
Abstract
Background
There are limited data on outcomes for patients with peripheral artery disease undergoing endovascular revascularization by multi-disciplinary teams in a community hospital setting.
Methods
From January 2015 through December 2015, we assembled a multi-disciplinary program comprised of cardiologists, surgeons, radiologists, nurses, and administrative staff for managing patients with peripheral artery disease undergoing endovascular revascularization. Demographic, procedural, and outcomes data were collected with use of a template from the Society for Vascular Surgery Vascular Quality Initiative database. We compared characteristics and outcomes of patients with intermittent claudication and critical limb ischemia. We used Kaplan–Meier methods to estimate the rate of overall survival and freedom from rehospitalization between groups.
Results
After excluding patients with acute limb ischemia (n = 5), peripheral intervention to the upper extremity (n = 6), or abdominal aorta (n = 11), there were 82 patients in the study cohort; 45 had intermittent claudication and 37 had critical limb ischemia. Baseline and procedural characteristics were similar between groups, although critical limb ischemia patients were more likely to have hyperlipidemia (75.7% vs. 53.3%, P = .42). Procedural success was achieved in 91.3% of cases. Actionable access site bleeding occurred in 2.4% of patients. High rates of aspirin (91.5%) and statin (87.8%) were noted at discharge. After two years of post endovascular revascularization, survival was 57.5% for critical limb ischemia patients and 94.4% for intermittent claudication patients (P < .001). Freedom from rehospitalization was 32.7% for critical limb ischemia patients and 83.5% for intermittent claudication patients (P < .001).
Conclusions
We found that favorable outcomes may be achieved with a multi-disciplinary peripheral artery disease program at community hospitals. The incorporation of quality improvement practices may further help to develop standardized and regionalized approaches to care delivery for patients with peripheral artery disease.
Introduction
Peripheral artery disease (PAD) is an epidemic that affects nearly nine million in the US and is a costly growing problem among high-risk cohorts, with a prevalence nearing 30%. 1 The high burden of cardiovascular (CV) events in patients with PAD has been demonstrated irrespective of PAD symptom status, 2 highlighting the existing public health problem of this condition. Substantial advances in medical and endovascular therapy for the treatment of PAD have suggested important benefits for morbidity and quality of life 3 and have increased interest in conducting comparative effectiveness research and optimizing the quality of care for patients with PAD.
Given the highly prevalent nature of PAD, many patients are evaluated at regional hospitals, but little information is available on process measures and outcomes from community practice. Previous data suggested that lower volume endovascular PAD programs are associated with higher in-hospital mortality and postprocedural complications compared with higher volume centers; however, findings were limited by lack of follow-up. 4 Limited data are available on patient characteristics, treatment patterns, and long-term outcomes of patients with PAD who undergo endovascular therapy in a community program.
In this study, we evaluated the characteristics and outcomes of patients with intermittent claudication (IC) and critical limb ischemia (CLI) as part of our multidisciplinary vascular program. We sought to identify rates of guideline-recommended therapies and factors associated with long-term outcome among these high-risk patients.
Methods
From 15 January 2015 through 31 December 2015, we developed a multidisciplinary vascular quality improvement (QI) program to help improve the delivery of care to patients with PAD at Mayo Clinic Health System‒Franciscan Healthcare, a 142-bed community hospital in western Wisconsin. Patients with PAD were evaluated in the outpatient clinical practice of the surgery and cardiology departments. Biweekly multi-disciplinary conferences were conducted to review clinical history, objective testing, and endovascular approach to treatment. Prior to endovascular revascularization, patients were required to be on guideline-directed medical therapy as part of risk reduction. Among active smokers, revascularization was deferred for three months, while patients were referred to smoking cessation programs, provided pharmacotherapy targeting smoking cessation, or were provided literature on smoking cessation with instructions to identify a quit date. All endovascular procedures were performed in the angiographic suite in the cardiac catheterization lab at the hospital. We defined procedural success as acute technical success and absence of serious adverse events within 72 h of the procedure. We framed our database structure in keeping with the database of the Society for Vascular Surgery Vascular Quality Initiative (VQI) 5 and followed patients after revascularization for important clinical outcomes. The QI project was collaborative and multidisciplinary, incorporating clinician providers from various departments (surgery, interventional radiology, and interventional cardiology), nursing administrators, and allied health staff.
Baseline demographic variables included age, sex, race, hypertension, diabetes mellitus, smoking history, coronary artery disease, congestive heart failure, chronic obstructive lung disease, creatinine, functional status, prior peripheral vascular intervention (PVI), and preprocedural medications. Prior PVI was defined as any lower extremity revascularization (surgery or endovascular), aneurysm repair, major amputation, or prior carotid revascularization. Procedural characteristics included anatomical level of the clinically culprit lesion, the Trans-Atlantic Inter-Society Consensus Document on Management of Peripheral Arterial Disease (TASC) classification, treatment method (including angioplasty, atherectomy, and stenting), postoperative complications, and discharge medications. We assessed short-term events (30 days) and long-term outcomes. Events included death, myocardial infarction, stroke or transient ischemic attack, repeat revascularization, amputation, and any hospitalization longer than 48 h. All events were determined through review of medical records. If patients had clinical events at local centers, their records were reviewed to adjudicate clinical events. The study was approved (No. 18–005459) by the Mayo Clinic Institutional Review Board, and waiver of consent was obtained.
Continuous variables were summarized as mean (SD) and median (interquartile range [IQR]), and categorical variables were reported as frequency (percentage). Patient characteristics and outcomes were compared between the IC and CLI groups. Continuous variables were compared with the Wilcoxon rank sum test, and categorical variables were compared with the χ2 or Fisher exact test where appropriate. The Kaplan–Meier method was used to estimate the rate of overall survival and freedom from rehospitalization between the IC and CLI groups. Group comparisons were made with the log-rank test. The duration of follow-up was defined as the period from the procedural date to the last known date of follow-up or the date of the end point (death or rehospitalization). All tests were two-sided with the α level set at .05 for statistical significance.
Results
At our institution, 104 patients with PAD were treated with endovascular therapy from 15 January 2015 through 31 December 2015. Patients presenting with acute limb ischemia (n = 5) and patients undergoing peripheral intervention to the upper extremities (n = 6) or aorta (n = 11) were excluded from the analysis. Of the 82 patients in the final analysis, 45 had IC and 37 had CLI. Baseline characteristics were generally similar between the IC and CLI patients (Table 1), although current smoking rates were significantly higher among patients with IC and heart failure rates were significantly higher among patients with CLI. In addition, as compared to patients with IC, patients with CLI were older and had trends towards higher rates of hypertension, diabetes mellitus, atrial fibrillation, end stage renal disease, and prior PVI. Right leg ABI values <0.70 were 50.0% for IC and 41.1% for CLI. Non-compressible right leg values were 6.3% for IC and 41.2% for CLI. Left leg ABI values <0.70 were 46.9% for IC and 41.1% for CLI. Non-compressible left leg values were 3.1% for IC and 29.4% for CLI. Symptom burden of patients with IC by Rutherford class was 8.9% (n = 4) as class 2 (moderate claudication), 84.4% (n = 38) as class 3 (severe claudication), and 6.7% (n = 3) as class 4 (rest pain). Table 2 shows rates of recommended medical therapy use among patients with PAD. Rates were high for use of aspirin and statins; rates were modest for use of angiotensin-converting enzyme inhibitors or angiotensin receptor blockers. Approximately one-fifth of patients were receiving dual antiplatelet therapy before endovascular intervention. American Society of Anesthesiologists physical status classification scores (which were used to characterize the functional status of PAD patients undergoing endovascular therapy and to highlight comorbidity and systemic illness) were relatively high (≥2) before the index procedure for 16 patients (36.4%) with IC and for 32 patients (86.5%) with CLI (Table 2).
Baseline characteristics of patients.
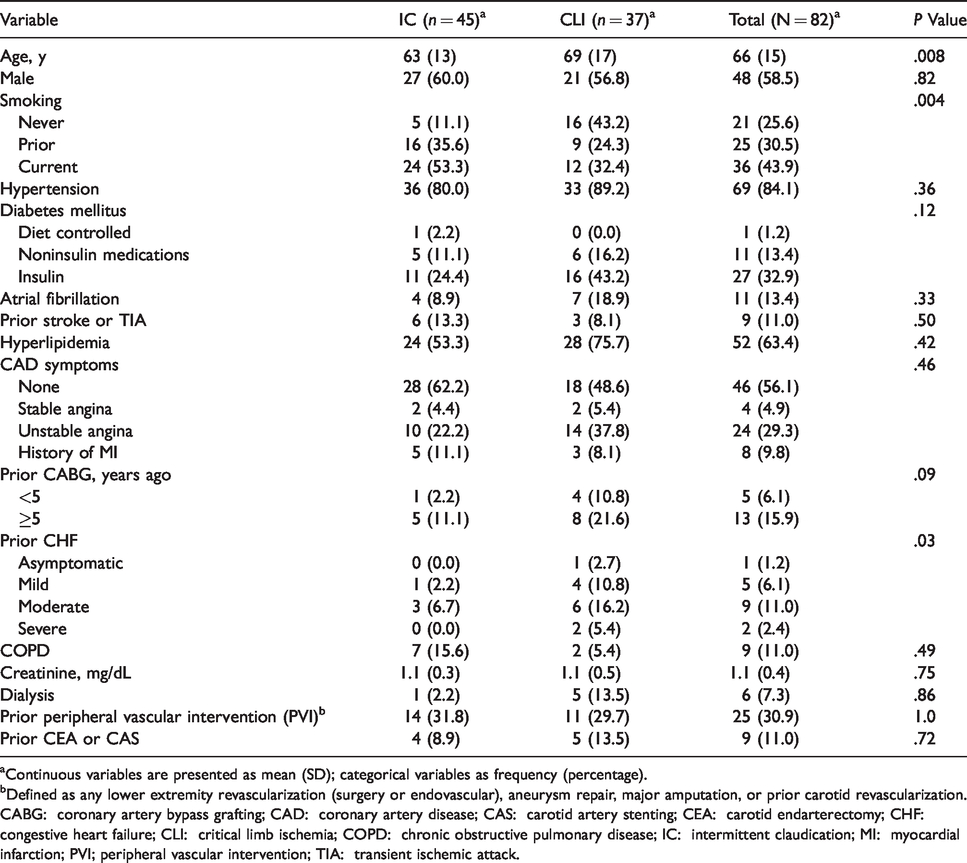
aContinuous variables are presented as mean (SD); categorical variables as frequency (percentage).
bDefined as any lower extremity revascularization (surgery or endovascular), aneurysm repair, major amputation, or prior carotid revascularization.
CABG: coronary artery bypass grafting; CAD: coronary artery disease; CAS: carotid artery stenting; CEA: carotid endarterectomy; CHF: congestive heart failure; CLI: critical limb ischemia; COPD: chronic obstructive pulmonary disease; IC: intermittent claudication; MI: myocardial infarction; PVI; peripheral vascular intervention; TIA: transient ischemic attack.
Patient preoperative status and medication use.

aValues are frequency (percentage).
ASA: American Society of Anesthesiologists; ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; CLI: critical limb ischemia; IC: intermittent claudication.
Procedural success was achieved in 91.3% of cases. Multi-specialty intervention (i.e. with subspecialist operators from ≥2 disciplines working together), compared with PAD intervention performed by a single operator, was commonly used during the period of the study and reflected the multidisciplinary operator component of our PAD program (Table 3). Rates of multispecialty procedures were high for IC patients (44.4%) and for CLI patients (62.2%). Anatomical level of disease and PAD lesion complexity are summarized in Table 3. The rates of TASC C or D lesions were high for iliac arteries (37.5%), femoropopliteal arteries (55.8%), and infrapopliteal arteries (81.8%). Table 4 summarizes observed rates of access site complications, discharge medications, and major CV events at 30 days. With respect to complication rates, actional bleeding rates at the access site were 2.4%, with one patient experiencing pseudoaneurysm requiring treatment. Rates of aspirin and statin at discharge were 91.5% and 87.8%, respectively. There were no observed deaths, myocardial infarctions, or strokes or transient ischemic attacks at 30 days. Repeat revascularization was performed more often for patients with CLI than for patients with IC (10.8% vs. 2.2%). Nearly a quarter of patients with CLI were hospitalized within 30 days of their index PAD procedure.
Procedural characteristics.
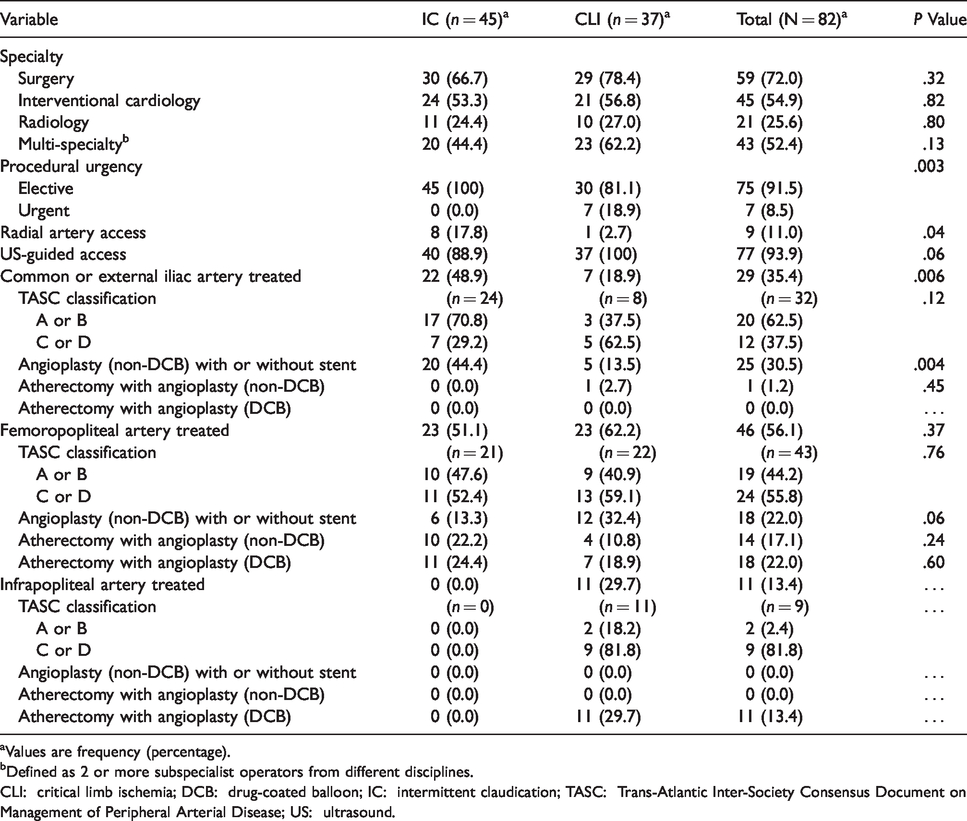
aValues are frequency (percentage).
bDefined as 2 or more subspecialist operators from different disciplines.
CLI: critical limb ischemia; DCB: drug-coated balloon; IC: intermittent claudication; TASC: Trans-Atlantic Inter-Society Consensus Document on Management of Peripheral Arterial Disease; US: ultrasound.
Postprocedural medications and outcomes.

aValues are frequency (percentage).
ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; AV: atrioventricular; CLI: critical limb ischemia; DOAC: direct oral anticoagulant; IC: intermittent claudication; MI: myocardial infarction; TIA: transient ischemic attack.
Median long-term follow-up was 2.2 years (IQR, 1.4–2.7 years). During follow-up, 17 patients died (15 in the CLI group and 2 in the IC group). For patients with IC, one-year survival was 97.4% and two-year survival was 94.4%; for patients with CLI, one-year survival was 76.8% and two-year survival was 57.5% (Figure 1). For patients with IC, freedom from hospitalization was 95.0% at one year and 83.5% at two years; for patients with CLI, freedom from hospitalization was 46.2% at one year and 32.7% at two years (Figure 2).

Overall survival. All patients underwent endovascular intervention for peripheral artery disease and had either intermittent claudication (IC) or critical limb ischemia (CLI).

Freedom from rehospitalization. All patients underwent endovascular intervention for peripheral artery disease and had either intermittent claudication (IC) or critical limb ischemia (CLI).
Discussion
The main findings of our study are the following: (1) community practices can implement multidisciplinary programs for patients who have PAD, (2) these patients can undergo endovascular treatment with low procedural morbidity and mortality, and (3) QI initiatives can be applied in a parallel fashion to inform practice and build collaboration with stakeholders. With the VQI registry covariates, QI initiatives can be implemented at community hospitals to inform process measures for improving the delivery of care to patients with PAD. Since many patients with PAD receive care at local hospitals and often establish long-term relationships, QI registries in community practice can be leveraged to detail long-term clinical outcomes.
Our study showed important comorbidity differences between IC and CLI patients. A larger percentage of IC patients were active smokers compared with CLI patients (53.3% vs. 32.4%). Patients who actively smoke are less likely to receive a durable treatment effect after endovascular intervention and are at higher risk of mortality. Although some observational studies have shown inconclusive relationships between smoking cessation and outcome by vascular subtype (coronary, cerebral, and peripheral), 6 Armstrong et al. 7 demonstrated that in the year after lower-extremity angiography, abstinence from smoking was associated with lower all-cause mortality and better amputation-free survival compared with continuation of smoking. The higher rates of heart failure, particularly among patients with a worse functional class, may also account for worse outcomes among patients with CLI. In our study, CLI patients had higher rates of moderate to severe heart failure than IC patients (21.6% vs. 6.7%). Coexisting heart failure has been shown to be independently associated with incident CLI 8 and may be an important risk factor for targeted intervention given the high rates of hospitalization in our study.
Our cohort of patients with PAD had high rates of antiplatelet and statin therapy to reduce CV risk; however, rates of renin-angiotensin inhibition were modest. The benefits of certain adjunctive pharmacotherapy, as recommended in practice guidelines, have been previously described from large clinical trials 9 , 10 and support the framework for continued emphasis on CV risk reduction in patients with PAD. 1 Large trials in this population will inform additional therapies to reduce CV risk and limb events. 11 QI programs are vital to help identify treatment gaps and introduce opportunities to strive for best clinical practice, which is critical to improve outcomes among high-risk patients. In our study, cross-disciplinary involvement (i.e. ≥2 operators from different specialties) during endovascular procedures was common (IC patients, 44.4%; CLI patients, 62.2%). Although multidisciplinary involvement in providing care to vascular patients is often recommended, few studies have demonstrated processes where collaborative endovascular care has been achieved.
Contrary to previous reports, 4 our study demonstrated that lower volume programs can deliver high-quality vascular care with low rates of procedural complications. Arora et al. 4 used administrative discharge data and billing codes to relate low-procedural-volume hospitals with adverse short-term outcomes for procedural complications, mortality, and amputation rates. However, that study was limited by an absence of follow-up, lack of data on novel endovascular devices such as drug-coated balloons and stents, and likely exclusion of patients who underwent endovascular treatment and did not require hospitalization after the intervention. The use of hospital volume as an indicator of quality has limitations, and some have advocated for more rigorous risk-adjusted outcome metrics and high-value QI initiatives to mirror high-volume practices. 12
The long-term follow-up of our study cohort demonstrated that despite low mortality among patients with IC, approximately 20% had a hospitalization event by two years. This finding highlights the comorbidity burden for patients with PAD, who remain at risk for subsequent events despite low mortality. Conversely, outcomes among patients with CLI are dismal over long-term follow-up, with high rates of hospitalization and a nearly 25% annual mortality rate. Vogel et al., 13 using Medicare claims data, showed similarly poor outcomes for CLI patients after tibioperoneal intervention: 30-day mortality, 6.7%; rehospitalization rate, 29.6%; and amputation rate, 23.8%. Patients with CLI are high users of health care resources and have a considerable baseline comorbidity burden. Future care delivery models for CLI patients may resemble those currently used for management of heart failure and include multidisciplinary teams, 14 incorporating not only wound management and limb salvage strategies but also management of guideline-recommended CV risk-reduction strategies and processes to decrease rehospitalization rates.
Our study was limited to a single community hospital practice with a modest sample size; however, baseline covariates were the same as those used in the VQI with the addition of long-term clinical follow-up. Owing to marked heterogeneity of patient triage, evaluation, and revascularization strategies pursued in the years prior to formation of our multidisciplinary vascular program, including limited data availability on important clinical variables, a pre-post comparison was not feasible. This limitation impacts identifying the magnitude of the benefit that multidisciplinary vascular practices can offer in the community hospital setting or elsewhere. Supervised exercise was preferred for eligible PAD patients in our study and was performed in our cardiac rehabilitation department; however, eligibility for insurance coverage varied and home exercises was recommended for those unable to complete a three-month (36 sessions) program. There are limited data for supervised exercise in CLI patients, as many have functional impairment, and further research into alternative exercise methods as part of CV risk-reduction in this population is needed. Finally, smoking abstinence was recommended prior to elective peripheral intervention in our study; however, we were unable to provide specific rates of true abstinence nor the success rates of smoking cessation in our population post intervention. Practice guidelines have recommended the use of societal registries for guidance on clinical outcomes and appropriateness of interventions. 1 Such processes could allow a deeper understanding of vascular services provided at regional programs and may help in development of strategies for ongoing improvement.
Conclusions
Good outcomes can be achieved in community PAD programs and can be aided by implementation of QI initiatives. The types of outcomes differ between patients with IC and patients with CLI, yet both groups require aggressive risk-reduction therapies. Since a majority of patients with PAD receive treatment locally, future research should engage community programs to document their process measures and perform regular QI audits of their practice to identify program strengths and opportunities for improvement. Further study is required to determine whether establishing multidisciplinary vascular QI initiatives will improve outcomes for patients with PAD.
Footnotes
Acknowledgements
Statistical support was provided through the Heart-Lung Focused Research Team at Mayo Clinic Florida.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.