
Abstract
Objectives
The involvement of myeloperoxidase in the production of dysfunctional high-density lipoproteins and oxidised biomolecules leads to oxidative stress in the blood vessel endothelium. This prospective cohort study aimed to examine the prognostic value of myeloperoxidase in patients with peripheral artery disease in relation to major adverse cardiac events (MACEs), target lesion revascularisation, and major adverse limb events (MALEs) and its association with multi-bed vascular disease, which is defined as any combination of the following: peripheral artery disease and coronary artery disease.
Methods
Myeloperoxidase levels were measured in patients with peripheral artery disease and coronary artery disease during angiography. A total of 94 patients were analysed and followed up regarding their MACEs, target lesion revascularisation, and MALEs from August 2016 until February 2019.
Results
Among patients with peripheral artery disease, the rates of MACE and mortality were higher in patients with high myeloperoxidase levels than in those with low myeloperoxidase levels; the myeloperoxidase levels were 3.68 times higher in these patients (p < 0.0001). Patients with peripheral artery disease and coronary artery disease (multi-bed vascular disease) had higher myeloperoxidase levels than those with only peripheral artery disease and only coronary artery disease (one-bed vascular disease). Peripheral artery disease patients with higher myeloperoxidase levels had significantly higher rates of limb ischaemia, requiring further revascularisation than those with low myeloperoxidase levels.
Conclusions
High myeloperoxidase levels suggest poor outcomes and are associated with MACE and limb ischaemia. Our findings indicated that myeloperoxidase levels could become a prognostic marker and may be used in conjunction with other methods for risk stratification in patients with peripheral artery disease and multi-bed vascular disease.
Keywords
Introduction
Myeloperoxidase (MPO) is a leukocyte enzyme mainly found in neutrophil granulocytes, and it comprises part of a host’s innate defence. 1 As MPO is the most abundant enzyme in the azurophilic granules of neutrophilic granulocytes, it is also found in monocytes and other tissue macrophages, including liver “Kupffer cells”, 2 and the central nervous system, including microglia. 3 MPO accounts for up to 5% of the total protein in monocytes and neutrophilic granulocytes.1,4
Besides its immunological role, MPO contributes to atherogenesis2,5 by generating highly reactive oxygen species, including oxidised low-density, dysfunctional high-density, and nitro-low-density lipoproteins, which are ligands for scavenger receptors, causing foam cell formation.3,6 MPO provokes endothelial dysfunction by reducing nitrogen dioxide levels; several studies have revealed that elevated MPO levels are an independent predictor of cardiac events.1,2
Zhang et al. 4 were among the first to postulate that elevated MPO and leukocyte levels are associated with higher coronary artery disease (CAD) severity. Subsequent studies have shown that MPO concentrations change according to different CAD stages.7–10 Heslop et al. 7 specified that the MPO concentration was an indicator of the long-term prognosis for cardiac events.
Peripheral artery disease (PAD) is associated with higher mortality rates and more frequent reinfarction and considered a risk factor for major adverse cardiac events (MACEs). 11 Kang et al. 12 suggested that PAD is an independent risk factor for negative outcomes in patients with cardiac events. However, PAD remains underdiagnosed, undertreated, and poorly understood.
In this study, we aimed to evaluate the prognostic potential of the MPO concentration in patients with PAD in relation to MACEs, target lesion revascularisation (TLR), and major adverse limb events (MALEs). Moreover, we examined its association with multi-bed vascular disease, which is defined as any combination of the following: PAD and CAD. Our goal was to identify patient groups with a particular risk and improve the surveillance and risk stratification.
Material and methods
Inclusion and exclusion criteria
Between August 2016 and February 2019, 104 patients referred for vascular assessments for PAD at the angiology outpatient clinic were enrolled. The inclusion criteria were as follows: age ≥18 years, provision of written informed consent, visit to the outpatient clinic for vascular assessment, presence of symptomatic PAD, and diagnosis of PAD and CAD. Patients with incomplete CAD or PAD history data, those who did not provide written informed consent, and those already included in other interventional studies were also excluded. Ninety-four patients were finally enrolled.
Study population
Patients (n = 94) were assigned to one of three groups based on the presence of PAD (n = 27), CAD (n = 16), or multi-bed vascular disease (n = 51). Subsequently, all patients with PAD (PAD and CAD+PAD; n = 78) underwent a peripheral angiography. Patients who exhibited haemodynamically non-significant stenosis or adequate collateralisation as per angiography (n = 12) underwent DSA only and did not require further revascularisation. Patients with a need for angioplasty (n = 66) required revascularisation, which involved stenting or balloon angioplasty. Patients with CAD only (n = 16) were qualified and included in this group based on the coronary angiographic results and CAD symptoms (Figure 1).
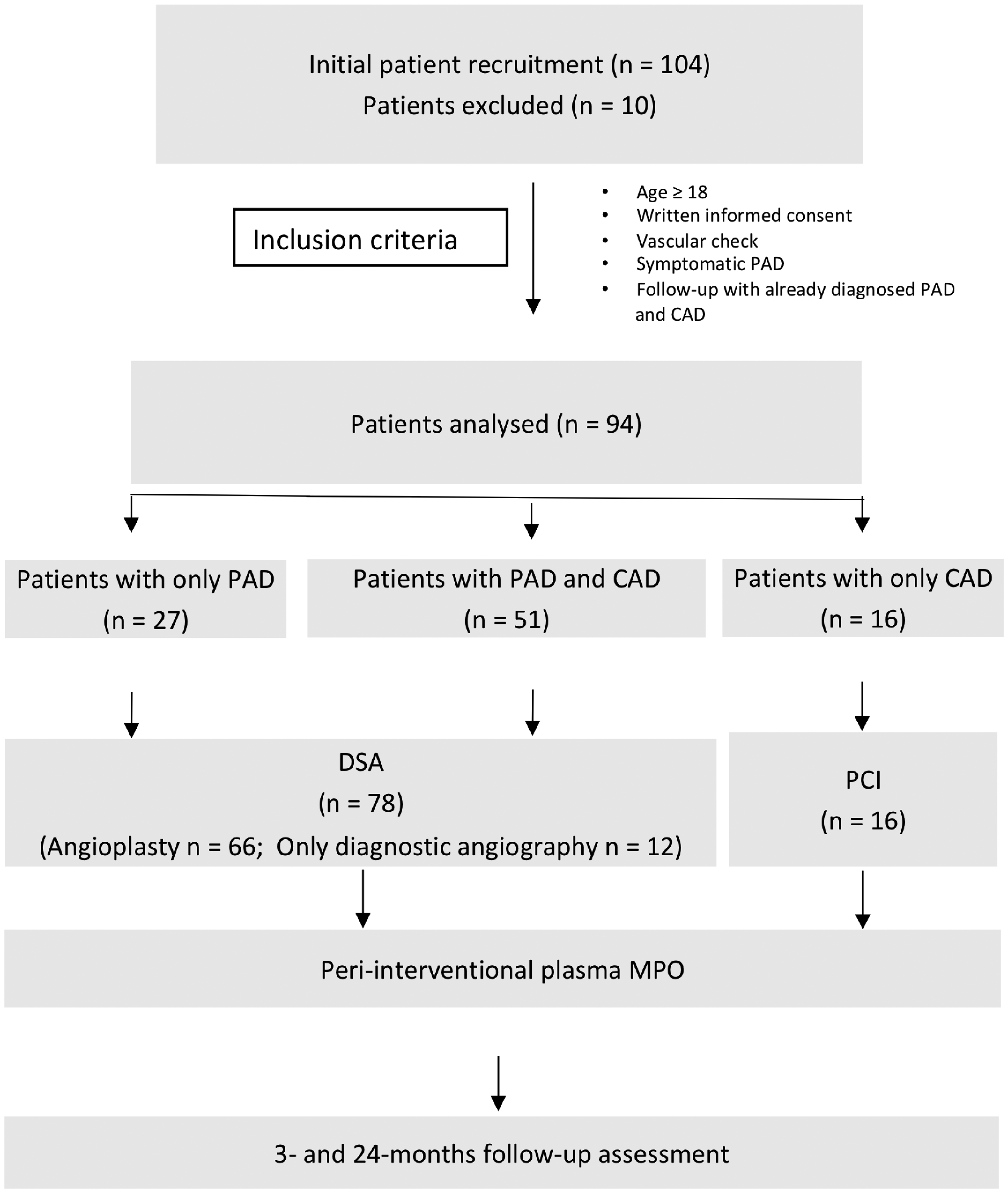
Study flowchart. PAD: peripheral artery disease; CAD: coronary artery disease; MPO: myeloperoxidase; FU: follow-up.
A patient with multi-bed vascular disease was defined as a patient with both PAD and CAD. PAD was confirmed based on an ankle–brachial index (ABI) of ≤0.9, duplex sonographic findings, clinical findings (Rutherford stage), and treadmill test results; all these assessments were performed as part of the standard care of patients with PAD scheduled for percutaneous transluminal angioplasty. Patients were classified into the following three groups using the Rutherford classification: PAD stage I group, patients with Rutherford category 0 disease; PAD stage II group, patients with Rutherford category 1–3 disease; and PAD stage III, patients with Rutherford category 4–6 diseases.
Serum MPO levels were measured in the blood samples collected during digital subtraction angiography (DSA). All patients were prospectively followed for the occurrence of MACEs and MALEs. MACE was defined as an unscheduled coronary revascularisation procedure (including ST-segment elevation myocardial infarction and non-ST-segment elevation myocardial infarction), stroke, or rehospitalisation for any cardiac reasons. MALE was defined as acute or acute-on-chronic limb ischaemia and included all major amputations in this analysis. Major amputation was defined any amputation above the ankle. Acute limb ischaemia was defined as limb-threatening ischaemia confirmed from a limb’s haemodynamic parameters or imaging, which led to early reintervention, including peripheral artery surgery/reconstruction, peripheral angioplasty/stenting, or amputation. Chronic limb ischaemia was defined as follows: ongoing ischaemic limb, foot, or digit pain that led to hospitalisation; an intervention that did not fulfil the definition of acute limb ischaemia; and presence of Rutherford category 4, 5, or 6 at baseline and use of peripheral vascular interventions during the study.
Sample collection and processing
After arterial puncture, blood was collected in two monovettes (7.5 mL) containing 12 mg ethylenediaminetetraacetic acid (EDTA) and a serum clot activator gel. Within 1 h, the samples were centrifuged at 1811g (relative centrifugal force) at a temperature of 21°C for 10 min, the supernatants were pipetted into 1.5-mL Eppendorf tubes, and the samples were stored at −80°C before analysis.
To investigate the prognostic potential of MPO, blood was collected before DSA, and MPO levels were measured using a human MPO ELISA kit (ab119605; Abcam, Cambridge, UK) according to the manufacturer’s instructions. The washing buffer comprised 0.01-M phosphate-buffered saline at pH 7.2–7.6, sodium chloride (8.5 g), disodium hydrogen phosphate (1.4 g), and sodium dihydrogen phosphate monohydrate (0.2 g) in distilled water (1 L). The serum and EDTA samples were diluted at a ratio of 1:50 and 1:5, respectively. Each sample was analysed in duplicate, and the final MPO concentration in a sample was calculated as the mean of both measurements. Interleukin (IL)-6 and C-reactive protein (CRP) levels were measured using an electrochemiluminescence immunoassay and nephelometry, respectively, at the hospital centre laboratory.
Statistical analyses
All statistical analyses were conducted using Microsoft Excel for Office 365®, 2018 (Redmond, WA, USA), IBM® SPSS® version 22.0 (IBM Corporation, Armonk, NY, USA), and GraphPad Prism® version 6.02 (GraphPad Software Inc., La Jolla, CA, USA). Normally and non-normally distributed data are expressed as means and standard deviations (SD) and medians and interquartile ranges (Q1–Q3), respectively. The Kolmogorov–Smirnov and Shapiro–Wilk tests were used to assess the normality of distribution of continuous variables. Variance analyses using the t-test were performed for normally distributed variables. When more than two groups were analysed, one-way analysis of variance (ANOVA) was performed using the GraphPad Prism® software, followed by post hoc tests (Tukey’s multiple comparisons or Fisher’s exact test). Pearson’s correlation coefficients were calculated, and significance analyses were performed. The relative risk was calculated using a two-by-two contingency table. GraphPad Prism® was used to identify outliers using the ROUT method, and the Q co-efficient was set at 1%. A p-value of <0.05 was considered statistically significant.
Ethical considerations
All data were fully pseudo-anonymised prior to access and analysis. This study was approved by the local ethics committee and conducted in accordance with the Declaration of Helsinki. Interventions were conducted only with the understanding and consent of each patient and for any relevant, medically appropriate care that should be provided in emergencies. All patients provided written informed consent before enrolment.
Results
Study population
Table 1 presents the patients’ baseline characteristics. Data for 94 patients (sex, 62 men and 32 women, mean age, 69.7 ± 9.67 years) were analysed. The patients were assigned to three groups according to the presence of PAD only, CAD only, and two-bed vascular PAD and CAD. In total, 82.9% (n = 78/94) had symptomatic PAD (28.7% with PAD only and 54.2% with two-bed vascular disease). An asymptomatic clinical stage was observed in 4.2% (n = 5) patients (Rutherford category 0, Fontaine I), whereas 56.3% (n = 53) and 21.2% (n = 20) patients had mild-to-moderate (Rutherford categories 1–3, Fontaine II) and severe (Rutherford categories 4–6, Fontaine III–IV) PAD, respectively (Table 1, Figure 1).
Patients’ baseline clinical characteristics.

Note: Data are expressed as frequencies and percentages or means and standard deviations. The p-values refer to comparisons between patients with PAD or CAD only and those with polyvascular disease.
ABPI: ankle–brachial pressure index; ACE: angiotensin-converting enzyme; ADP: adenosine diphosphate; ASS: acetylsalicylic acid; AT: angiotensin; CAD: coronary artery disease; CRP: C-reactive protein; DM: diabetes mellitus; GFR: glomerular filtration rate; IL-6: interleukin 6; MPO: myeloperoxidase; NOACs: new oral anticoagulants; PAD: peripheral artery disease; PAD I: Rutherford 0; PAD II: Rutherford 1–3; PAD III: Rutherford 4–6.
There were no between-group differences in the proportion of patients with diabetes mellitus (DM), hypertension, current or past smoking habits, and hyperlipidaemia (Table 1). Patients with two-bed vascular disease had a higher rate of DM (43.1%) and renal insufficiency (52%), with a glomerular filtration rate of 69–21 mL/min, than did those with isolated PAD or CAD (DM: PAD only, 29.6%; CAD only, 12.5%; p = 0.3158; renal insufficiency: PAD only, 33.3%; CAD only, 35.7%; p = 0.0479).
The groups did not differ with respect to the use of antithrombotic, anticoagulant, antihyperlipidaemic, and antidiabetic drugs. Patients with CAD only were more likely to receive β-blockers, aldosterone receptor antagonists, and diuretics as daily medications (Table 1).
We also analysed the correlation of MPO levels with acetylsalicylic acid (ASS) or DM. Patients with ASS had a non-significant higher level of MPO than did those without ASS (461.1 ± 347.8 ng/ml vs. 322.9 ± 205.2 ng/ml; p = 0.171). Moreover, the presence of DM did not influence MPO levels (with DM, 531.0 ± 397.8 ng/ml vs. without DM, 428.9 ± 313.9 ng/ml; p = 0.309). Altogether, 12.7% (n = 12/94) patients did not require revascularisation or stenting and only underwent diagnostic angiography, which was based on a well-collateralised lesion in the index leg; thus, there was no further need for revascularisation. The rate of percutaneous transluminal angioplasty and revascularisation was 70.2% (n = 66/94). Multi-bed vascular disease (>1 vessel bed, PAD, and CAD) and PAD only were observed in 54.2% (n = 51/94) and 28.7% (n = 27/94) patients, respectively (Figure 1).
The proportion of patients who had typical symptoms of CAD (angina, dyspnoea, or pathological electrocardiogram with signs of ischaemia) and underwent elective coronary angiographies was 17.1% (n = 16/94); these patients comprised the CAD group.
Follow-up consultations were held at 3 and 24 months after angioplasty. The mean and median follow-up times for the overall cohort were 17.9 ± 9.6 and 23 ± 8.9 months, respectively. In the PAD only and CAD only groups, the mean follow-up time was 23.7 ± 6.76 and 8.4 ± 0.63 months, respectively (p ≤ 0.0001). The follow-up time for patients with CAD was short because of late recruitment of this group into the study.
MPO levels
Patients with two-bed vascular disease (PAD+CAD) had higher mean MPO levels (627.3 ± 531.9 ng/mL) than did those with PAD (425.2 ± 331.3 ng/mL) or CAD (347.2 ± 207.5 ng/mL) only. ANOVA showed that the presence of both PAD and CAD could lead to slightly higher MPO levels (p = 0.0388) (Figure 2). This result could be verified by Fisher’s Least Significant Difference test (CAD only vs. both PAD and CAD, p = 0.0289), but not by the multiple comparison test after Tukey’s test.
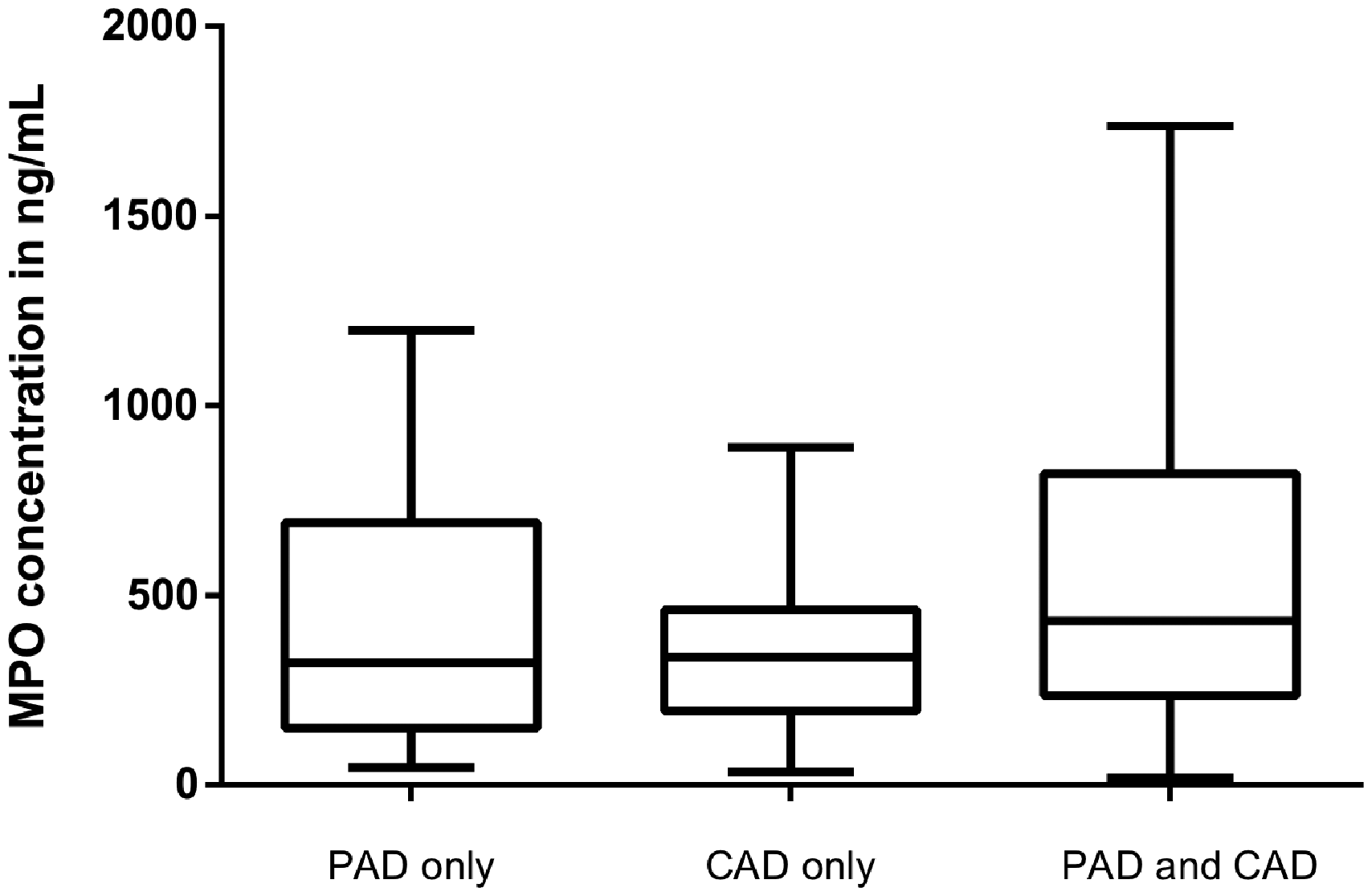
MPO levels in patients with PAD only, CAD only, and both PAD and CAD. The MPO level is significantly higher in patients with both PAD and CAD (n=51; 627.3 ± 531.9 ng/mL) than in those with PAD (n=27; 425.2 ± 331.3 ng/mL) or CAD (n=16; 347.2 ± 207.5 ng/mL) only (p=0.0289). CAD: coronary artery disease; MPO: myeloperoxidase; PAD: peripheral artery disease.
Prognostic potential of MPO
The mean MPO levels were higher in the group requiring revascularisation (746.8 ± 542.8 ng/mL) than in the group not requiring revascularisation (377.2 ± 202.9 ng/mL) (Figure 3). Considering that the latter group was very small, with only 12 patients not requiring further intervention, we could only assume the potential benefit of this finding.
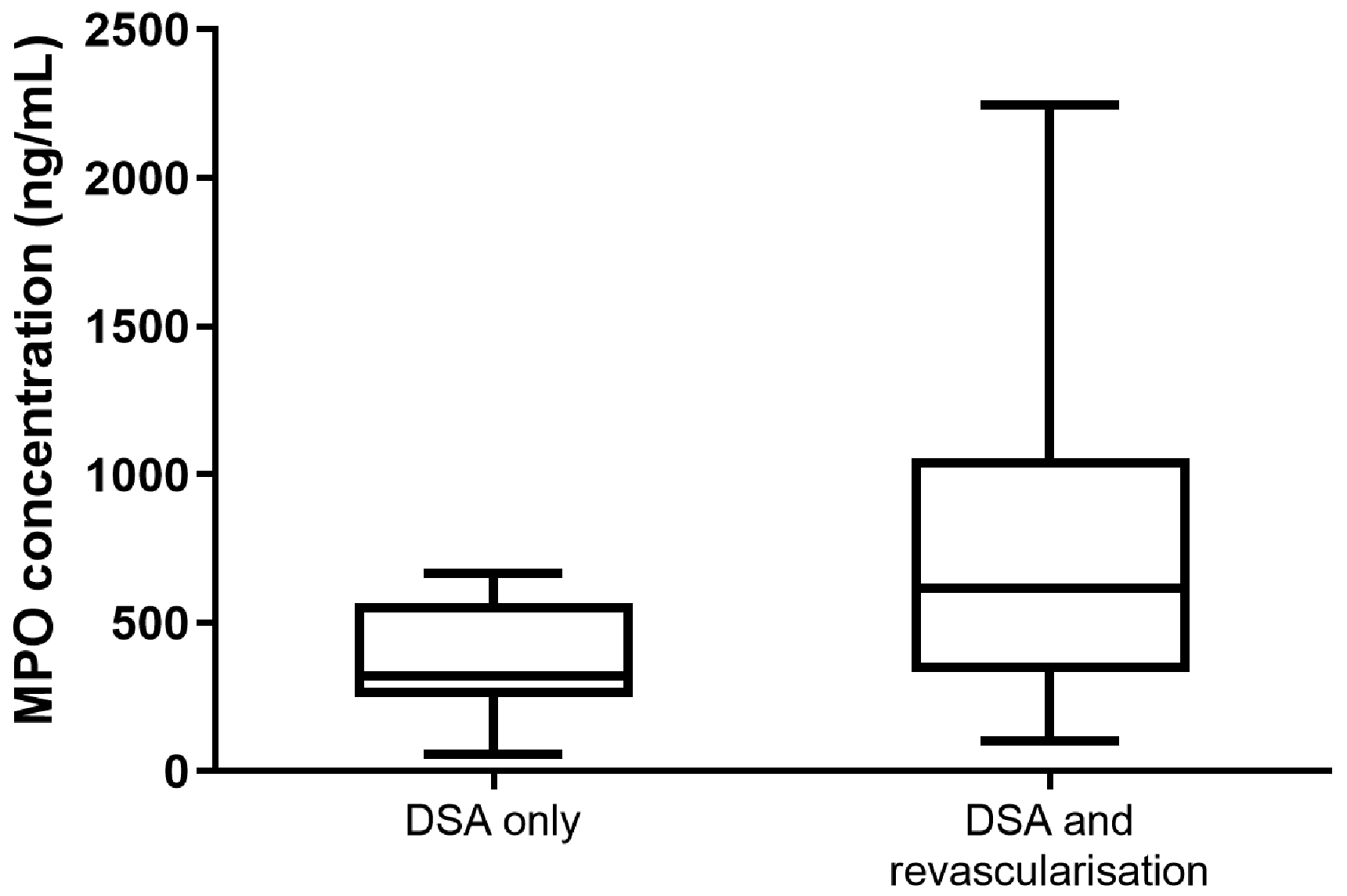
MPO concentrations in patients undergoing DSA without revascularisation and patients requiring revascularisation. The MPO level is higher in patients who underwent revascularisation (n = 66; 746.8 ± 542.8 ng/mL; median, 616.9 ng/mL) than in those without revascularisation (n = 12; 377.2 ± 202.9 ng/mL; p = 0.006). DSA: digital subtraction analysis; MPO: myeloperoxidase.
Patients with initially higher MPO levels had a trend towards higher MACE and MALE rates than did those with lower MPO levels (Figure 4). In the PAD only group, patients with MACE and MALE had higher serum MPO levels than did those without such adverse events (p < 0.0001) (Figure 5). The mean±SD MPO level was 3.68 times higher in patients with MACE than in patients without MACE or MALE (1067 ± 156.4 vs. 290.1 ± 206.4 ng/mL). The mean±SD MPO level was 1.48 times higher in patients with MALE than in patients without TLR or MALE (429.3 ± 250.5 ng/mL vs. 290.1 ± 206.4 ng/mL) (Figure 5).

MPO levels in patients with MACE (n = 13), MALE (n = 7), and TLR (n = 10) and patients without such events (n = 27). The boxplots show the minimum, maximum, and median MPO levels and the 25th and 75th percentiles. Patients without cardiac or vascular events show the lowest MPO levels. Patients with MACE show the highest MPO levels. MPO: myeloperoxidase; MACE: major adverse cardiac events; MALE: major adverse limb events; TLR: target lesion revascularisation
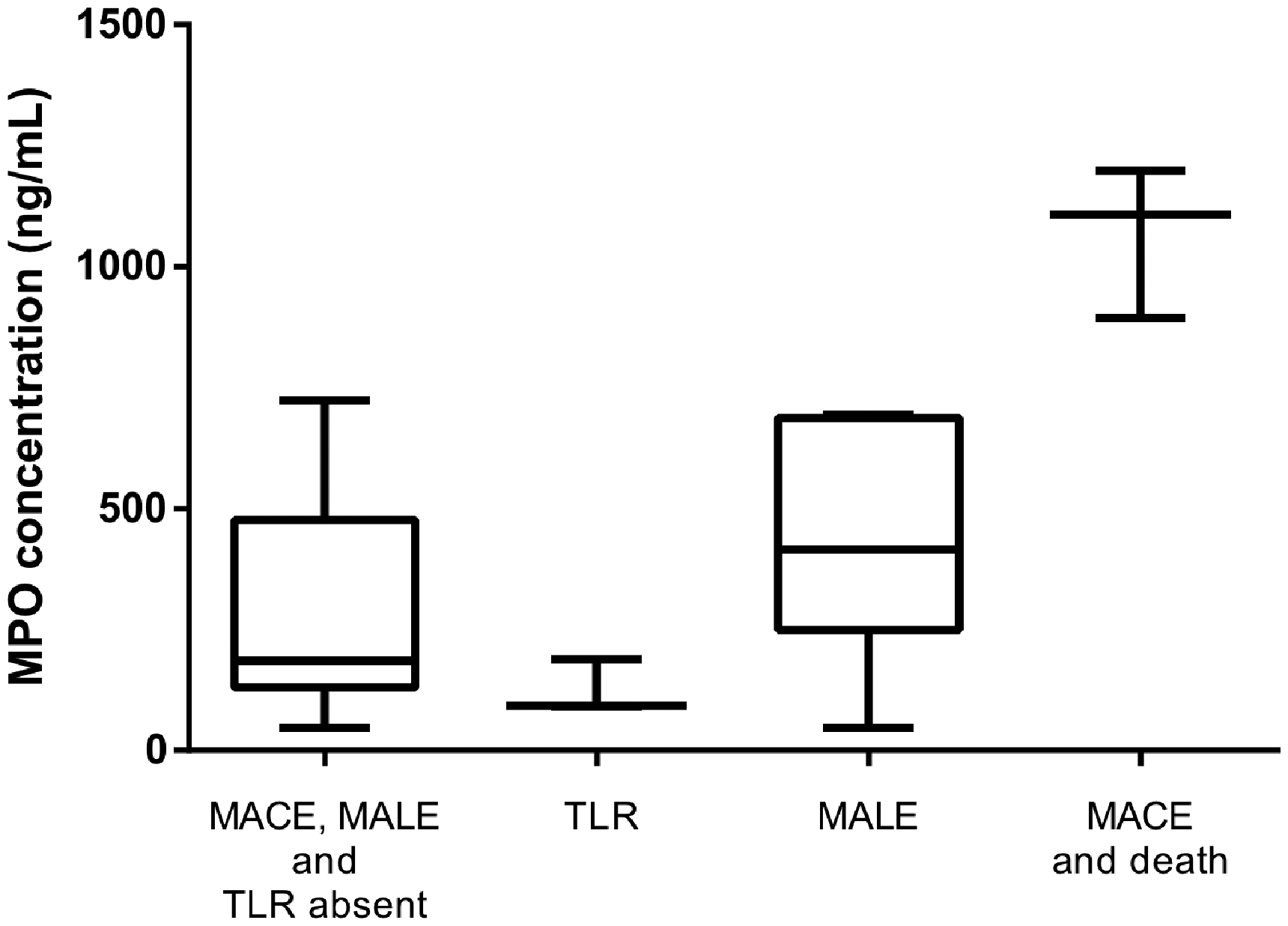
MPO levels in patients with PAD only, with or without (n = 13) MACE (n = 3), MALE (n = 6), and TLR (n = 3). The box plots show the maximum, minimum, and median MPO levels and the 25th and 75th percentiles. The MPO level is 3.68 times higher in patients with MACE than in those without MACE or MALE (1067 ± 156.4 ng/mL; median, 1108 ng/mL vs. 290.1 ± 206.4 ng/mL; median, 185.4 ng/mL), and 1.48 times higher in patients with MALE than in those without TLR or MALE (429.3 ± 250.5 ng/mL; median, 416.2 ng/mL vs. 290.1 ± 206.4 ng/mL; median, 185.4 ng/mL). MPO: myeloperoxidase; MACE: major adverse cardiac events; MALE: major adverse limb events; TLR: target lesion revascularisation
Correlations between MPO levels and inflammatory markers
In the total patient cohort, MPO levels did not correlate with leukocyte (r = 0.124; p = 0.336) or IL-6 levels (r = −0.007; p = 0.958), and the relationship between MPO and CRP levels was not significant (r = 0.0413; p = 0.752) (Figure 6).
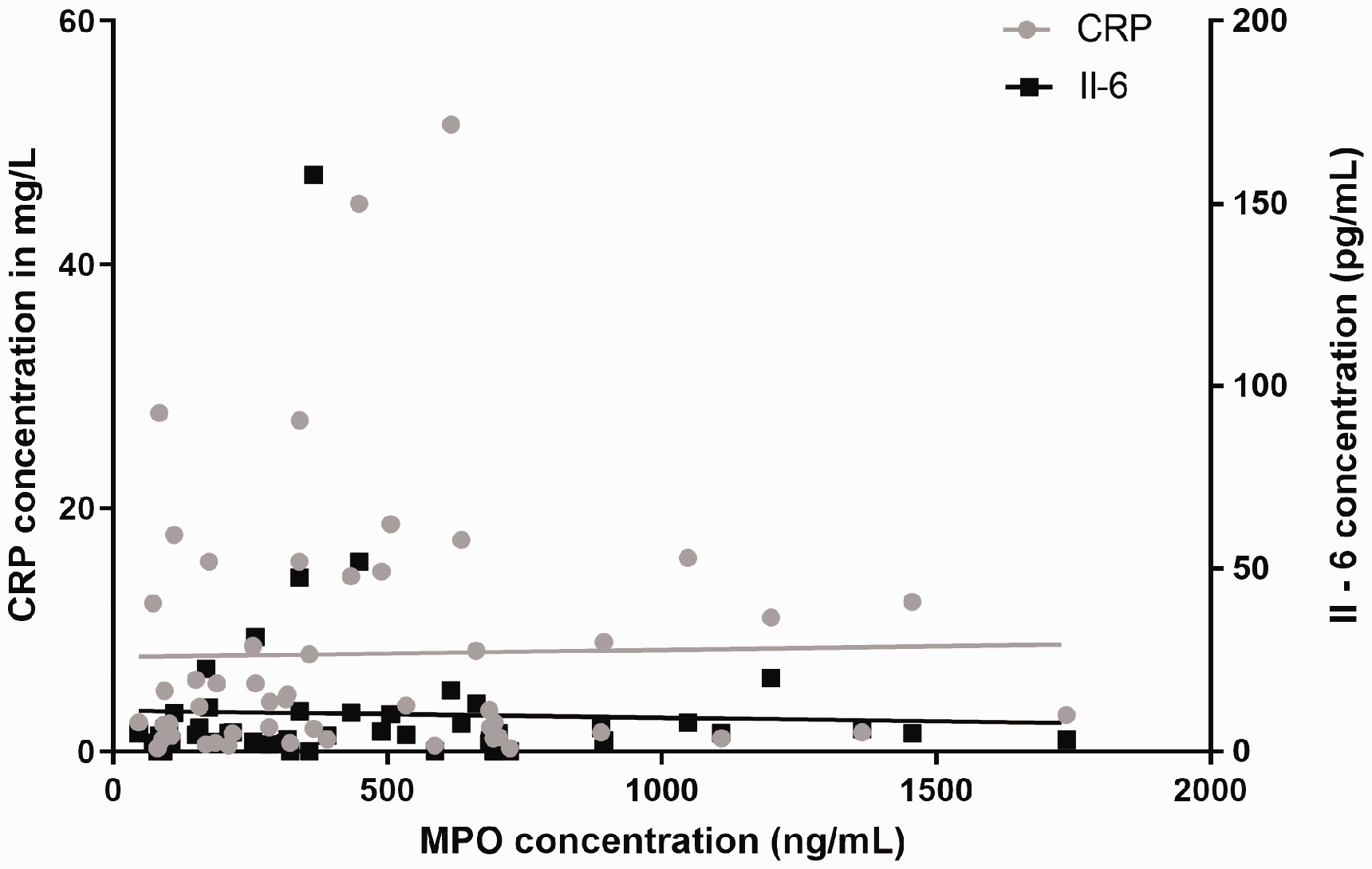
Associations between MPO levels and CRP and interleukin-6 concentrations. CRP: C-reactive protein; IL-6: interleukin 6; MPO: myeloperoxidase
Correlations of MPO levels with different PAD stages and ABI
Serum MPO levels were measured at different PAD stages based on Rutherford categories and ABI. The association between the MPO concentration and PAD stage was not significant (p = 0.3425) and could not be stratified. The highest (674.9 ± 332.9 ng/mL) and lowest (425.3 ± 296 ng/mL) mean MPO concentrations were observed in patients with Rutherford category 0 (n = 5) and 4–6 (n = 20) diseases, respectively. The mean±SD MPO concentration was 478.9 ± 350.4 ng/mL in patients with Rutherford category 1–3 disease (n = 53) (Figure 7).
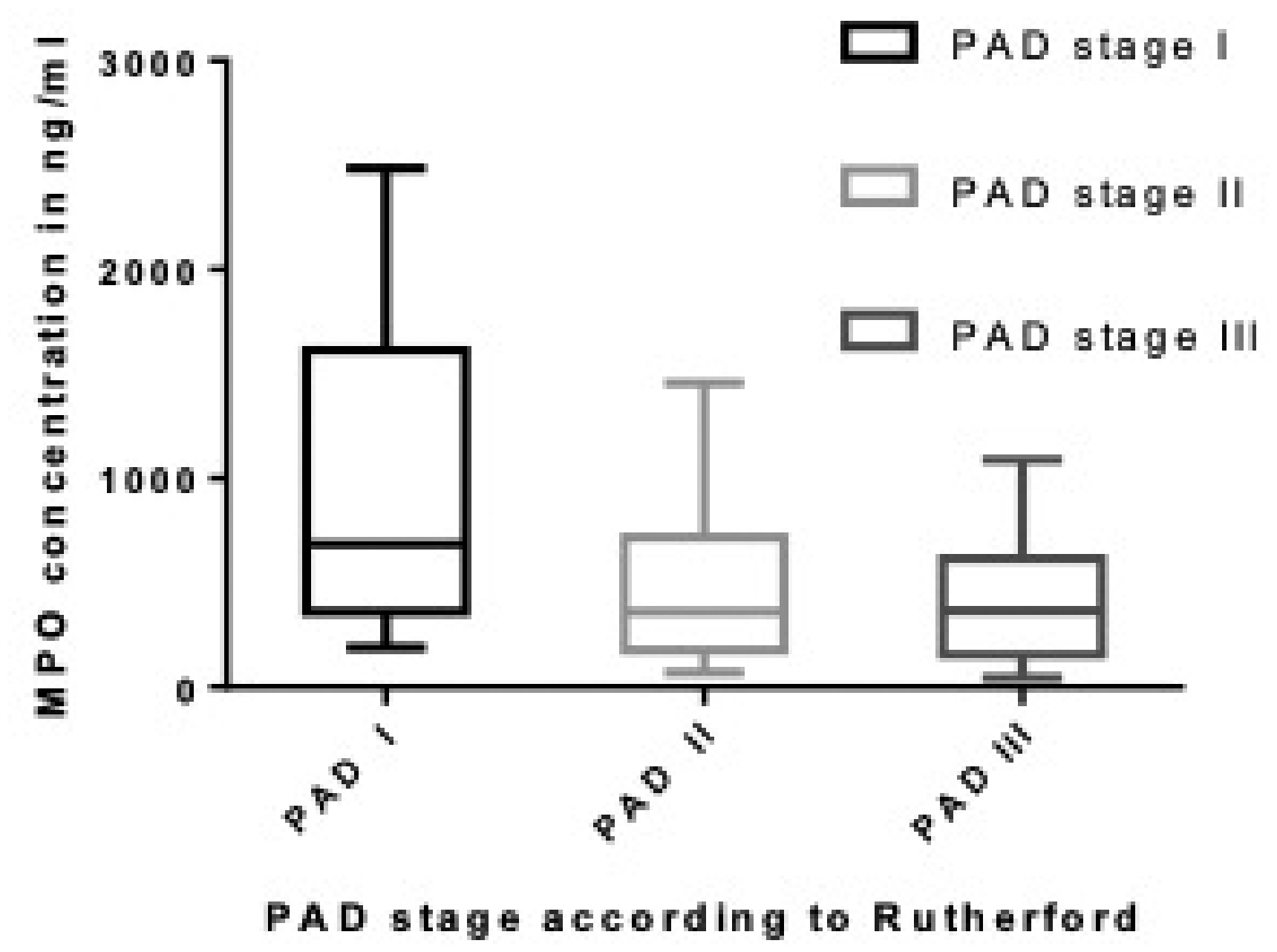
MPO concentration in relation to the PAD stage according to the Rutherford classification. The highest and lowest MPO concentrations are observed in patients with Rutherford category 0 (n = 5; 674.9 ± 332.9 ng/mL) and Rutherford category 4–6 (n = 20; 425.3 ± 296 ng/mL) diseases, respectively. The mean MPO concentration is 478.9 ± 350.4 ng/mL in patients with Rutherford category 1–3 disease (n = 53). MPO: myeloperoxidase; PAD: peripheral artery disease.
Patients were further categorised into the following groups according to an ABI of 0.90–0.5 and <0.5. MPO levels did not differ between groups (p = 0.3261); a lower ABI showed a slight increasing trend with increasing MPO levels, albeit without any significantly correlation (r = −0.093; p = 0.572) (Figure 8).
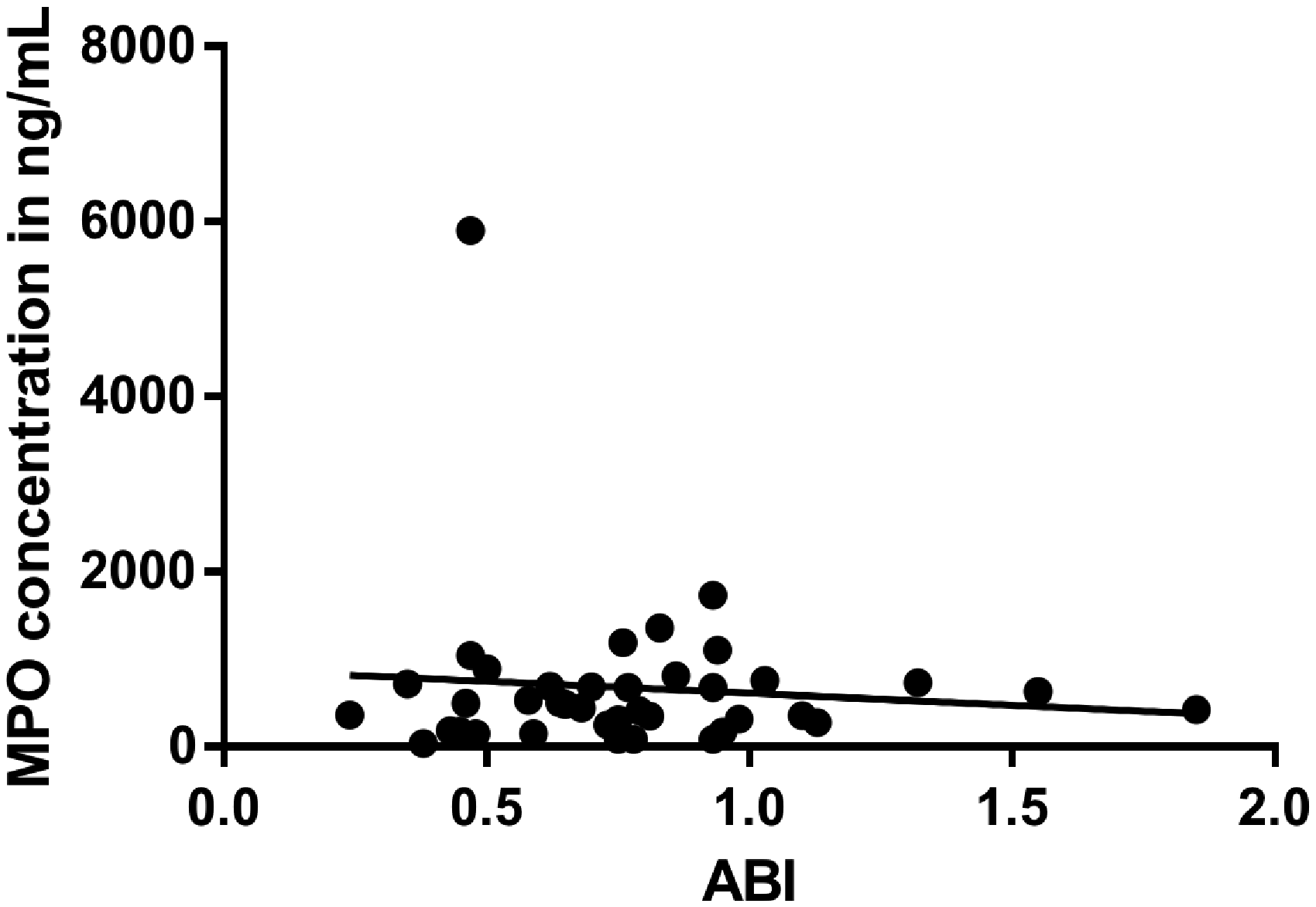
Correlation of MPO concentrations with ABI values. A lower ABI value showed a slight increasing trend with increasing MPO levels, but this was not significantly correlated (r = −0.093; p = 0.572). ABI: ankle–brachial index; MPO: myeloperoxidase.
Discussion
Studies have indicated that MPO concentrations change according to different CAD stages.7–10 To our knowledge, this is the first study to examine the prognostic potential of MPO levels in patients with symptomatic PAD in relation to MACE, TLR, and MALE, and to evaluate the association between MPO levels and multi-bed vascular disease.
Our results indicated that MPO levels could be used as a biomarker for risk stratification of patients with PAD. Initial MPO levels were higher in patients who required further revascularisation than in those who did not. As the latter group comprised only 12 patients, these results should be analysed in bigger trails. However, Haslacher et al. 13 showed that patients with PAD and higher MPO levels had a high risk of MACE, demonstrating the predictive value of MPO levels. Among patients with PAD only, those who experienced MACE or MALE had significantly higher MPO levels.
Patients with atherosclerosis may have higher inflammatory activity. Berger et al. 14 showed that patients with PAD had higher MPO levels than did those without PAD. The findings of several studies have indicated that inflammatory protein levels are higher in patients with CAD or PAD than in healthy individuals.14–20 Ye et al. 15 showed that inflammatory proteins, including CRP, IL-6, and MPO, were elevated in African-American patients with lower ABI values. Furthermore, Zhou et al. 16 reported high CRP levels in patients with PAD. Our study indicated a numerical association between CRP and MPO levels; however, there was no significant correlation between MPO and IL-6 levels or ABI in our cohort. This could be explained by our small cohort comprising patients with low-grade and stable PAD. Patients with polyvascular diseases had higher MPO levels than those with CAD or PAD only; therefore, MPO levels might indicate a patient’s plaque load, which may explain why among patients with PAD, those with higher serum MPO levels were most at risk of MACE and MALE.
As inflammation itself also causes atherosclerosis, high inflammatory activity could lead to a vicious self-perpetuating circle. 21 This could partially explain the poor outcomes of patients with PAD and CAD who had higher MPO levels, which aligned with previous findings. 1 , 19 , 20 Baldus et al. 19 showed that MPO levels had a high predictive potential in relation to cardiac events. Ali et al. 20 also showed that higher MPO levels were accompanied by a higher risk of adverse cardiac events. Therefore, multi-vessel atherosclerosis may induce higher MPO levels, which may be associated with higher MACE and MALE risks and poor outcomes in patients with PAD. By contrast, different plaque loads and inflammation stages may have induced the wide range of MPO levels. This could partly explain why some patients with less severe PAD (e.g. Rutherford categories 0–3 and CAD) had higher MPO levels than those with more advanced PAD. We assumed that the high plaque burden, which does not cause any typical symptoms such as claudication, may be responsible for this finding. On the other hand, focal high-grade stenosis in a vessel causes more severe symptoms, even in the absence of a high plaque burden.
Ali et al. 20 analysed a cohort of patients with PAD and showed that combining the results from the assessments using clinical classification tools (e.g. the Rutherford classification) with laboratory-determined parameters improved patients’ risk stratification. Additionally, we ascertained that among the patients with PAD, there was a trend towards the risks of further revascularisation and MALE in patients with high MPO levels, rather than in those with low MPO levels. To our knowledge, this is a new finding, because recent studies have mainly focused on the patients’ cardiac outcomes.9,10,20 Considering that the study population was too small to conclude significant results, we can assume that MPO levels may suggest worse outcomes. They may also be helpful in conjunction with other methods, including detecting other manifestations of atherosclerosis in other vascular areas, and determining individual cardiac and vascular event risks among patients with unknown or early PAD. Moreover, they may be useful in identifying patients with higher MACE and MALE risks. 22
Positive correlations have been demonstrated between MPO and CRP levels.23,24 Correlations between MPO and IL-6 levels were not evident in our patients, partly because of the presence of mild PAD, rather than severe acute PAD, and the low generalised plaque burden. Despite these contradictory findings, MPO levels indicated worse outcomes for patients with PAD and could become an individualised risk marker for this group of patients.
Study limitations
This was a single-centre study that began in 2016, and only 94 patients were enrolled in 3–5 years because of the inclusion and exclusion criteria. Moreover, the SDs of MPO levels were rather wide and overlapping between the groups because of the small patient number. There was a statistically significant difference regarding the follow-up times between the PAD only and CAD only groups, severely limiting our conclusions. Regarding the outcome of the patients and the prognostic value of MPO, it would be useful to extend the follow-up period in larger future studies. Therefore, our findings should be validated in a larger multi-centre study. The proportions of patients with PAD were not well balanced in relation to the PAD severity because of the small sample size, and most patients had mild-to-moderate PAD, which may explain the absence of correlations between MPO levels, Rutherford categories, and ABI. Most patients with PAD had Rutherford category 1–3 disease, which may have led to under-representation of other PAD stages. To corroborate and generalise our results, larger studies with more patients with more severe PAD are required. Furthermore, different plaque load levels may have induced the wide range of MPO levels and high level of variation in MPO concentrations within groups. Further studies should analyse MPO levels and plaque or calcium scores.
Conclusions
Determining the concentrations of markers, including MPO, could be useful for identifying high-risk individuals and patients with PAD who require more aggressive management of cardiovascular risk factors. Serum MPO levels may predict an increased risk of cardiovascular events, further revascularisation, or MALE.
Footnotes
Acknowledgment
We thank Dr. Meghan Campbell (scientific coordinator at the Heart Centre Bonn, Bonn, Germany) for proofreading the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.