
Abstract
Objectives
To compare preoperative coagulation and fibrinolysis activity and incidence of perioperative complications between patients undergoing vascular procedures for peripheral artery disease and abdominal aortic aneurysm.
Methods
This is a substudy of a prospective observational cohort study (VISION; NCT00512109) in which we recruited patients aged ≥45 years, undergoing surgery for peripheral artery disease and abdominal aortic aneurysm. Blood samples were obtained 24 h preoperatively to measure platelet count, concentrations of coagulation coagulation (fibrinogen, factor VIII, von Willebrand factor:Ristocetin cofactor, antithrombin III), fibrinolysis (dimer D, plasmin–antiplasmin complexes, tissue plasminogen activator) markers and level of soluble CD40 ligand. Incidence of myocardial infarction, stroke, and death (composite endpoint) was assessed in 30-day follow-up.
Results
The study group included 131 patients at the mean age of 68.3 years among whom reason for surgery was peripheral artery disease in 77 patients (58.8%) and abdominal aortic aneurysm in 54 patients (41.2%). Peripheral artery disease group was characterized by higher platelet count (250.5 versus 209.5 (×10 3 /µl), p = 0.001), concentrations of fibrinogen (5.4 versus 4.1 (g/l), p < 0.001), factor VIII (176.9 versus 141.9 (%), p < 0.001), von Willebrand factor:Ristocetin cofactor (188.9 versus 152.3 (%), p = 0.009), and soluble CD40 ligand (9016.0 versus 7936.6 (pg/ml), p = 0.005). The dimer D level was higher (808.0 versus 2590.5 (ng/ml), p < 0.001) in the abdominal aortic aneurysm group. Incidence of major cardiovascular events (death, myocardial infarction, stroke) within 30 days from surgery did not differ between the groups (39.0% versus 29.6%, p = 0.27).
Conclusions
The study suggests higher activation of coagulation and relatively lower fibrinolytic activity in peripheral artery disease group compared to patients undergoing surgery for abdominal aortic aneurysm without a significant difference in cardiovascular outcomes.
Keywords
Introduction
Peripheral artery disease (PAD) and abdominal aortic aneurysm (AAA) are among the leading causes of morbidity and mortality in most of the developed countries.1–3 They are associated with an increased risk for cardiovascular events and often require surgical treatment. Due to multiple factors, including advanced atherosclerosis, high rates of cardiovascular comorbidities, as well as tendency for perioperative bleeding and reperfusion injury, these procedures are classified as high-risk surgeries in the current perioperative care guidelines.4–6
Both PAD and AAA are chronic vascular diseases associated with enhanced inflammation as well as derangements in coagulation and fibrinolysis systems. 7 , 8 Interestingly, coagulation activity is associated with the clinical severity of both diseases (i.e. diameter of aneurysm in AAA and intensity of symptoms in PAD). 8 , 9 Some previous studies pointed to a significant role of procoagulant activity of intraluminal thrombus in patients with AAA 10 while in case of PAD, the most crucial pathomechanism is related to atherosclerotic endothelial damage which leads to the formation of thrombi and subsequent activation of hemostasis. To the best of our knowledge there are no available reports directly comparing these two groups of patients in terms of baseline preoperative coagulation and fibrinolysis activity.
Large perioperative cohort studies showed that cardiac complications are the leading cause of death after noncardiac surgery. 11 , 12 The emphasis has recently been put on myocardial injury after noncardiac surgery (MINS) which is defined as a postoperative troponin elevation attributable to ischemia. The underlying pathophysiology of MINS has not been well established yet. The two most plausible mechanisms are atherosclerotic plaque rupture with further thrombosis (type I myocardial infarction) and oxygen supply/demand mismatch (type II myocardial infarction).13–16 Nonetheless, the elevated concentration of coagulation, fibrinolysis, and inflammation markers is associated with an increased cardiovascular risk, including a higher prevalence of perioperative myocardial injury. 17 These abnormalities seem to be shifted further toward hypercoagulability by the procedure itself, probably rendering patients even more susceptible to cardiovascular complications.18–20
We hypothesized that patients undergoing vascular surgeries for PAD and AAA differ in terms of preoperative coagulation and fibrinolysis activity. We additionally aimed to evaluate this association in the context of other potentially relevant factors. Moreover, we suspected that study group with more pronounced coagulation might have higher rate of cardiovascular events.
Methods
Patients
This study, conducted between October 2010 and November 2013, was a substudy of Vascular events In noncardiac Surgery patIents cOhort evaluatioN Study (VISION; NCT00512109) which was a prospective observational cohort study. Details concerning screening, enrollment, and data gathering in the VISION Study were described in previous reports. 11 Consistently with VISION enrollment criteria, patients at the age of ≥45 years who received general or regional anesthesia for noncardiac surgery and who were hospitalized at least overnight after the procedure was included. We recruited 475 patients undergoing elective open vascular surgery in the Vascular Surgery Department, St John Grande Hospital, Krakow, Poland. The exclusion criteria were surgery for carotid artery disease, surgery for acute bypass graft thrombosis, cancer, estimated glomerular filtration rate <30 ml/min, deep vein thrombosis within three months prior to surgery, or an acute infection. In this study group, we identified 47 patients who met prespecified criteria for MINS and matched 84 controls in a 1:2 ratio based on age, sex, indication for surgery, cardiovascular risk factors, and heparin use before surgery, as described in a previous report published by our group. 17 Finally, the study group comprised 131 patients in whom we performed laboratory measurements described below. Study flow-chart is presented in Figure 1.
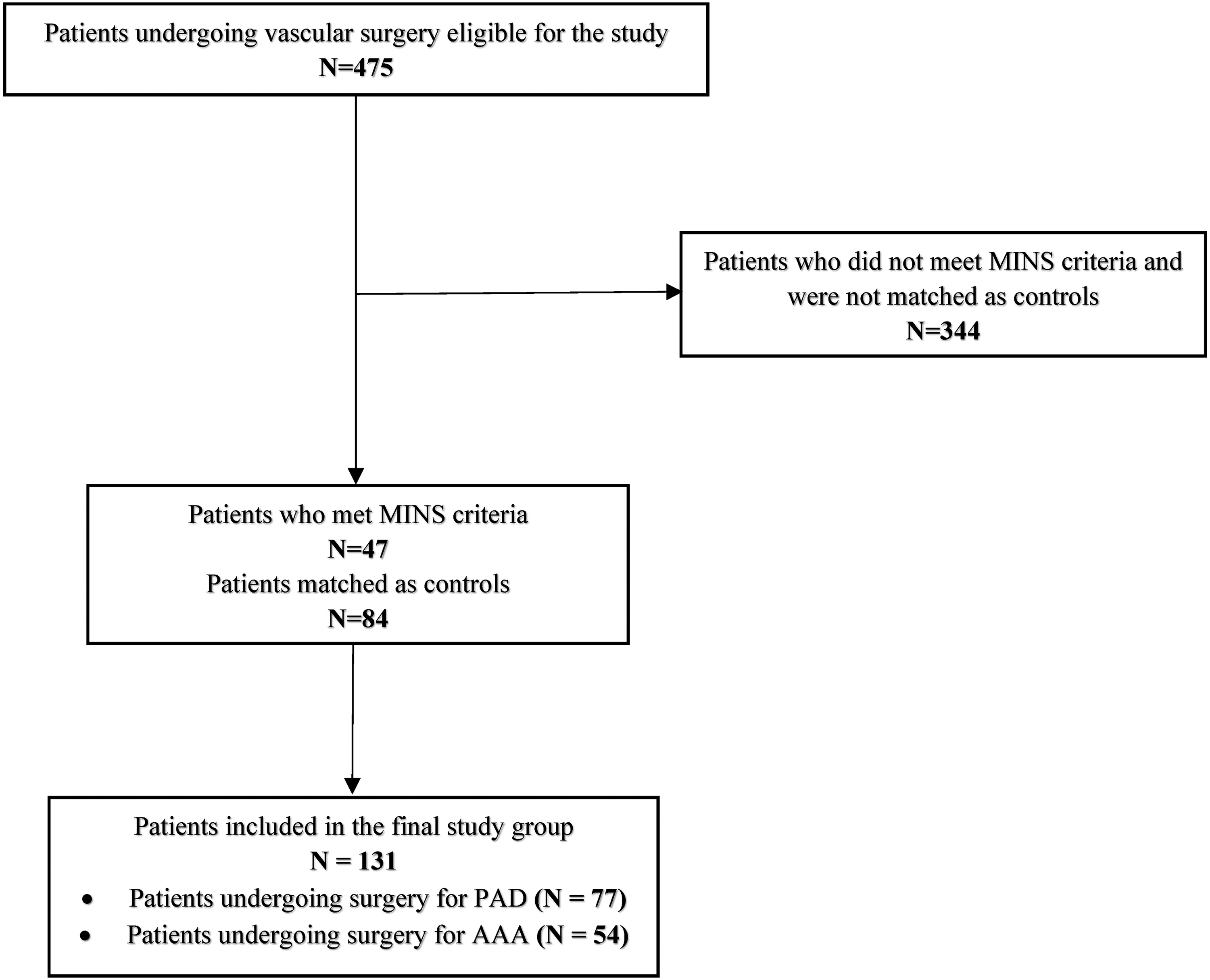
Study flow-chart. AAA: abdominal aortic aneurysm; MINS: myocardial injury after noncardiac surgery; PAD: peripheral artery disease.
Laboratory tests
Standard perioperative laboratory results were recorded, including platelet count, hemoglobin, and creatinine level. In all patients high sensitive troponin T (hsTnT; Elecsys 2010 analyzer; Roche, France) was measured before surgery, 6–12 h postoperatively and on the first, second, and third day after surgery. Blood samples (serum and plasma) were collected in serum separation tubes and into 3.2% (0.109 mol/l) sodium citrate tubes (one part sodium citrate to nine parts venous blood) and spun for 10 min at 3500 r/min at room temperature within 2 h from sampling. Serum and plasma samples were then stored at −80°C until in a validated freezer for further study.
Preoperative levels of the following blood biomarkers were measured in platelet poor plasma:
antithrombin (chromogenic method; Innovance Antithrombin, Siemens, Germany); activity of factor VIII (F VIII; one-stage clotting assay, Siemens, Germany); activity of von Willebrand factor:Ristocetin cofactor (vWF:CoR; turbidimetric method; BC von Willebrand Reagent, Siemens, Germany); fibrinogen (Clauss method—Multifibren U; BCS XP analyzer, Siemens, Germany), dimer D (turbidimetric method; Innovance D-Dimer, Siemens, Germany); plasmin–antiplasmin (PAP) complexes (ELISA method; Technozym PAP Complex, Technoclone, Austria); tissue plasminogen activator (tPA; ELISA method; Zymutest tPA Antigen, Hyphen BioMed, France); soluble CD40 ligand (sCD40L; ELISA method; CD40 Quantikine ELISA Kit, R7D, United Kingdom).
Clinical data collection
Patients were interviewed preoperatively by the research personnel to gather data on age, sex, smoking status, comorbidities (hypertension, diabetes mellitus, overweight, atrial fibrillation, coronary artery disease, history of previous cerebrovascular events), and use of medications. In case of elevated hsTnT level an electrocardiogram was routinely performed. We recorded data about myocardial infarction, stroke, and death during the hospitalization and within 30 days after the procedure. The 30-day follow-up information was gathered during telephone call with a patient or patient’s family member by study personnel member.
Clinical outcomes definition
Myocardial infarction was diagnosed according to the Third Universal Definition of Myocardial Infarction. 21
Stroke was defined as a new focal neurological deficit thought to be vascular in origin with signs and symptoms lasting more than 24 h.
Primary clinical outcome in this study (major cardiovascular event) was defined as composite of death, myocardial infarction, and stroke within 30 days from surgery.
Statistical analysis
Categorical variables were presented as numbers (percentages), whereas continuous variables were reported as medians (interquartile range), if not specified otherwise. A complete case analysis was performed.
Categorical variables were compared using χ2 test or the Fisher’s exact test, while continuous variables were compared using Student’s t-test and Mann–Whitney U test as appropriate. Adjusted analyses were performed using ordinary least squares regression models. Type of surgery, age, sex, BMI, history of smoking, diabetes, as well as preoperative administration of heparin and antiplatelet therapy were included in the final multivariable regression model. We evaluated the assumption of normality of residuals and homoscedasticity and assessed multicollinearity using variance inflation factors. A two-sided P value <0.05 was considered statistically significant. Statistical analyses and graphs were performed with R Studio version 3.6.0 (R Project, Vienna, Austria), packages: rms, ggplot2.
The funding source had no involvement in the study design; the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication. The study was approved by the local ethics committee (Jagiellonian University Bioethics Committee; number KBET/74/B/2010). The protocol complied with the Helsinki Declaration. All participants provided written informed consent before being enrolled.
Results
Clinical characteristics
The study group comprised 131 patients at the mean age of 68.3 years (range: 50.0–87.0) of whom 100 (76.3%) were males. The indications for vascular surgery were PAD in 77 patients (58.8%) and AAA in 54 patients (41.2%). History of smoking, diabetes mellitus, and preoperative heparin use were more commonly reported in the PAD group while obesity was more prevalent in the AAA group. Detailed demographic and clinical characteristics of both study groups are described in Table 1.
Comparison of baseline characteristics between patients undergoing surgery for peripheral artery disease and abdominal aortic aneurysm.
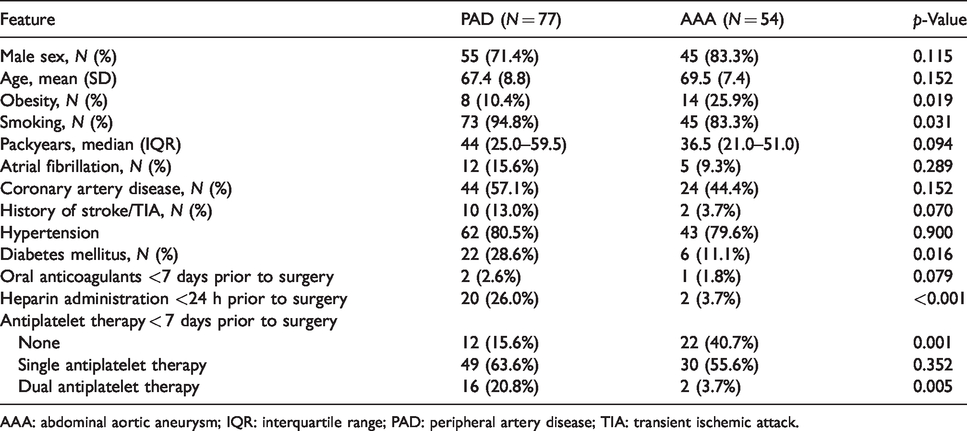
AAA: abdominal aortic aneurysm; IQR: interquartile range; PAD: peripheral artery disease; TIA: transient ischemic attack.
Markers of coagulation and fibrinolysis
Platelet count (250.5 versus 209.5 (× 10 3 /µl), p = 0.001) as well as levels of fibrinogen (5.4 versus 4.1 (g/l), p < 0.001), F VIII (176.9 versus 141.9 (%), p < 0.001), vWF:CoR (188.9 versus 152.3 (%), p = 0.009), and sCD40L (9016.0 versus 7936.6 (pg/ml), p = 0.005) were higher, while the dimer D (808.0 versus 2590.5 (ng/ml), p < 0.001) concentration was lower in PAD group compared to patients undergoing surgery for AAA. We did not observe statistically significant differences in the remaining markers’ levels. Detailed results are summarized in Table 2.
Comparison of preoperative coagulation and fibrinolysis markers between patients undergoing surgery for peripheral artery disease and abdominal aortic aneurysm.
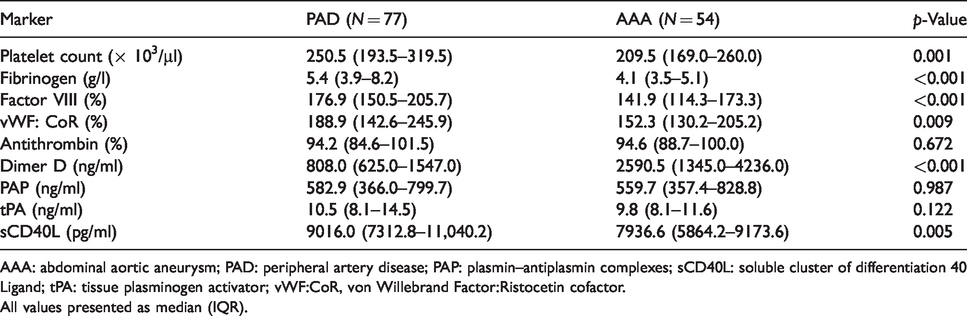
AAA: abdominal aortic aneurysm; PAD: peripheral artery disease; PAP: plasmin–antiplasmin complexes; sCD40L: soluble cluster of differentiation 40 Ligand; tPA: tissue plasminogen activator; vWF:CoR, von Willebrand Factor:Ristocetin cofactor.
All values presented as median (IQR).
Multivariable analysis
In a multivariable analysis we confirmed significant association between reason for surgery and concentrations of F VIII (p = 0.008), vWF:CoR (p = 0.006), fibrinogen (p = 0.014), and dimer D (p < 0.001). We also found that age is associated with levels of F VIII (p = 0.031), vWF:CoR (p = 0.003), and dimer D (p = 0.001), while diabetes is associated with level of F VIII (p = 0.02) and fibrinogen (p = 0.049). Beta coefficients with 95% confidence intervals are presented in Table 3 (only variables that reached statistically significant association with selected marker’s level) and Supplementary Table 1 (complete results of the multivariable analysis). The proportions of markers’ level variance explained by selected factors are summarized in Figure 2.
Results of the multivariable analysis.
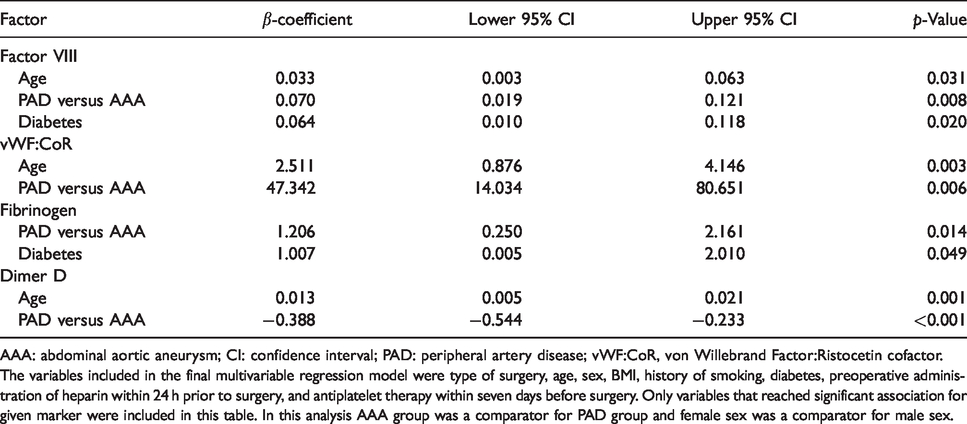
AAA: abdominal aortic aneurysm; CI: confidence interval; PAD: peripheral artery disease; vWF:CoR, von Willebrand Factor:Ristocetin cofactor.
The variables included in the final multivariable regression model were type of surgery, age, sex, BMI, history of smoking, diabetes, preoperative administration of heparin within 24 h prior to surgery, and antiplatelet therapy within seven days before surgery. Only variables that reached significant association for given marker were included in this table. In this analysis AAA group was a comparator for PAD group and female sex was a comparator for male sex.

Proportion of selected markers’ levels variance explained by factors included in the multivariable analysis. (a) F VIII, (b) von Willebrand Factor:CoR; (c) fibrinogen; (d) dimer D. In this analysis, group of patients with AAA was a comparator for PAD group and female sex was a comparator for male sex. APT: antiplatelet therapy; BMI: body mass index; PAD: peripheral artery disease.
Clinical outcomes
We did not observe any difference between patients undergoing surgery for PAD and those in the AAA group in a 30-day incidence of major cardiovascular event (39.0% (30/77) versus 29.6% (16/54), p = 0.271), myocardial infarction (35.1% (27/77) versus 29.6% (16/54), p = 0.233), and death (5.2% (4/77) versus 3.7% (2/77), p = 0.519). The incidence of stroke in PAD group accounted to 2.6% (2/77 patients) while none of the patients undergoing surgery for AAA suffered from stroke. Incidence of cardiovascular events is visualized in Figure 3. We observed higher concentration of PAP (711.7 versus 511.0, p = 0.048) in patients who developed major cardiovascular event compared to the remaining individuals without significant differences in the remaining markers’ levels. Detailed results are presented in Table 4.

Comparison of cardiovascular events rate between the study groups. AAA: abdominal aortic aneurysm; MACE: major cardiovascular event; MI: myocardial infarction; PAD: peripheral artery disease.
Comparison of preoperative coagulation and fibrinolysis markers between patients who developed major cardiovascular event and the remaining patients.
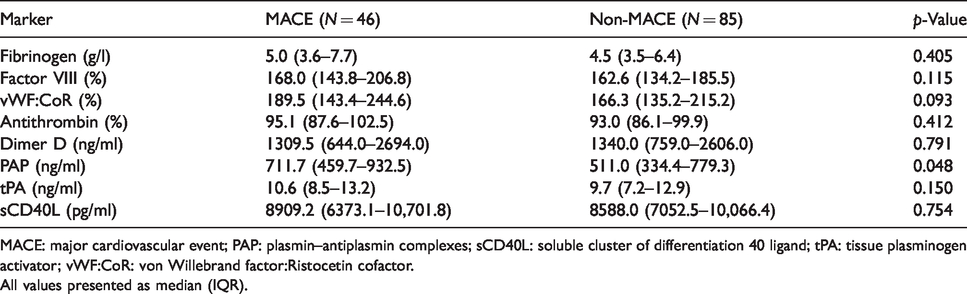
MACE: major cardiovascular event; PAP: plasmin–antiplasmin complexes; sCD40L: soluble cluster of differentiation 40 ligand; tPA: tissue plasminogen activator; vWF:CoR: von Willebrand factor:Ristocetin cofactor.
All values presented as median (IQR).
Discussion
In this observational study, including 131 patients undergoing vascular surgery, we affirmed our hypothesis that there are marked differences in preoperative profiles of coagulation and fibrinolysis activity between patients having surgery for PAD and AAA. Multivariable analyses additionally identified age and diabetes as factors associated with activity of evaluated systems. Surprisingly, there were no differences in incidence of cardiovascular events between the groups.
Higher levels of F VIII, vWF, and fibrinogen in patients with PAD suggest a more pronounced activation of coagulation in this population. One possible explanation is more advanced atherosclerosis in the PAD group, suggested by higher prevalence of coronary artery disease, cerebrovascular events, and higher concentration of sCD40L which is a protein involved in the development and promotion of atherosclerosis and its level probably correlates with cardiovascular risk. 22 , 23 Multivariable analysis revealed that there is an association between coagulation activity and reason for surgery as well as age and diabetes. This is not surprising considering data from previous reports suggesting major impact of these factors on coagulation. 24 , 25
Results concerning fibrinolytic activity are less coherent. Interpretation necessitates understanding that tPA:Ag represents the concentration of tPA:PAI-1 complexes and therefore its higher levels are indicative of hypofibrinolysis, while increasing concentrations of both PAP and the dimer D correlate with more pronounced fibrinolysis. 26 In a direct comparison between study groups, we observed higher dimer D concentration in AAA patients without statistically significant differences in tPA:Ag and PAP levels between the groups. Such results may suggest a relatively lower activity of fibrinolysis in patients undergoing surgery for PAD. Interpretation of absolute values also brings some valuable insights. The median concentrations of PAP are close to upper reference limit, while dimer D level is elevated in both groups which is consistent with previous reports suggesting increased preoperative fibrinolytic activity in patients undergoing vascular surgeries, particularly those with AAA. 7 Multivariable analysis confirmed the previously described positive association between dimer D level and age, but surprisingly did not show any relation with sex and history of smoking.
Majority of patients with vascular diseases receive medications potentially altering hemostatic function in the perioperative period. Heparin, which tends to lower serum levels of coagulation factors, including fibrinogen and F VIII and vWF:CoR, was used more commonly among patients with PAD. In order to minimize the risk of bias, we performed a multivariable analysis including both heparin and antiplatelet therapy which showed their surprisingly weak association with analyzed markers’ levels, therefore emphasizing strength of association between reason for surgery and coagulation and fibrinolysis activity.
Aside from their role in the assessment of coagulation and fibrinolysis activity, markers used in the present study were suggested as predictors of cardiovascular events. There are several reports showing an association between increased levels of F VIII, vWF:CoR, as well as fibrinogen and incidence of adverse cardiovascular events, both in medical and surgical populations.27–30 Our group previously showed an association between preoperative levels of coagulation and fibrinolysis markers and incidence of MINS. 17 Based on these data, we expected that the combination of more pronounced coagulation and lower fibrinolytic activity could potentially put patients with PAD at higher risk of major cardiovascular complications in comparison to those undergoing procedures due to AAA. Surprisingly, we did not observe significant differences in incidence of short-term major cardiovascular events between the groups. One possible explanation may be more evident activation of coagulation system during surgery for AAA, compared to PAD procedures, which could neutralize preoperative differences between these subgroups. Another potential explanation may be the complexity of perioperative cardiovascular complications etiology with multitude aspects that need to be taken into consideration, e.g. demographic and clinical variables as well as factors related to type II myocardial infarction (oxygen supply/demand mismatch). Interestingly, an additional comparison between patients who developed major cardiovascular event and the remaining patients did not show significant between-group differences in concentrations of coagulation markers. It may suggest that alterations in coagulation and fibrinolysis play more important role in the development of myocardial injury, while major cardiovascular complications are probably influenced by other factors to higher extent.
Further prospective studies on larger samples, utilizing serial measurements of coagulation and fibrinolysis activity with modern laboratory techniques, complemented by a comprehensive assessment of perioperative complications are warranted in order to precisely assess the role of coagulation and fibrinolysis in this setting. Such knowledge could provide us with potential targets for future prophylactic and therapeutic interventions, ultimately leading to the improvement of patients’ outcomes.
Our study has several limitations. The use of classic coagulation and fibrinolysis markers allows to assess the activity of these systems only in one specific moment, while the use of global tests, such as rotational thromboelastometry and thrombography offers a real-time, dynamic, and exact description of the coagulation and fibrinolytic activity. Moreover, the analysis of platelet count could be expanded by use of platelet function tests, particularly in the light of common use of antiplatelet therapy in the study group. Also, we lack data concerning clinical severity of analyzed diseases (aneurysm size and presence of intraluminal thrombus in case of AAA and Fontaine or Rutherford classifications in case of PAD), which could offer some additional explanation of differences between the groups. Finally, we were unable to perform a reliable multivariable analysis concerning clinical outcomes due to limited number of events.
Conclusions
The present study suggests a higher activity of coagulation accompanied by a relatively less pronounced fibrinolysis in patients undergoing surgery for PAD compared to those having a procedure for AAA without apparent differences in perioperative complications rate.
Supplemental Material
sj-pdf-1-vas-10.1177_1708538120937127 - Supplemental material for Perioperative cardiovascular complications rate and activity of coagulation and fibrinolysis among patients undergoing vascular surgery for peripheral artery disease and abdominal aortic aneurysm
Supplemental material, sj-pdf-1-vas-10.1177_1708538120937127 for Perioperative cardiovascular complications rate and activity of coagulation and fibrinolysis among patients undergoing vascular surgery for peripheral artery disease and abdominal aortic aneurysm by Kamil Polok, Jacek Górka, Jakub Fronczek, Teresa Iwaniec, Karolina Górka and Wojciech Szczeklik in Vascular
Footnotes
Authors’ contribution
All authors (KP, JG, JF, TI, KG and WS) made a substantial contribution to the concept or design of the work; or acquisition, analysis, or interpretation of data; drafted the article or revised it critically for important intellectual content; approved the version to be published; and have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Polish Ministry of Science and Higher Education (Grant number NN402083939 and DI2011023141).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.