
Abstract
Objective
In the last decades, life expectancy has increased worldwide considerably. Traditionally, very elderly patients have been considered too frail to undergo major vascular interventions. Considering that abdominal aortic aneurysm is an age-related disease, there is an increasing need of a correct management of the disease even in nonagenarians, but data are still scarce. The purpose of this single-centre study is to report early and mid-term outcomes of all-comer abdominal aortic aneurysm patients in their 10th decades of age.
Methods
A retrospective review of our prospectively maintained database identified a total of 33 patients aged ≥ 90 presenting with abdominal aortic aneurysm between 2014 and 2019. Elective and emergency repairs were both considered. Early technical success and mortality rate at 30 days were considered as primary outcomes. Mid-term clinical success was reported, and overall survival, freedom from aneurysm-related death, re-interventions and endoleaks were estimated with the Kaplan–Meier method, stratified for elective of emergency repair and type of treatment.
Results
The mean age was 91.7 (range 90–96), and 63.6% were male. Mean abdominal aortic aneurysm diameter was 67.4 ± 16.8 mm. Sixteen patients were admitted for rupture abdominal aortic aneurysm: three untreated, five underwent open and seven underwent endovascular aneurysm repair (EVAR), with an early mortality rate of 100, 100 and 42.8%, respectively. Eighteen (60%) patients were asymptomatic, and all underwent elective EVAR, with an early mortality rate of 0%. At one-month follow-up, clinical success was 84% in EVAR group. At a median follow-up of 22.4 ± 14.5 months, no abdominal aortic aneurysm-related death was registered. Freedom from all cause of mortality was 77.3, 59.4 and 40.7% at one, two and three years. Freedom from endoleaks was 95.4% at one month and 61.7% at one and three years. Freedom from reintervention was 85.8% at three years.
Conclusion
Elective EVAR in nonagenarians is associated with acceptable early and mid-term outcomes. Age by itself should not be considered an exclusion criterion for treatment.
Introduction
Since the early 19th century, life expectancy started to increase worldwide and, in particular, in the early industrialized countries, mainly as a consequence of the developments in medicine. In Europe, life expectancy was estimated to be 80.9 years in 2017, reaching 83.5 years for women and 78.3 years for men, a difference of 5.2 years. 1 In United States, people over 80 years are going to increase from 3.4 to 9 million by 2030, and by 2050, there will be an estimated 20.9 million people over the age of 85. 2 The same trend has been predicted for European population, where the number of octogenarians is going to increase, reaching the number of 61.4 million in 2060. 3
Considering that abdominal aortic aneurysm (AAA) is an age-related disease, its prevalence has increased as well, leading to the necessity to manage the disease even in very elderly and frail patients. The negative impact of advanced aging on mortality in open AAA repair is well-known, and it is mainly due to the limited functional reserve of elderly patients, making endovascular aneurysm repair (EVAR) an attractive less invasive alternative. 4 Still, many very elderly patients miss a screening in the asymptomatic phase of the disease and are admitted with symptoms, leaving the vascular surgeon with the challenging choice whether to treat or not.
Previous studies have focused on the treatment of AAA in octogenarians,5–7 while data in nonagenarians is quite scarce, and the debate on the convenience of treatment is still open.
The purpose of this single-centre retrospective study is to report early and mid-term outcomes of a series of all-comer AAA patients in their 10th decades of age, with respect to the elective of emergency clinical condition at presentation and to the type of treatment received.
Methods
A retrospective analysis of all the available records of our hospital was performed to obtain data of all-comer patients aged 90 years or older with a diagnosis of AAA between January 2014 and December 2019. Patients’ demographics, intraoperative data and post-operative outcomes were collected through hospital charts. Coronary artery disease (CAD), hypertension, diabetes mellitus (DM), chronic obstructive pulmonary disease (COPD), renal disease (chronic renal insufficiency defined by serum creatinine >1.2 mg/dl), smoking history (any current or past regular use of tobacco), congestive heart failure (CHF), history of cerebrovascular events (stroke and/or transient ischaemic attacks), history of cancer (any current or past incidence if malignancy), dyslipidemia and atrial fibrillation (AF) were taken in account as comorbidities.
For patients admitted in emergency setting for AAA rupture with intra- or immediate postoperative death, anamnestic data were collected reviewing previous hospital admissions and general practitioner interviews.
Pre-operative aneurysm size and anatomic characteristics (aortic neck length and angulation, iliac arteries diameter, calcification and tortuosity) were determined by computed tomography angiography (CTA). 8
EVAR was always considered as a first-line treatment. In emergency, anatomical suitability was analysed by an expert endovascular surgeon, although in case of severe hemodynamic instability and impossibility to perform CTA, open repair (OR) was performed. Surgery procedures were achieved according to our department standards. Open surgical approach was through a median laparotomy in all cases, considering supra-renal cross-clamping in case of inadequate infrarenal neck and choosing a tube or bifurcated grafts on the patients’ anatomic features.
In endovascular cases, stent graft deployment was made through femoral accesses (surgical cutdown and/or percutaneous) under local or loco-regional anaesthesia. The choice of the device was based on anatomical patient features, comorbidities and surgeon’s preference. In case of emergency setting, the endografts used were based on their prompt availability.
Post-operative follow-up protocol included duplex ultrasound (DUS) examination at 1–6 and 12 months and annually thereafter, while CTA was typically performed only in the early post-operative period (within the first three months) or in case of suspected findings at DUS exams.
The study protocol and informed consent were approved by the Institutional Review Board, and all subjects gave informed consent. The ethical committee of the hospital was informed of the no-experimental design of the retrospective investigation and endorsed the study.
Outcomes
According to Standard Report, 9 the following outcomes were analysed: technical success and mortality rate at 30 days, which were considered as primary outcomes. Secondary endpoints consisted of surgical graft (graft thrombosis, graft infections, haemorrhage, aorto-iliac pseudoaneurysms) and EVAR complications (endoleaks, aneurysm expansion, graft migration, AAA rupture, secondary interventions and conversion to OR) and long-term clinical success.
Technical success for EVAR cases was defined as successful deployment of endograft with secure fixation and patency, absence of type I or III endoleaks within the first 24 h.
Endoleaks, graft patency and graft migration were detected with DUS and/or CTA exams following our scheduled follow-up program. For the analysis of endoleaks, the event was considered as present from the first time that it was detected. Graft migration was defined by distal displacement of the stent graft of 10 mm or more. Graft patency was also evaluated by DUS and/or CTA exams.
Clinical success is defined as a successful deployment of the endovascular device at the intended location without death as a result of aneurysm-related treatment, type I or type III endoleaks, graft infection or thrombosis, aneurysm expansion (diameter >5 mm or volume >5%), aneurysm rupture or conversion to OR.
Renal function deterioration was defined as an elevation of serum creatinine concentration of >25% or >0.5 mg/dL (44 mmol/L) from baseline within 48 h.
Secondary interventions performed to fix or to avoid a potential complication included endovascular procedures (proximal cuff and stent implantation, distal extension implantation, catheter-based thrombolysis, iliac angioplasty, coil or glue embolization of aortic branch vessels) and surgical intervention (balloon thrombectomy, femoro-femoral bypass, conversion to OR, open or laparoscopic ligation of collaterals).
Statistical analysis
Mean (±standard deviation) and median were used to analyse continuous variables. Student’s two-tailed t-test was used when applicable, and categorical variables were compared using Fisher’s exact test. Statistical significance was considered for P value less than 0.05. Rates of freedom from overall death, aneurysm-related death, reinterventions and endoleaks were estimated with the Kaplan–Meier method. Log-rank test was used to compare life table curves.
Results
Thirty-four patients with AAA aged ≥ 90 years were admitted to our Vascular Surgery department during the study period. The mean age at the time of intervention was 91.7 ± 1.6 years (range 90–96 years), and 63.6% were male. The mean AAA diameter was 67.4 mm ± 16.8 mm (range 49–100 mm).
Three cases admitted with a diagnosis of ruptured or impending rupture AAA remained untreated because of lack of patient’s consent. All patients died within 24 h from the admission and were no longer considered in the further study analysis.
Of the remaining 30 patients, 12 (40%) were admitted in emergency setting for rupture and received OR (n = 5) and EVAR (n = 7); 18 (60%) were asymptomatic and underwent elective EVAR (Figure 1).
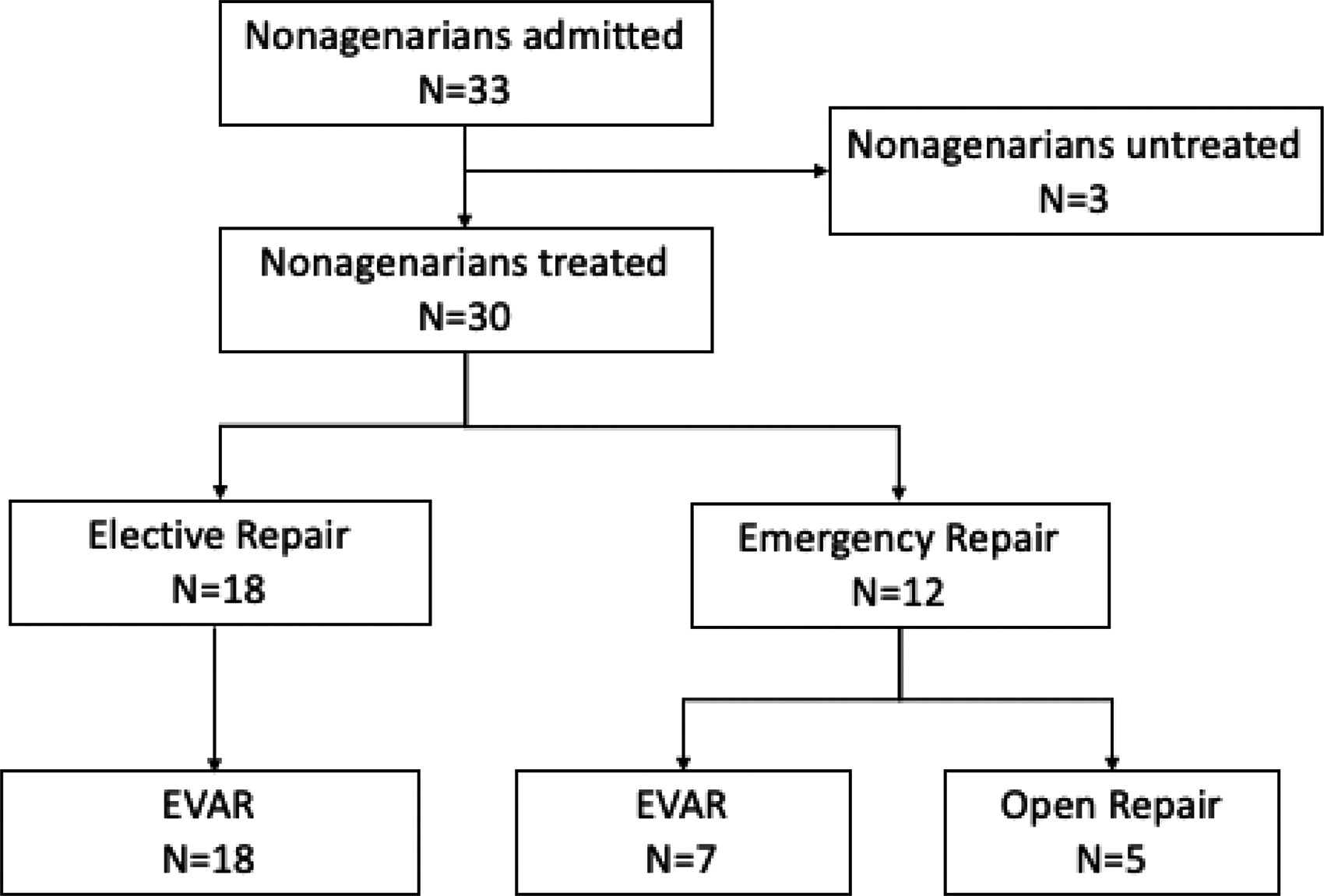
Patients’ cohort scheme.
Table 1 shows the anamnestic baseline data.
Patients’ characteristics.

Patients with emergency AAA repair
The five patients who underwent OR for ruptured AAA died of multi-organ failure (MOF) in the perioperative time, between the first and the ninth post-operative day.
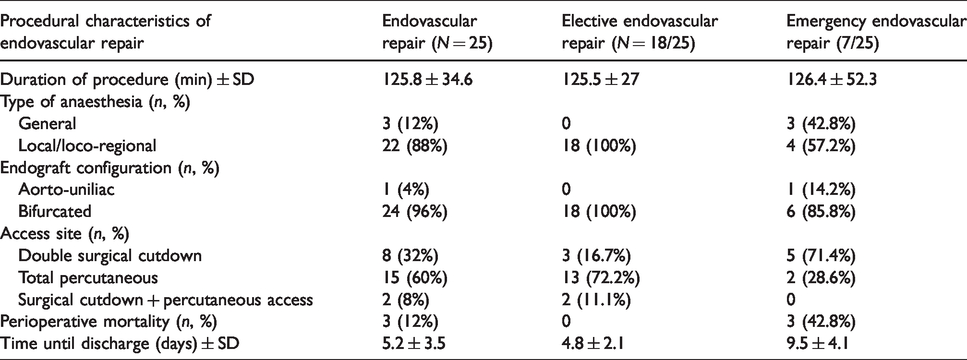
The remaining seven patients received EVAR under local or loco-regional anaesthesia. The mean procedural duration was 126.4 ± 52.3 min, and the average contrast medium used was 95 ± 15 ml. The blood loss estimation was impossible to be determined, but all emergent cases required intraoperative transfusion. Six bifurcated and one aorto-uniliac endografts were implanted (Medtronic Endurant). Endograft outside the instructions for use (IFU) were three (42.8%). All patients required intensive care unit (ICU) monitoring for the early post-operative time (36 ± 9.3 h). Mortality rate was 42.8% (n = 3 MOF). The remaining four patients were discharged after a mean hospitalization time of 9.5 ± 4.1 days (Table 2).
Procedural features of endovascular repair procedures performed.
Temporary renal function deterioration was registered in 42.8% (3/7), no acute kidney injury was registered and no haemodialysis was required post-operatively.
Patients with elective AAA repair
All patients received EVAR under local or loco-regional anaesthesia. The average procedure duration was 125.5 ± 27 min, and the average contrast medium used was 80 ± 15 ml. No intra-operative transfusion was needed. In terms of endograft configuration, the bifurcated design was chosen in all cases. A total of 27.8% (5/18) received Medtronic Endurant grafts, 55.6% (10/18) Endologix Ovation grafts, 11.1% (2/18) Bolton Treovance grafts and 5.5% (1/18) Anaconda graft.
Endografts outside the IFU were 12 (66.6%). Early technical success was 94.4% (17/18). In one case, the deployment of a Bolton Treovance stent graft was impossible due to extremely calcified iliac axis. The repair was re-scheduled two days later using a low-profile device (Ovation) with complete aneurysm exclusion at the end of the procedure. No intraoperative type 1 or 3 endoleaks were detected, and type 2 endoleaks were recorded in 11.1% of cases (2/18).
ICU monitoring was not required, no perioperative local complications were detected and the mean hospitalization time was 4.8 ± 2.1 days (Table 2).
Temporary renal function deterioration was registered in three patients (16.6%), no acute kidney injury was registered and no haemodialysis was required post-operatively.
Early outcomes
Early clinical success was 0% for OR and 84% (21/25) for EVAR (7 emergency, 18 elective repairs) because of three deaths (Emergency EVAR group) and one type 1-A endoleak that was detected during routine pre-discharge DUS (Elective EVAR group). This high-flow endoleak was promptly treated with coil embolization during the same hospitalization. As a result, assisted clinical success for EVAR was 88% (22/25).
At one-month follow-up, clinical success was 84% (21/25) in EVAR group. One death (patient admitted for impending rupture) for acute myocardial infarction (AMI) was registered on the 17th post-operatory day, when the patient was at home.
Mid-term follow-up
Follow-up was available for all survived patients after the first month (n = 22). At a median follow-up of 22 ± 14.95 months, a total of 11 patients died during follow-up, and no AAA-related deaths were registered. The population study all-cause survival was 68% at one year, 52.3 at two years and 34.8% at three years (Figure 2).
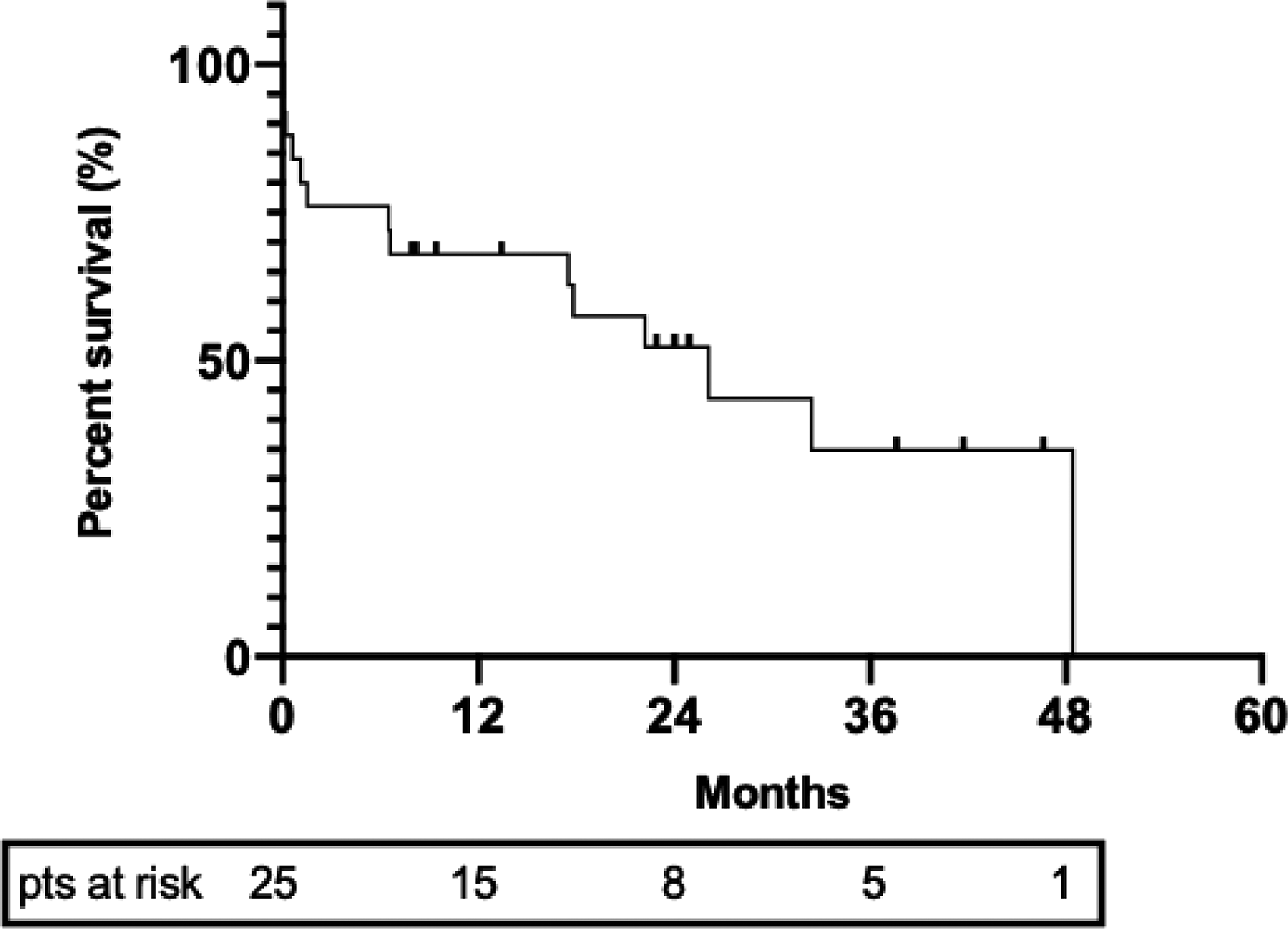
Kaplan–Meier graph represents freedom from all-cause mortality for the whole population study (30 patients).
Freedom from all-cause mortality in the EVAR-group was: 77.3% at one year, 59.4% at two years and 40.7% at three years. Subgroup analysis between elective versus rupture EVARs revealed significant differences (P = 0.03) (Figure 3).

Kaplan–Meier graph represents freedom from all-cause mortality in EVAR group with curves of subgroup analysis (elective EVAR vs. emergency EVAR.)
During the follow-up period, seven endoleaks were detected: three type 1-A and four type II endoleaks. Kaplan–Meier freedom from endoleaks is shown in Figure 4 (95.4% at one month and 61.7% at one and three years).
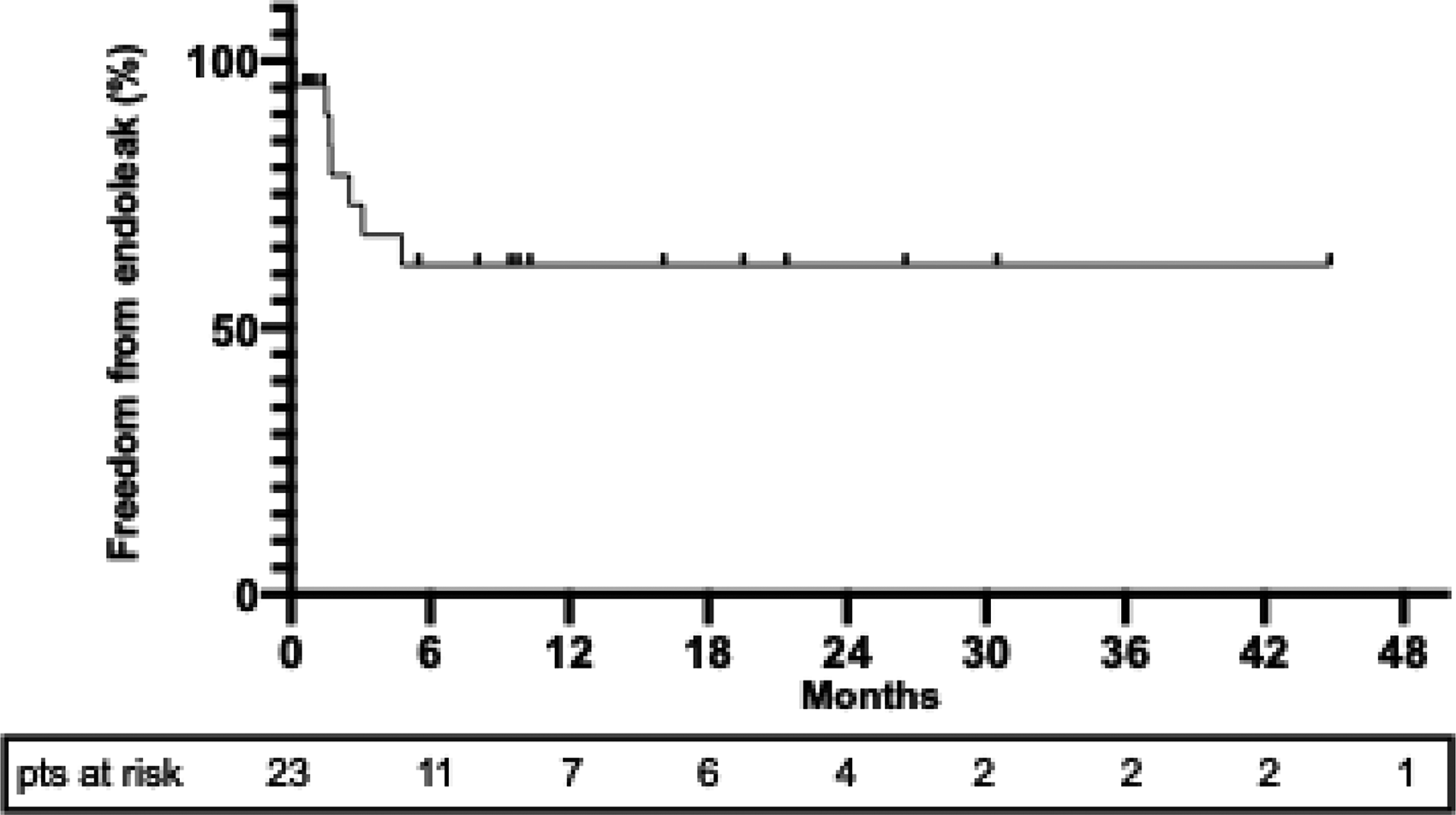
Kaplan–Meier graph represents freedom from endoleaks in EVAR group.
Three re-interventions for type 1-A correction were performed during follow-up: two cases of cuff extension and one case of coil embolization. Freedom from re-intervention was 85.8% at one and three years. Subgroup analysis between elective versus emergency EVARs showed no statistically significant differences between curves (P = 0.07) (Figure 5).

Kaplan–Meier graph represents freedom from secondary intervention.
There were no significant differences in terms of early and mid-term complications between inside versus outside IFU procedures.
Discussion
High-income nations are experiencing a gradually increasing of life expectancy with significant critical issues in terms of incidence and prevalence of acute and chronic cardiovascular disease. This means that the occurrence of AAA in elderly patients will be more and more frequent in the future, and the decision of when and how to treat is more and more challenging.
A systematic literature search revealed acceptable results of EVAR in nonagenarians with no intraoperative mortality, a perioperative medical or surgical complication rate of 22%, a 30-day mortality of 5% and survival rates at one, three and five years of 82, 56 and 17%, respectively. 10
Of note, a patient’s selection had been performed in most of the articles included in this systemic review. This led to the conclusion that given the typical life expectancy, careful consideration should be given to individual cases before undertaking EVAR in the nonagenarian.
Our experience seems to partially disagree with this conclusion. Although we agree that the present clinical significance of treating nonagenarians with AAA is debatable, our data support a policy of endovascular treatment for all-comer nonagenarian patients, with no one excluded to treatment just because of the age. To deny treatment in such elderly population or to miss a diagnosis of asymptomatic AAA led the patient to future scenario with very poor outcome. Even with our policy of treating all-comer nonagenarian AAA patients, the rate of symptomatic versus asymptomatic clinical presentations is surprisingly high (47%, 16 vs. 18). Considering that 4 out of 16 symptomatic patients denied any treatment and died within 24 h and that the mortality rate in the remaining 12 cases was tremendously high, we believe that the best consideration to give to individual nonagenarians cases is to offer EVAR as much as possible and as early as possible.
Of course, such a policy should take into consideration that very elderly patients present with challenging anatomical features such as diffuse calcifications, small arteries, huge aneurysm and short or angulated aortic neck. A large experience in endovascular techniques and the availability of a wide range of materials may help to overcome these anatomical situations, which have been considered exclusion criteria for EVAR in previous experiences. 11 In our experience, the use of ultra-low-profile devices with a new concept of proximal sealing made often possible EVAR even in the presence of challenging anatomy, such as short or conical neck or neck with a large amount of thrombus.12,13
Contrast-induced nephropathy is a well-known reported complication after EVAR especially in the elderly population strictly related to the amount of contrast used. 14 A careful pre-operative planning of EVAR procedures, including choice of device diameters and lengths and projection for correct angiographic visualization of vessels are the key factors for reducing the amount of contrast in our experience (in emergency mean 95 ± 15 ml, in elective mean 80 ± 15 ml), minimizing the risk of renal failure in this frail population. Of note, medium use of contrast during EVAR has been reported somehow higher (median contrast medium used 120 ml). 15
In our experience, both emergency and elective EVARs were often performed with a percutaneous approach (60%) and under local or loco-regional anaesthesia (88%). Such intraoperative management impacted positively on the need of ICU stay (mean of 36 h for emergency repair, no need for elective repair), on the post-operative complication rate (no IMA) and on the length of hospitalization (mean 4.8 ± 2.1 for elective and 9.5 ± 4.1 for emergency repairs).
In our report, elective repair was characterized by a very high clinical and technical success, with data comparable to younger cohort of patients. In emergency setting, EVAR represented a life-saving procedure in more than half of cases (58%) comparing much better than emergency OR (survival 0%), confirming how the adoption of EVAR as a first policy in non-elective setting is profitable in terms of incidence of in-hospital mortality, respiratory complications, renal failure, cardiac complications and mesenteric ischaemia. 16
At mid-term follow-up, we observed no AAA-related deaths and acceptable rates of endoleaks (freedom at three years of 61.7%) and reintervention (freedom at three years of 85.8%), more or less in line with those reported for general population. 17
So, can age by itself be considered an exclusion criterion for treatment of AAA?
The role of age as predictor of poor outcome after AAA repair remains somehow debatable, especially for EVAR. An age older than 70 years has been reported as related to more complex anatomy and consequently to a higher risk of endoleaks and re-interventions.18,19 In contrast, Machado et al. 20 reported no significant statistical differences in terms of mortality and re-interventions among different age group of patients who have undergone EVAR. 20
Acceptable results after EVAR have been already reported for nonagenarians, although was noted that comorbidities may influence outcomes considerably. In particular, long-term survival was significantly decreased for patients presenting with >5 comorbidities. 21
A correct selection of nonagenarians patients may have positive effect on mid and long-term survival rate. Lee et al. 22 reported an impressive median survival of 56.2 months in nonagenarians with good/excellent preoperative status and an average number of comorbidities less than three. 22 On the other hand, higher mortality rates at 30 days (5.6%) were found if selection is not appropriate, with a substantial long-term mortality (56.3% at two years). 23
Our conviction is that excluding very elderly patients from elective EVAR may avoid any chance of future treatment. The emergency treatment for AAA rupture or impending rupture, also in high-volume centres, is burdened by high mortality especially if OR is performed.
Sometimes, decision to operate on very elderly patients depends also on ethical, economic and political aspects. This may be linked to local culture and different national healthcare system policies. In our country, the attitude is to never deny any treatment of life-threatening conditions, even in very elderly patients. So, when facing patients with AAA demanding repair, our suggestion is to offer EVAR, even with advanced techniques, in all cases irrespective of the age.
The present study has some limitations, and the primary is the retrospective, single-centre nature of the study and comparison without a contemporaneous control group. These elements, together with the relatively limited number of patients analysed, could be overcome in future population-based study with a larger cohort of patients involved. Still, we know that the cost-effectiveness EVAR procedure for nonagenarians is really controversial and that our investigation is clearly underpowered to fully address this question.
In this perspective, although we do not have any recommendations on which patients we should not operate or who are going to die because of any other conditions, we believe that our policy of treating all comers is somehow cost-effective: in our society, life expectancy is going to further increase with a contemporary growing number of very elderly individuals with good quality of life. In this perspective, in the near future, we would have to be prepared to face an increasing number of elderly patients with dangerous aneurysm with high risk of rupture. Our policy clearly aims to avoid emergency treatment for AAA rupture or impending rupture for two main reasons: high mortality rates and high costs with these events. In fact, emergency treatment, ICU stay, general medical treatment and adjunctive long-term recovering therapies (e.g. post-op physiotherapy) are burdened by significant costs.
In conclusion, our data support that the elective EVAR in nonagenarians is associated with acceptable early and mid-term outcomes and that age by itself should not be considered an exclusion criterion for treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.