghetti plots linking variables) to examine for potential outliers and for the necessity of transformation prior to analysis. Continuous variables are expressed as mean ± standard deviation. For categorical variables, we used proportions, for overall and subgroups. Chi-square test was used to find association between categorical variables. Fisher exact test was used where appropriate. P value less than 0.05 was considered as statistical significant.
Results
Baseline characteristics
A total of 40 patients were enrolled in the study and divided in to two groups to receive either SiteSeal® device or manual compression (20 patients in each group). Study data points were collected on all patients except one patient in the manual compression group who did not have hemostasis and ambulation timings documented in the medical chart. He was discharged uneventfully but was not included in the results analysis, though no complications occurred at discharge or on follow up. There were no differences between the two groups in baseline characteristics (Table 2). Both groups were predominantly male Caucasians. Notably, a majority of the study patients were obese. Both groups were similar in terms of co-morbidities and cardiovascular diagnoses as assessed by mean CHADS2 score. There was no significant difference in antiplatelet and anticoagulant therapy use between the groups.
Baseline characteristics of SiteSeal® and manual compression groups.

Data are expressed as mean ± SD or as number (percentage).
BMI: Body mass index; COPD: chronic obstructive pulmonary diseases; ESRD: end stage renal disease; OSA: obstructive sleep apnea.
Procedural characteristics
All patients underwent diagnostic cardiac catheterization via FA. The right common FA was accessed in all patients in manual group and in 19 of the SiteSeal® group (left FA was accessed in one SiteSeal® patient). Six French sheaths (Terumo Pinnacle®) were used in all patients. The SiteSeal® was deployed successfully in all 20 patients in the cardiac catheterization laboratory after completion of procedure. Manual compression to achieve hemostasis was performed in the recovery area per standard protocol by a dedicated sheath management team.
Primary efficacy endpoints
SiteSeal® device deployment was successful in all patients. The procedural characteristics of the two groups are described in Table 3. Patients in SiteSeal® group achieved hemostasis in significantly shorter time as compared to manual compression group (4 ± 2.4 vs. 19 ± 2.4 min, P < 0.001) (Table 3 and Figure 5(a)). Time from hemostasis to ambulation was significantly shorter in the SiteSeal® group (95 ± 44 vs. 388 ± 63 min, P <0.001) (Table 3 and Figure 5(b)). Time from SiteSeal® deployment or manual compression to discharge was significantly shorter in SiteSeal group (4.7 ± 1.1 vs. 8.9 ± 4.8 h, P = 0.001) (Table 3 and Figure 5(c)). All patients in the SiteSeal® group had an access site ultrasound performed, delaying their discharge (included).
Procedural characteristics of SiteSeal® and manual compression groups.
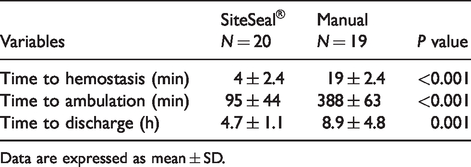
Data are expressed as mean ± SD.
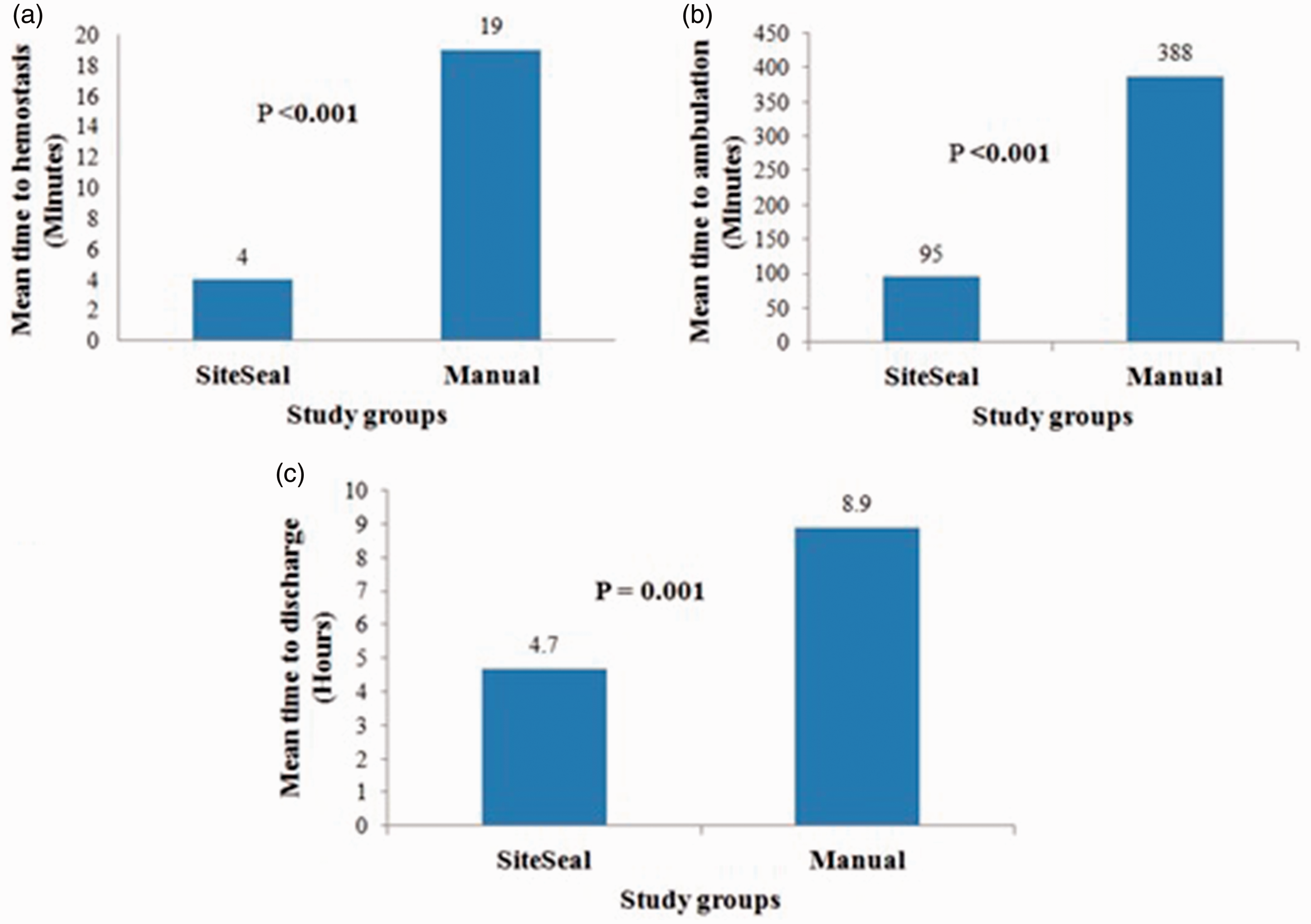
Comparative analysis of efficacy of hemostasis achieved in different study groups. (a) Mean time to hemostasis (minutes); (b) mean time to ambulation (minutes); (c) mean time to discharge (hours).
Primary safety endpoints
Hemostasis was achieved in the majority of patients (95%) after device deployment. Minimal discomfort (2–4/10 on scale) was reported by three patients due to pressure related to device deployment in the immediate post procedure period. Significant discomfort (8/10 on scale) was reported by one patient, which was not just at the groin site but was diffuse and related to generalized discomfort in relation to known diagnosis of fibromyalgia. The majority of patients in device group (80%) reported good comfort level (0/10 on scale) post procedure. One patient had the device removed due to misinterpretation of surrounding soft tissue as hematoma by nursing staff, just prior to time to device removal. Subsequent evaluation by physician revealed no hematoma or clinical complication but patient was crossed over to the manual compression group for additional bed rest from a safety standpoint, per protocol. One patient in the device group was readmitted 48 h after the discharge with groin hematoma > 6 cm in size, which was confirmed on repeat vascular ultrasound. No retroperitoneal bleeding was identified. There was no clinical or vascular imaging evidence of minor or major complications in this patient prior to discharge from the hospital. The patient was monitored and managed conservatively without any need for surgical intervention. There was no other clinical evidence of major or minor complication at 7 days and 30 days follow up in device group.
Vascular ultrasound
Vascular duplex ultrasound of the groin was performed in all patients receiving SiteSeal® to assess for vascular complication prior to discharge. None of the patients had evidence of deep venous thrombosis, hematoma, arteriovenous fistula, FA pseudoaneurysm, or any other vascular complications.
Discussion
The study reports the first clinical experience with the SiteSeal® VCD after transfemoral cardiac catheterization. The results of this study support our hypothesis of the SiteSeal® device achieving earlier effective hemostasis and decreased time to ambulation when compared to manual compression after diagnostic cardiac catheterization. The time from hemostasis to discharge was also decreased with the SiteSeal® device compared to manual compression. These findings are consistent with the prior clinical studies suggesting that VCDs may play an increasing role in the economics of medicine, allowing for earlier discharge, and thus decreasing the staffing needs for monitoring, as well as increasing turnover rate in post procedure recovery areas.21,22
The SiteSeal® device was deployed successfully in all patients without the need for prolonged bed rest, allowing for earlier ambulation. The device deployment was associated with good overall patient comfort level at discharge as well as at 7- and 30-day follow up. There was no significant difference in the incidence of minor and major clinical and vascular complications between the SiteSeal device and manual compression. One case of device failure occurred <24 h post device deployment due to misinterpretation of surrounding soft tissue as hematoma by nursing staff, and could have been avoided. One major complication in the device group occurred >24 h after discharge when the patient was readmitted for a groin hematoma (>6 cm), possibly related to increased straining or persistent oozing from arteriotomy site. This patient was conservatively managed without surgical intervention and has had no sequelae on follow up. Overall, the safety endpoint of device use was supplemented by vascular ultrasound with no evidence of DVT, hematoma, arteriovenous fistula, femoral artery pseudoaneurysm, or other vascular complications.
VCDs have emerged as an effective alternative to traditional manual compression after cardiac catheterization since their introduction in the 1990s. These devices can be loosely grouped into two categories: passive closure devices, such as external clamps/tamping devices which either mimic manual compression, or pro-coagulant patches or sealants which aid in sealing the arteriotomy tract; and active closure devices, such as suture based closure, clips, or collagen-plug mediated devices, all of which leave material behind when the procedure is complete. These devices have the potential to reduce the time to hemostasis, facilitate early patient mobilization, decrease hospital length of stay, and improve patient satisfaction.8–13 While VCDs are convenient to both the patient and the healthcare systems, their use has not become the standard of care for invasive cardiac procedures, 23 largely because the data on efficacy and safety of these devices is controversial with variable results observed in multiple meta-analyses and prospective randomized and nonrandomized trials. Some studies have shown that these devices are as efficacious as manual compression,24,25 whereas others have shown superiority of these devices compared with manual compression for both efficacy 26 and cost minimization despite the upfront cost of these devices, largely based on a lower complication rate with VCDs. 22 However, other studies have expressed concern about increased risk of complications with these devices.14–20 There is also apprehension about excess vascular inflammation and scarring associated with VCDs, because most active devices leave material behind when the procedure is complete, either in intravascular or extravascular component at arteriotomy site.
Following the concept of the “ideal” closure device as stated above, we present the first clinical experience with SiteSeal® VCD, which was able to provide prompt hemostasis, achieve excellent patient comfort and satisfaction, and has potential to reduce complications, which are associated with other devices which leave a foreign body within the arteriotomy site.
Limitations
We evaluated the efficacy and safety of the SiteSeal® device for hemostasis after transfemoral cardiac catheterization procedures. These results should not be extrapolated to those undergoing interventional procedures with use of antiplatelet and anticoagulant therapies. Since all subjects had 6 F sheaths used these results may not apply to other sheath sizes. The device was not evaluated for use in presence of significant common femoral artery atherosclerosis or calcification, thus the findings of this study may not be applicable to those patients.
Conclusion
In this first clinical experience with SiteSeal® device, among the patients undergoing diagnostic transfemoral cardiac catheterization, the SiteSeal® device is effective at achieving efficient hemostasis, early ambulation time and faster discharge when compared to manual compression. The SiteSeal® deployment is safe with no clinical or ultrasound evidence of significant major or minor vascular complication at discharge and had good overall patient comfort at discharge and 30 days follow up. The key feature of SiteSeal® device is that it achieves effective hemostasis without leaving the foreign material either in the intravascular or extravascular compartment at the arteriotomy site.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Matthew B Earnest has consulting agreement with St. Jude Medical. Suresh Sharma, Nilay Patel, Vinodh Jeevanantham, and Kamal Gupta declare no conflicts of interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.