
Abstract
Objective
The current literature on the major complications of embolo-sclerotherapy of upper and lower extremity vascular malformations is scarce. Evaluating and understanding the rates and types of potential major complications of embolo-sclerotherapy of vascular malformations help treatment planning and informed consent. Therefore, this study reviewed major complications following embolo-sclerotherapy of all upper and lower extremity vascular malformations in a single specialized multidisciplinary vascular malformation center over a 5-year period.
Methods
All patients with vascular malformations underwent multidisciplinary directed intervention. Demographic, procedural, follow-up, and complication data were collected prospectively in a dedicated database, and reviewed retrospectively. Major complications for upper and lower extremity vascular malformations from 1 January 2013 to 31 December 2017 were analyzed. All embolo-sclerotherapies of high-flow vascular malformations (HFVMs) were performed under selective catheter angiography and direct injection, but low-flow vascular malformations (LFVM) with direct injection only. Major complications were defined as any tissue or functional damage caused by direct injection, distal embolization, or tissue reaction.
Results
Seventy patients (median age of 25 years; 44 males and 26 females) had 150 embolo-sclerotherapy procedures for upper extremity vascular malformation. Of these, 28 patients had embolo-sclerotherapy for HFVM and 42 patients for LFVM; total 78 and 72 procedures, respectively. A total of 107 patients (median age of 26 years; 42 males and 65 females) had 160 embolo-sclerotherapy interventions for lower extremity vascular malformations. Of these, 18 patients had embolo-sclerotherapy for HFVM and 89 patients for LFVM; total of 30 and 130 procedures, respectively. The overall major complication rates following embolo-sclerotherapy of upper and lower extremity vascular malformations were 14.3% and 4.7%, respectively (P = 0.030). In the upper extremity HFVM group, major complications from embolo-sclerotherapy occurred in five patients; three ischemic fingers requiring amputation and two skin ulcerations. Meanwhile, in the upper extremity LFVM group, major complications occurred in five patients; one median nerve injury requiring nerve grafting and hand therapy, one hand contracture requiring tendon release, and three skin ulcerations. There was only one major complication, which was cellulitis in the lower extremity HFVM group. In the lower extremity LFVM group, major complications occurred in four patients; two skin ulcerations, one cellulitis, and one deep vein thrombosis.
Conclusions
Embolo-sclerotherapy is relatively safe for upper and lower extremity vascular malformations in a high-volume experienced center where our major complication rates were 14.3% and 4.7%, respectively, which compare favorably or similar to those reported in most recent literature. These outcomes will direct treatment strategies to avoid local and systemic toxic complications in the upper and lower extremity, for both HFVM and LFVM, and to improve informed consent.
Keywords
Introduction
Embolo-sclerotherapy (EST) is an important interventional treatment for vascular malformations (VMs) including those in the upper and lower extremities.1–5 Despite being minimally invasive, EST for upper and lower extremity VMs carries significant risk of major complications including ischemia, infarction, amputation, nerve injury, contracture, and ulceration.1,3–9 For example, major complication rates of as high as 61% and 24% for hand and foot arteriovenous malformation (AVM) treatments, respectively were most recently reported.3,4 A recent study reported a complication rate of 12.3% from sclerotherapy of intramuscular venous malformation of the upper and lower extremity. 9 Post-operative death including from pulmonary embolism following EST of peripheral VM has also recently been reported. 10
Despite improved care in specialist centers, up-to-date estimates of complication risk for audit and informed consent are scarce; recent literature focuses on high-flow vascular malformations (HFVM) with a paucity of data for low-flow vascular malformations (LFVM). Therefore, this study aimed to review major complications following EST of all upper and lower extremity VM in our specialized multidisciplinary center for vascular anomalies over a 5-year period. Improving our existing understanding and knowledge on major complications following EST, particularly when the information in the literature on this was scarce, would help direct treatment strategies to avoid local and systemic toxic complications in the upper and lower extremity, for both HFVM and LFVM, and to aid informed consent.
Methods
This is a retrospective audit study of a prospectively collected departmental database with no patient identifiable data used; that was carried out for service improvement as part of the clinical governance of the department, hence did not require institutional review board approval and informed consent.
Embolo-sclerotherapy
All patients with non-central nervous system VM treated in our hospital underwent multidisciplinary team (including vascular surgeons, interventional radiologists, and clinical nurse specialist) review directed intervention. Our center received tertiary referrals of peripheral vascular anomalies from around the country. All the clinicians in the multidisciplinary team who performed the EST in this study were consultant interventional radiologists and consultant vascular surgeons with subspecialty interest and training in managing peripheral vascular anomalies. EST was our mainstay interventional treatment for patients with rapidly growing and/or significantly symptomatic VMs, which included pain and discomfort, disfiguration, swelling, pressure effect, ulceration, bleeding, localized intravascular coagulopathy, and cardiac failure. Patients with asymptomatic or minimally symptomatic VMs, which were stable, were treated with conservative treatment.
Clinically, we classified the VM into HFVM when it is an AVM; whereas LFVM when it is not an AVM such as venous, lymphatic, capillary, and a combination of these. Pre-operative cross-sectional images i.e. computed tomography (CT) and/or magnetic resonance imaging were performed on all patients to aid planning of the EST. All ESTs were performed under general anesthetics to limit patient movement and anxiety. All ESTs of HFVM were performed under selective catheter angiography and direct injection, but LFVM with direct injection only. All ESTs during this study were carried out under fluoroscopy guidance with digital subtraction angiography performed to confirm the accurate position of the catheter and/or needles, and to assess the flow; either in a vascular hybrid theatre with a floor mounted C-arm or standard operating theatre with a mobile C-arm. Ultrasound was also used in some cases, but not cone beam CT. ESTs were performed either with foam sclerosants (sodium tetradecyl sulfate 3% or polidocanol; mixed with air in either 1:4 or 3:8 ratio), ethanol, embolization coils, a few other substances such as Onyx, and a combination of them (Table 1), and the choice of agents used was determined based on the operator’s discretion. The majority of the ESTs were carried out as day cases, and followed up in the out-patient clinic around 6–12 weeks post-operatively.
EST agents used for LFVMs and HFVMs in this study.

EST: embolo-sclerotherapy; STS: sodium tetradecyl sulfate.
Data collection
All patients with HFVM and LFVM of upper and lower extremities, who underwent EST in our center from 1 January 2013 to 31 December 2017 were identified. Demographic, anatomical, procedural, treatment outcome, complication, and follow-up data collected in a prospective database were analyzed. Major complications were defined as any tissue or functional damage caused by direct injection, distal embolization or tissue reaction. The major complications in the study were determined by our multidisciplinary team described above.
Statistical analysis
Data was collected and analyzed using Microsoft Office Excel (Redmond, Washington, USA) and GraphPad Prism 7.04 (GraphPad Sorftware, San Diego, CA). Data was presented as median and range. Proportional data was presented in percentage. Differences in the rates of major complications between subgroups were analyzed using Chi-square and Fisher’s exact tests. P < 0.05 was considered significant.
Results
Upper extremity vascular malformations
Patients
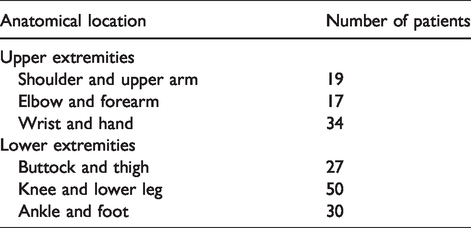
During the study period, 70 patients had a total of 150 EST procedures for upper extremity VMs with a median age of 25 years (range 1–73 years); 44 (63%) males and 26 (37%) females. Of these, 28 (40%) had EST for HFVM and 42 (60%) for LFVM; total of 78 and 72 procedures, respectively. All the LFVM in the upper extremity were venous except one lymphatic malformation. Table 1 summarizes the embolizing agents used for all the EST procedures for upper and lower VM. Meanwhile, Table 2 summarizes the anatomical distribution of the VMs in the upper and lower extremities. EST involving the hand were done in 21 patients (75%) or 64 procedures (82%) for HFVM, and 15 patients (35%) or 29 procedures (40%) for LFVM.
Anatomical distribution of the vascular malformations treated with EST in the upper and lower extremities.
Major complications
In total, ten patients (14.3%) sustained major complications from EST procedures of upper extremity VMs over 5 years (6.7% of total procedures). In the upper extremity HFVM group, major complications from EST occurred in five patients (17.9%) or 6.4% of total procedures. Meanwhile, in the upper extremity LFVM group, major complications occurred in five patients (11.9%) or 6.9% of total procedures. The major complications for the EST of the upper extremity VMs in the study were summarized in Table 3. Figure 1 shows an angiogram and photographs of ischemic and gangrenous right distal index and little finger requiring amputation in a patient who had EST of HFVM of the hand. Figure 2 shows photographs of skin ulceration of the dorsum of the right hand of a patient who had EST of LFVM of the hand. Significant differences in the rate of major complications were observed when anatomical distributions of the upper extremity VMs were compared (P = 0.016; Chi-square test). However, no significant difference in the major complication rates was found between EST of HFVM and LFVM of the upper extremities (P = 0.507; Fisher’s exact test).
Patients with major complications following EST of upper extremity vascular malformations.

EST: embolo-sclerotherapy; HFVM: high-flow vascular malformation; LFVM: low-flow vascular malformation; STS: sodium tetradecyl sulfate.

Angiogram and photographs of ischemic and gangrenous right distal index and little finger requiring amputation in a patient who had EST of HFVM of the hand.

Photographs of skin ulceration of the dorsum of the right hand of a patient who had EST of LFVM of the hand.
All skin ulcerations resolved with medical treatment only without significant long-term disability. However, the nerve injury, hand contracture, and amputations carried some degrees of long-term functional disability. The patient who developed muscular contracture subsequently underwent tendon release surgery with good overall functional outcome eventually. Meanwhile, the patient who suffered median nerve injury subsequently underwent nerve grafting by the plastic surgeons, and required on-going hand therapy and neurological follow-up. The three patients, all underwent EST for HFVM of the hand, developed ischemic and gangrenous fingers secondary to distal embolization with or without some degree of steal syndrome from the HFVM, and required amputation.
Lower extremity vascular malformations
Patients
A total of 107 patients had 160 ESTs with the median age of 26 years (range 8–70 years); 42 males (39%) and 65 (61%) females. Of these, 18 patients (17%) had EST for HFVM and 89 patients (83%) for LFVM; total of 30 and 130 procedures, respectively. Similar to the upper extremity, all the LFVM in the lower extremity were venous except one lymphatic malformation. EST involving the foot were done in 6 patients (20%) or 6 procedures (82%) for HFVM, and 24 patients (27%) or 26 procedures (20%) for LFVM.
Major complications
During the study period, 5 (4.7%) patients or 3.1% of total procedures experienced major complications from EST of lower extremity VMs. In the lower extremity HFVM group, major complications from EST occurred in one patient (5.6%) or 3.3% of total procedures. Meanwhile, in the lower extremity LFVM group, major complications occurred in four patients (4.5%) or 3.1% of total procedures. The major complications for the EST of the lower extremity VMs in the study were summarized in Table 4. Figure 3 shows a photograph of skin ulceration with blistering of a patient who had EST of LFVM of the foot. For EST of the lower extremity VMs, there were no significant differences found in the rates of major complications when anatomical distributions (P = 0.877; Chi-square test) and the flow of the lesions (P > 1.000; Fisher’s exact test) were compared. However, there was a significant difference observed in the rates of major complications from EST between upper and lower extremity VMs (P = 0.030; Fisher’s exact test).
Patients with major complications following EST of lower extremity vascular malformations.
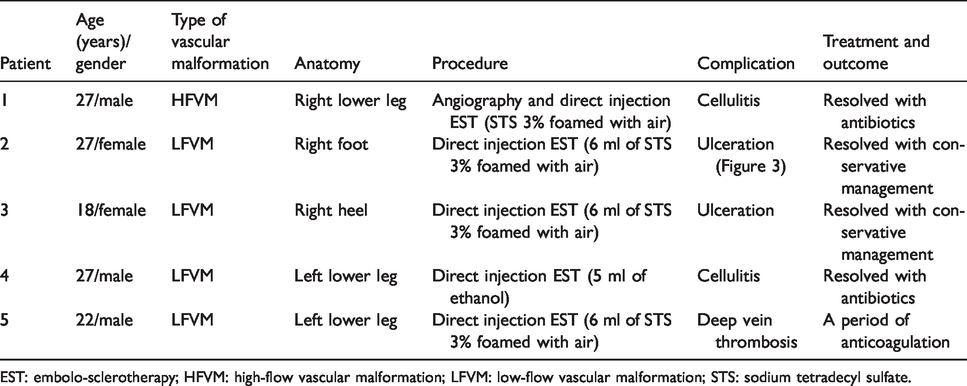
EST: embolo-sclerotherapy; HFVM: high-flow vascular malformation; LFVM: low-flow vascular malformation; STS: sodium tetradecyl sulfate.

Photograph of skin ulceration with blistering of a patient who had EST of LFVM of the foot.
All the major complications of the lower extremity EST resolved with medical treatment without significant long-term physical or functional disability although the single DVT case required a period of anticoagulation only.
Discussion
This study reported a wide range of major complications from EST of upper and lower extremity VMs including some with long term implications. There was significantly higher rate of major complications found in the EST of the upper than the lower extremity VMs. The majority of major complications reported in this study were due to local toxicity of the EST agents, particularly in those treated for LFVM, causing skin ulceration, cellulitis, hand contracture, and median nerve injury causing wrist drop. It is worth pointing out that our major complications from EST of the upper extremity HFVM and LFVM appeared to be significantly high in the wrists and hands, particularly when the fingers were involved. Therefore, performing EST on any VM that involves the wrists and hands must be regarded as potentially high risk and should not be taken lightly, with all patients appropriately counseled and the potential for major complications thoroughly explained. Furthermore, upper and lower extremities vary in terms of their anatomy such as vascularity and distribution of the nerves, and functions, hence they are likely to have differences in their complication rates and profiles even though the EST technique used is the same. Interestingly, there were no significant differences found in the major complication rates from EST of HFVM and LFVM within the upper and lower extremity groups in this study although the sample size of this study might be too small to demonstrate this.
Understanding the major complication rates of EST for VMs is important in helping clinicians and patients make decisions with informed consent. Although EST is widely used to treat VMs of the upper and lower extremity VMs, there are only a few studies reporting on the complication rates in recent literature. Vogelzang et al. retrospectively evaluated endovascular therapy, principally with ethanol embolization, for 46 patients with VMs including nine involving the upper extremity, 31 in the lower extremity and 6 in the trunk, in a single center; with the overall complication rate of 24%. 5 Park et al. reported a complication rate of 61% for ethanol EST in hand AVMs in a retrospective study of 31 patients. 4 These complications included skin necrosis in 14 patients (45%), bullae in 7 patients (23%), joint stiffness or contracture in 6 patients (19%), and transient nerve palsy in 4 patients (13%); all of them resolved completely except in 2 patients who underwent amputation. In another retrospective study, a complication rate of 49% was reported in 41 patients who underwent EST with ethanol involving the hand; 17 patients with skin necrosis (including one who had autoamputation and two who underwent amputation) and 7 patients with transient neuropathic complications. 8 Hyun et al. retrospectively reviewed 29 patients who had ethanol EST for foot AVMs, and reported major and minor complication rates of 24% and 52%, respectively; skin necrosis being the most common for the latter. 3 More recently, Park et al. retrospectively reviewed 306 patients with body and extremity AVMs who were treated over 20 years, during which 913 endovascular therapies were performed. 11 The overall major and minor complication rates by number of procedure were 3.1% and 20.1%, respectively. The most common complications reported included skin necrosis, bullae formation, and nerve injury. A recent single center retrospective study of 81 patients reported a complication rate of 12.3% from sclerotherapy of upper and lower extremity intramuscular venous malformation. These complications included one case of major nerve injury, six cases of skin necrosis and ulceration, and three cases of superficial venous thrombosis. 9 Our complication rates in this study appeared to compare favorable or similar to those in the literature; likely as a result of experience bias i.e. performance by high skilled operators at a specialized center with high volume of cases, and as such may merit these cases being done by similar type of professionals. Furthermore, it is important to note that the anatomical distributions and types of VMs, and the definitions of complications as well as the classification of their severity varied among studies. Moreover, so far there is no agreed reporting guidelines or consensus on what are considered complications and their severity following EST of VM. Such reporting guidelines and consensus is clearly needed to compare clinical outcomes between studies.
It is important to stress that this study was not designed to evaluate if any particular EST agent of any concentration was safer than the others for upper and lower extremity VMs. Therefore, we could not draw any conclusion on or recommend which EST agent or combination of agents was associated with the lowest risk of major complications. Meanwhile, there is no high level of evidence in the literature to support the method of EST, and the choice and concentration of agents, hence experience and familiarity with techniques remains the most reliable determinants of clinical outcomes.10,12 For example, foam sclerotherapy with STS is often used to treat LFVM, whereas ethanol is used for both HFVM and LFVM.13–15 The overall complication rate of ethanol sclerotherapy of AVM has been reported to be relatively high, ranging from 10% to 52%; with the use of absolute ethanol to be associated with the highest complication rates.2,11,16–20 Therefore, diluted ethanol has been used to reduce complication rate and ethanol dose. 11 It is also often reported that sclerotherapy with STS carries lower toxicity than ethanol.1,13–15,21 Our experience with foamed STS, which is our most commonly used EST agent including in this study, has been good in terms of clinical efficacy and safety, for both HFVM and LFVM. Therefore, our selective use of foamed STS over alcohol might have contributed to our relatively favorable major complication rates although further studies will be required to confirm this. It is also important to be aware that all EST agents can potentially cause local and systemic complications; hence, they must always be used cautiously, appropriately and within their recommended indications. Staged approach of EST in some cases of extensive VM, might reduce the risks of complications and toxicity of the sclerosants. We also believe that other factors including our multidisciplinary management approach, improved classification and targeted treatment, increasing learning curve and clinical experience, and high volume of cases for EST of upper and lower extremity VMs performed in our center were also important.6,11,22
Only simple statistical analyses were used and deemed sufficient to meet the aim of this study to report on the types and rates of major complications from EST of VM in the upper and lower extremities in our practice. Rigorous statistical analyses were considered but unlikely to provide additional clinical value in this study due to the relatively small number of major complications, highly heterogeneous groups of patients and lesions, and evaluation of the subgroups such as between HFVM and LFVM or upper and lower extremities, was not really comparing like with like. Future prospective studies with larger samples and longer follow-up should focus on assessing the potential factors that determine outcomes and complications including with multivariate analysis.
Limitations
There were several limitations in this study. Firstly, although our database was prospectively collected, the data was analyzed retrospectively, hence, leading to potential biases. All major complications were identified and recorded prospectively in the database, hence likely to reduce the risk of potential selection bias. Secondly, despite being a high-volume tertiary center for vascular anomalies, statistical differences between the subgroups, hence the potential risk factors for major complications of EST in this study should be interpreted with caution due to the large heterogeneity of VMs. Since VM is relatively uncommon, any larger sample size study will require a multi-center design including a registry. Thirdly, our definition of major complication might differ from those used in other similar studies in the literature. However, there was no one universally accepted definition of what should be considered as major complication following EST. Our major complications were identified by the multidisciplinary team including the vascular surgeons and interventional radiologists based on our clear definition. Finally, detailed information particularly as per the International Society for the Study of Vascular Anomalies and Schobinger classification were not routinely collected hence not fully included in this study. However, we provided information such as the flow, predominant vessel type, anatomical location, and patient demography, which were often considered clinically relevant when planning for EST treatment strategy. Since only patients with rapidly growing and/or significantly symptomatic patients were offered EST, most if not all of the patients with HFVM treated in this study should be stage II to IV on Schobinger classification.
Conclusions
Current EST is relatively safe for upper and lower extremity VMs in a high-volume experienced center where our major complication rate of 14.3% and 4.7%, respectively, compare favorably or similar to those reported in most recent literature. This is possibly due to our multidisciplinary management approach, improved classification and targeted treatment, and high volume of cases. These outcomes will direct treatment strategies to avoid local and systemic toxic complications in the upper and lower extremity, for both HFVM and LFVM, and to improve informed consent. Finally, an internationally agreed reporting guidelines or consensus is clearly needed to define complications following VM interventions including EST to allow meaningful comparison between studies.
Supplemental Material
sj-jpg-1-vas-10.1177_1708538120937616 - Supplemental material for Incidence of major complication following embolo-sclerotherapy for upper and lower extremity vascular malformations
Supplemental material, sj-jpg-1-vas-10.1177_1708538120937616 for Incidence of major complication following embolo-sclerotherapy for upper and lower extremity vascular malformations by Chung Sim Lim, Nicholas Evans, Ishapreet Kaur, Anthie Papadopoulou, Mohamed Khalifa, Janice Tsui, George Hamilton and Jocelyn Brookes in Vascular
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by researchers (CSL and JT) at the National Institute for Health Research University College London Hospitals Biomedical Research Centre.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.