
Abstract
Objectives
Endovascular therapy using balloon expandable stents has become the treatment standard for most iliac atherosclerotic lesions. We aimed to assess the safety and performance of the Dynamic stainless-steel balloon-expanding stent system in this location.
Methods
BIODYNAMIC is a retrospective single center study including consecutive patients with iliac lesions treated with the Dynamic stent system. Not included were implantations inside an endograft. The primary endpoint was freedom from major adverse limb events (MALE) at 12 months, defined as index limb amputation or target lesion revascularization (TLR). Secondary endpoints were procedure success, ankle brachial index (ABI) and Rutherford class change, mortality and freedom from TLR after 12 months.
Results
Within two years, 182 patients with 234 lesions in the common iliac artery were enrolled. Rutherford class 5 and 6 were present in 11.5% of patients, average stent diameter was 8.0 ± 0.5 mm and stented length 40.0 ± 15.3 mm. The primary endpoint was reached in 96.2% (225/234) of the cases, with six TLR (2.6%) and three target limb amputations (1.3%). Procedure success was obtained in all but three patients (98.4%). In paired analysis, ABI improved by 0.25 ± 0.21 from baseline to 0.90 ± 0.16 post-procedure and Rutherford class improved by −1.75 ± 1.53. There were four non-device–related deaths (2.2%). Freedom from TLR was 97%, 95.3%, 94% and 92.7% at 24, 36, 48 and 60 months, respectively.
Conclusion
The Dynamic balloon-expandable stent system proved to be safe and effective in a population with common iliac artery lesions.
Introduction
Peripheral artery disease (PAD) is a common and serious disease with the formation of atherosclerotic plaque that restricts the blood flow to the extremities. Prevalence and incidence increase with age, and more than 10% of people in their 60 s and 70 s are affected. Worldwide, more than 200 million patients suffer from PAD, with approximately 30% of them having a lesion located in the iliac arteries.1,2
Studies like BRAVISSIMO have indicated that with current stent systems, the treatment not only of TASC A & B lesions is possible, but also more complex lesion including TASC C & D can often be treated by endovascular procedures.3 Already in 1997, a meta-analysis by Bosch and Hunink concluded that compared to plain balloon angioplasty, the technical success rate was higher after stent implantation which also reduced the risk of long-term failure. 4 As a result, stenting in the iliac artery has become the standard in many centers and guidelines recommend stenting particularly in short lesions.5,6
Balloon-expandable, self-expandable and, more recently, covered stents are used to treat iliac disease. Balloon-expandable devices offer the advantage of higher radial outward force making them useful in calcified lesions. Mostly, they can be deployed with greater precision, leading to more accurate placement and target lesion coverage compared to self-expanding stents.5,7,8 However, published long-term data on balloon-expanding stents are scarce, particularly for Rutherford classes ≥4. With the BIODYNAMIC analysis (BIOtronik – For the Treatment of Iliac Atherosclerotic Lesions Using the Balloon-expanding DYNAMIC bare metal stent), we aimed to assess the safety and performance of the Dynamic balloon-expandable stainless-steel stent system (Biotronik AG, Buelach, Switzerland) in patients with iliac artery lesions treated at a single center in Germany.
Patients and methods
Study design and patient population
BIODYNAMIC is a single center retrospective cohort study of consecutive patients who underwent endovascular interventions of the iliac arteries using the Dynamic balloon-expandable stent between 2014 and 2015 and signed informed consent respective a data release form. Stents implanted in an endograft were not included. The procedure and medication followed common medical routine. Baseline and procedural data were retrospectively collected as well as follow-up data at 30 days and ≥12 months. The registry was conducted according to the Declaration of Helsinki and ISO14155:2011 as far as applicable, and was approved by the regional ethic committee. All patients provided informed consent or a data release form.
Study device
The Dynamic stent system consists of a balloon-expandable stent mounted on an over-the-wire percutaneous transluminal angioplasty balloon catheter. The balloon-expandable stent is sculpted by laser from a single tube of 316 L stain-less steel and is completely coated with amorphous silicon carbide (a-SiC:H) that acts as a barrier between the stent and the surrounding tissue and blood, providing a barrier against iron release, and creating a surface that reduces platelet aggregation while facilitating endothelialization. 9 The stent ends are made of closed, ring-shaped elements and the struts in between are arranged in a helicoid fashion for optimal flexibility. Diameters of 5 to 8 mm are available in lengths of 15, 25, 38 and 56 mm. Diameter stents of 9 and 10 mm are available in nominal lengths of 25, 38 and 56 mm. The delivery system is compatible with 0.035″ diameter guidewires and introducers with inner diameters of 5 F to 7 F depending on stent diameter and lengths.
Study endpoints
The primary endpoint is freedom from MALE at 12 months post index procedure, a composite of target lesion revascularization (TLR) and index limb amputation. Secondary endpoints are (a) procedural success, defined as technical success (completion of the assigned procedure and <30% residual stenosis determined by angiography immediately after stent placement) and absence of MAE before hospital discharge, (b) primary patency at 12 months, defined as freedom from >50% restenosis based on the DUS peak systolic velocity ratio ≥2.5 10 or based on clinically driven TLR with angiographic evidence of >50% stenosis, (c) Rutherford classification, and (d) ankle brachial index (ABI). Further secondary endpoints are (e) freedom from mortality at 12, 24, 36, 48 and 60 months as well as (f) freedom from TLR at 24, 36, 48 and 60 months.
Statistical analysis
The sample size calculation was performed using the “binomSamSize” package in R for the primary endpoint MAE at 12 months. The following assumptions were made: Expected MAE rate of 8.9%, 11 half-width of 95% asymptotic (Wald) confidence intervals (CI) of 5.5%, confidence level α = 0.05, and a drop-out rate of 15%. The required number of subjects enrolled was calculated to be 122 subjects. Besides, 122 subjects enrolled will provide the 95% asymptotic CI for primary patency with the half-width of 6.2%, assuming 89% expected primary patency.
For quantitative variables, mean values and standard deviation are calculated. Comparisons from baseline to post-procedure were performed using Signed Rank Test. For qualitative variables, absolute and relative frequencies are determined. 95% CI are calculated when relevant. For combined and individual clinical endpoints, the survival rate (and 95% CI) was calculated using Kaplan-Meier estimator and Kaplan-Meier curves are presented. Statistical analyses were carried out using SAS 9.4 (SAS Institute Inc. Cary, NC, USA).
Results
From January 2014 to December 2015, 182 patients with 234 lesions were enrolled. Patients were 66.3 ± 9.9 years old and predominantly male (65.4%). Most had hypertension (83.0%) and around half of patients had hypercholesterolemia (57.1%) or were smokers (53.6%) (Table 1).
Baseline data.
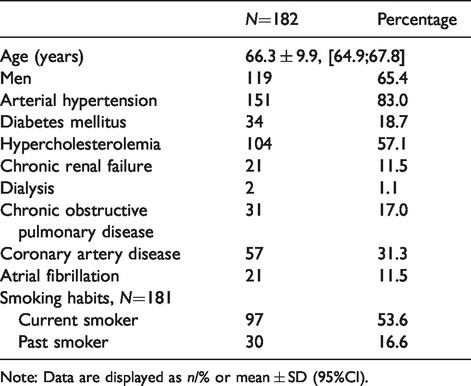
Note: Data are displayed as n/% or mean ± SD (95%CI).
Lesion characteristics are summarized in Table 2. Lesions were exclusively in the common iliac artery (CIA), mean stent diameter was 8.0 ± 0.5 mm and mean stented lengths 40.0 ± 15.3 mm (Table 3). The device could be implanted in all cases (Figure 1), and three procedural failures were caused by MAEs (two deaths and one TLR).
Lesion characteristics.

SD: Standard deviation; TASC: transatlantic society consensus.
Procedural data.
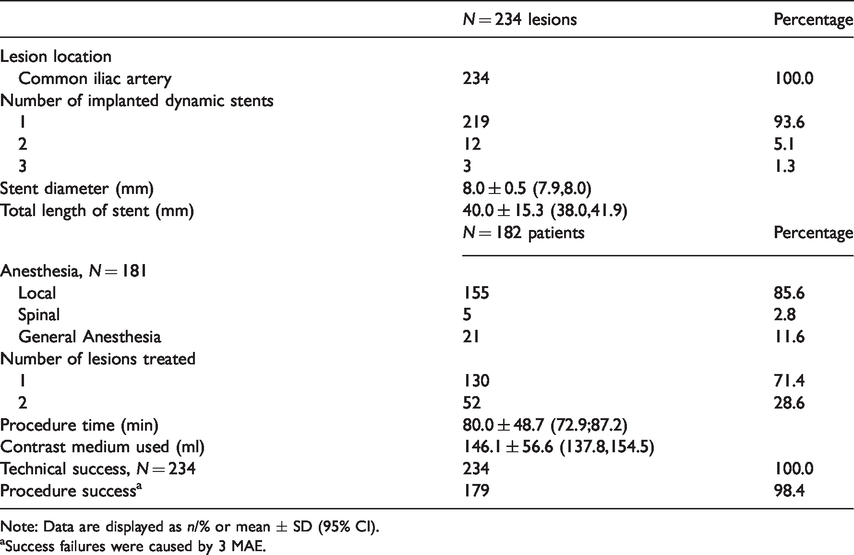
Note: Data are displayed as n/% or mean ± SD (95% CI).
aSuccess failures were caused by 3 MAE.
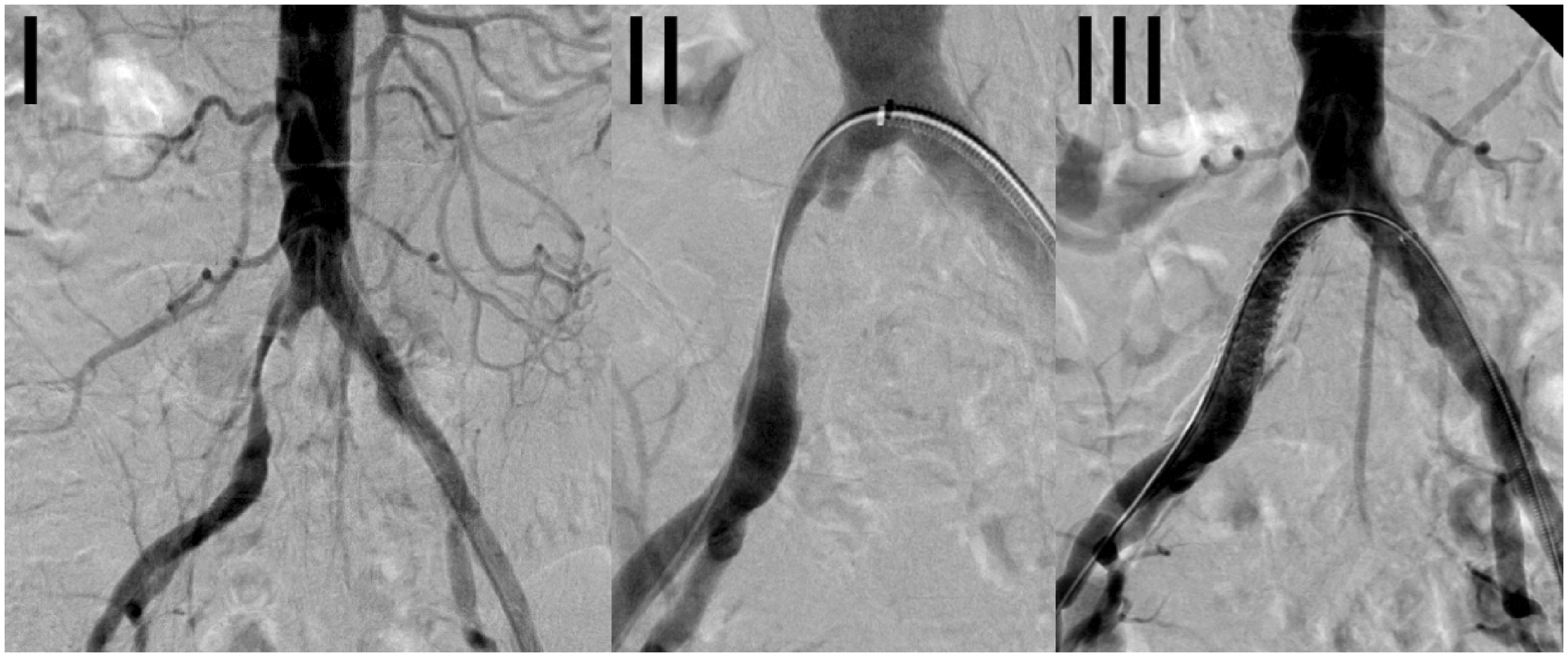
Case example. Angiograms of a 66-year-old male patient with intermittent claudication on the right side resulting from a high-grade common iliac artery stenosis (I). After passage of the wire and advancement of a 6 French sheath from the contralateral side (II), an 8 × 38 mm Dynamic Stent was placed in the right common iliac artery (III).
Follow-up data was available for 158 patients (86.8%) at 12 months, 136 patients (74.7%) at 24 months, 116 patients (63.7%) at 36 months, 86 patients (47.3%) at 48 months and 31 patients (17%) at 60 months. Mean follow-up was 39.5 ± 20.4 months.
At 12 months, the primary endpoint was reached in 96.2% (225/234) of the cases. There were three target limb amputations and six target lesion revascularizations. All patients with target limb amputation had diabetes at baseline, Rutherford class 5 or 6, and underwent femorocrural reconstruction due to concomitant PAD in the superficial femoral, popliteal and all three crural arteries. There were six target lesion revascularizations. One patient with instent stenosis was treated nine months after the index procedure by atherectomy (8 F Rotarex, Straub Medical, Wangs, Switzerland) and implantation of a stent-graft (Viabahn, WL Gore and Associates, Flagstaff, AZ). Five more patients with instent stenosis were treated between 7 and 11 months after the index procedure by drug-coated balloon angioplasty (In.Pact Admiral, Medtronic, Santa Rosa, CA, USA).
There were four deaths at 12 months (2.2%). None of the deaths were device-related. A 89-year-old patient with Rutherford class 6 and heart failure at baseline died on POD 6 of acute pancreatitis, sepsis and paralytic ileus. A 82-year-old patient with diabetes mellitus, coronary artery disease and heart failure at baseline died of multi-organ failure on POD 7. A 57-year-old patient with chronic limb ischemia due to distal aortoiliac occlusive disease, sepsis and Rutherford class 5 at baseline, died of sepsis and abdominal compartment syndrome from toxic megacolon with colitis on day 38. An 85-year-old patient with end-stage renal disease requiring dialysis, diabetes, coronary artery disease and heart failure at baseline died of unknown cause on day 240. Other complications included one myocardial infarction 30 days post-procedure and two strokes (1.1%, one patient had baseline atrial fibrillation). Acute renal failure occurred in four patients (2.2%), thereof one patient had baseline renal insufficiency, and two were older than 80 years.
Postoperative unpaired ABI and Rutherford data are shown in Figures 2 and 3. Mean ABI was 0.66 [95% CI: 0.64; 0.69] at baseline and improved to 0.90 [95% CI: 0.88; 0.93] post-procedure (prior to discharge). Paired ABI-data are available for 167 lesions showing a mean improvement of 0.25 ± 0.21 [95% CI: 0.22; 0.28], p < 0.0001, from baseline to post-procedure. Rutherford class had improved with 70.3% having less than severe claudication (37.5% in Rutherford class 0, 21.9% in class 1, 10.9% in class 2, 17.2% in class 3, 6.3% in class 4, 4.7% in class 5 and 1.6% in class 6). Longer term freedom from mortality and TLR rates are provided in Figures 3 and 4.
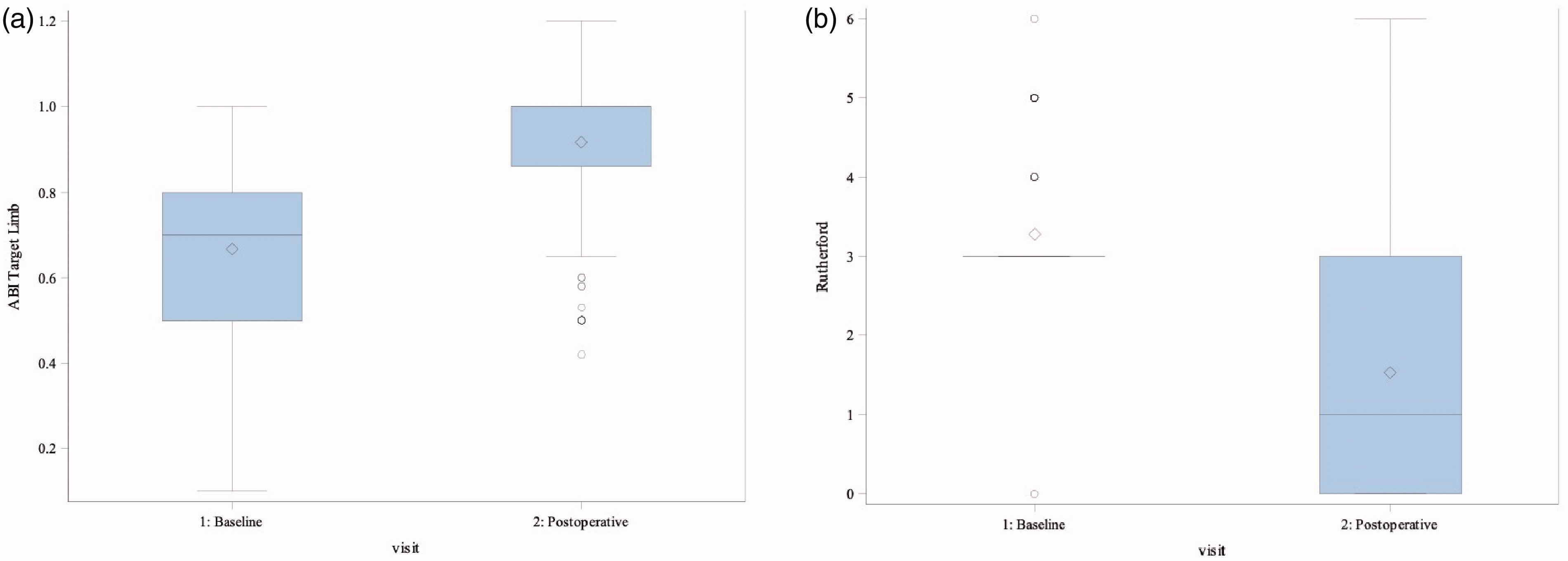
Ankle Brachial Index (ABI) and Rutherford classification at baseline and postoperatively. (a) Mean ABI was moderately impaired at baseline (0.66±0.19 [95% CI: 0.64; 0.69], evaluated in 179 lesions) and improved to normal values post procedure (0.90±0.16 [95% CI: 0.88; 0.93], evaluated in 205 lesions). (b) At baseline, only 0.5% of patients had less than severe claudication. Median, Q1 and Q3 were identical as 78.6% had Rutherford class 3, 9.3% class 4, 7.1% class 5, and 4.4% class 6. Post-procedure, Rutherford class had improved with 70.3% having less than severe claudication (37.5% in Rutherford class 0, 21.9% in class 1, 10.9% in class 2, 17.2% in class 3, 6.3% in class 4, 4.7% in class 5 and 1.6% in class 6). The whiskers present the first to third quartile, the band the median, the crystal the mean, and the end of the whisker maximum and minimum values. Outliers (distance of more than 1.5*IQR from the box) are marked in circles.

Kaplan–Meier estimate of survival. Kaplan–Meier survival plot, indicating the number of events and patients at risk at the respective time points.
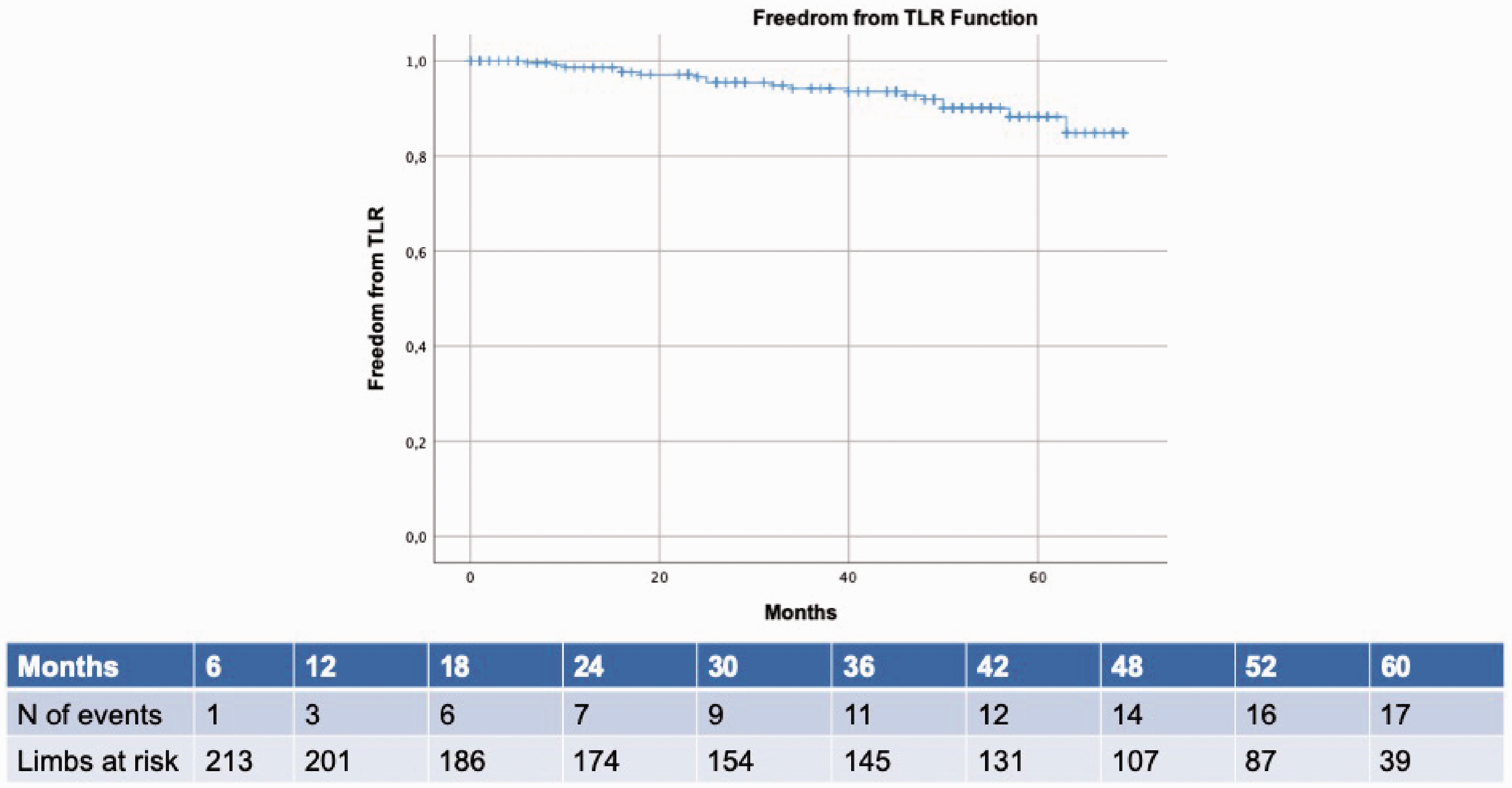
Kaplan–Meier estimate of freedom from target lesion revascularization. Kaplan–Meier plot, indicating the number of events and patients at risk at the respective time points.
Stent fractures were seen in three lesions (1.3%), thereof one was caused by the catheter during stenting of a renal artery, a new Dynamic stent was implanted as corrective action. Another stent was deformed during thrombectomy, and one stent was fractured during the procedure and pulled in the external iliac artery (EIA) by the balloon catheter.
Discussion
Iliac artery stenting in stenoocclusive disease is considered as the standard of care in many cases. 6 Numerous devices are available on the market, ranging from self-expanding stents 7 over balloon-expandable stents 12 to balloon-expandable stent-grafts. 14 The BIODYNAMIC registry assesses the safety and performance of the Dynamic balloon-expandable stent for treatment of iliac artery stenotic disease. The present study demonstrates technical and clinical success of this device, with a freedom from TLR and major limb amputation rate of 96.2% at 12 months. With six (2.6%) target lesion revascularizations, the results of this device correspond well with the TLR rates presented in the literature, ranging from 3.0% to 6.9%. 7 The freedom from TLR at 12 months (97.4%) is in line with other balloon-expanding stents with rates from 87.0% to 94%.3,5,7,12–14
In our eyes, this study adds two important aspects to the current body of evidence. First, the mean length of follow-up in this study is 39.5 months, with five-year data available for 31 patients. Few trials have reported mid- to long-term data. The iCAST trial reported a freedom from TLR of 86.6% at three years (84.7% in the intention-to-treat population). 15 The post hoc analysis of the COBEST trial with a five-year follow-up did not report TLR rates, but primary patency rates of 74.4% for stent-grafts and 62.9% for bare metal stents. 16 However, the results from both trials were on short lesions, treated with older-generation stent designs.
The second important aspect of this study is that it presents results of iliac artery stenting in more advanced PAD. In the present series, 11.5% of patients were Rutherford class 5 and 6, whereas most studies only include patients with Rutherford class up to 4. 5 , 7 , 12 , 13 While it might be hypothesized that this unfavorable disease burden would lead to higher amputation rates, the present study population target limb amputation rate is 1.3%, with all amputations in patients with extensive disease above and below the knee. In the literature, reported target limb amputation rates vary between 0% 7 and 10%. 14 Retrospective studies report higher amputation rates, hypothetically because prospective study inclusion protocols sought to exclude extensive occlusive disease.
Lesions were located in the CIA, reflecting the use of balloon-expandable stents in clinical routine. As balloon-expandable stents provide a high radial force and allow a precise placement, they are well suited for the CIA which is frequently calcified and prone to recoil. On the other hand, self-expanding stents play a larger role in the more tortuous EIA as they have a better conformability, preventing circumferential stress which potentially promotes neointimal hyperplasia.8,17,18 Likewise, the recent ICE trial that randomized patients with CIA or EIA lesions to either the balloon-expandable Visi-Pro stent or the self-expanding Protégé (both Medtronic), showed superior binary restenosis rates in the overall population for self-expanding stents, but not in patients with CIA lesions or heavily calcified lesions.7,17 A recent single center retrospective analysis also showed that balloon-expandable stents are mainly implanted in the CIA whereas self-expanding stents are mainly implanted in the EIA. With that distinction, in contrast to the ICE trial, balloon-expandable stents had even better patency rates as self-expanding stents, albeit confounded by the fact that the EIA itself has a higher risk of restenosis. 13
Mean stented lesion length was < 5 cm and thus within the current guideline recommendation for endovascular first strategy, 6 also reflecting outcomes of clinical studies such as COBEST and VISIBILITY that show superior results of covered stents compared to bare metal stents in long and complex lesions, but not in shorter and less complex lesions.12,16 In general, covered stents have the advantage of preventing intimal growth over the stent surface, minimizing the risk of in-stent restenosis, but also bear the risk of stent thrombosis and should therefore be reserved for severe cases. 8
Limitations
BIODYNAMIC has limitations inherent to retrospective single center studies. Neither a clinical events committee nor a core laboratory assessed the patients. Follow-up ABI and PSVR were not recorded for the long-term follow-up. These parameters would have been important to compare outcomes across studies. On the other hand, the retrospective design allows to evaluate subjects without limiting exclusion criteria, representing a real-world population treated according to our local practice.
Conclusion
The Dynamic balloon-expandable stent system has been exclusively used in the common iliac artery. In this indication, despite a high Rutherford classification at baseline, the Dynamic stent has proven to be safe with very good patency rates at 12 months. Longer term outcomes show the sustainability of outcomes at long-term follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BD receives consultancy fees from Biotronik. GFT, KD, BB, GBT, and EB have no relevant conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by BIOTRONIK AG, Buelach, Switzerland.