
Abstract
Objective
Mycotic aneurysms of the infrapopliteal vessels are rare, with few cases reported in the literature. Management strategies are diverse and should be tailored to the patient’s presentation.
Methods
We describe the case of a 40-year-old male who presented with a painful left leg mass in the setting of bacteremia and infective endocarditis. Imaging revealed an aneurysm of the anterior tibial artery.
Results
The patient was treated with antibiotics and open surgical repair with excision of the aneurysmal sac, ligation of the anterior tibial artery, and primary repair of the popliteal artery and tibioperoneal trunk.
Conclusion
The epidemiology, pathophysiology, and clinical management of infrapopliteal aneurysms are briefly reviewed in this case study.
Introduction
Infrapopliteal aneurysms are extremely rare, the majority of which are found to be associated with trauma, infection, or an inflammatory process.1–5 In this case, we present a patient with an anterior tibial artery aneurysm that occurred in the setting of infective endocarditis and bacteremia.
Case description
A 40-year-old male presented for treatment of progressive shortness of breath, dyspnea at rest, orthopnea, and a painful left leg mass. The symptoms worsened over the duration of four weeks prior to presentation. He reported a history of a heart valve abnormality diagnosed 13 years prior on routine physical examination. He had no history of trauma, claudication, deep venous thrombosis, recent travel, intravenous drug use, open wounds of the lower extremity, congestive heart failure, or an immunocompromising disease. On examination, he was noted to have jugular venous distension, a grade 3/6 systolic murmur, and crackles in bilateral lower lung fields. Evaluation of the left lower extremity revealed a mass and tenderness to palpation along the posterior aspect of the leg, while the right lower extremity was found to be normal. The femoral and popliteal pulses were palpable bilaterally; however, the posterior tibial and dorsalis pedal pulses were slightly diminished on the left, compared to the right. Laboratory studies revealed leukocytosis. A chest radiograph was performed in the emergency department which revealed an enlarged cardiac silhouette with significant pulmonary edema. Subsequent transesophageal echocardiogram revealed severe mitral valve regurgitation and a tri-leaflet aortic valve with severe regurgitation and vegetations. A duplex ultrasound (US) was performed on the left lower extremity and demonstrated a left lower extremity mass. Computed tomography angiogram (CTA) of the left lower extremity revealed a 10.8 × 3.9 × 1.8 cm ovoid mass concerning for an aneurysm arising from the proximal left anterior tibial artery (Figure 1). A conventional angiogram confirmed the aneurysm of the proximal anterior tibial artery (Figure 2). There was runoff to the foot via the posterior tibial and peroneal arteries, and there was delayed filling of a small caliber anterior tibial artery, with slower opacification of contrast than the posterior tibial and peroneal arteries. The dorsalis pedis artery reconstituted via collaterals from the peroneal artery before direct flow from the anterior tibial artery.

Sagittal reconstruction of CTA demonstrates an anterior tibial artery aneurysm.
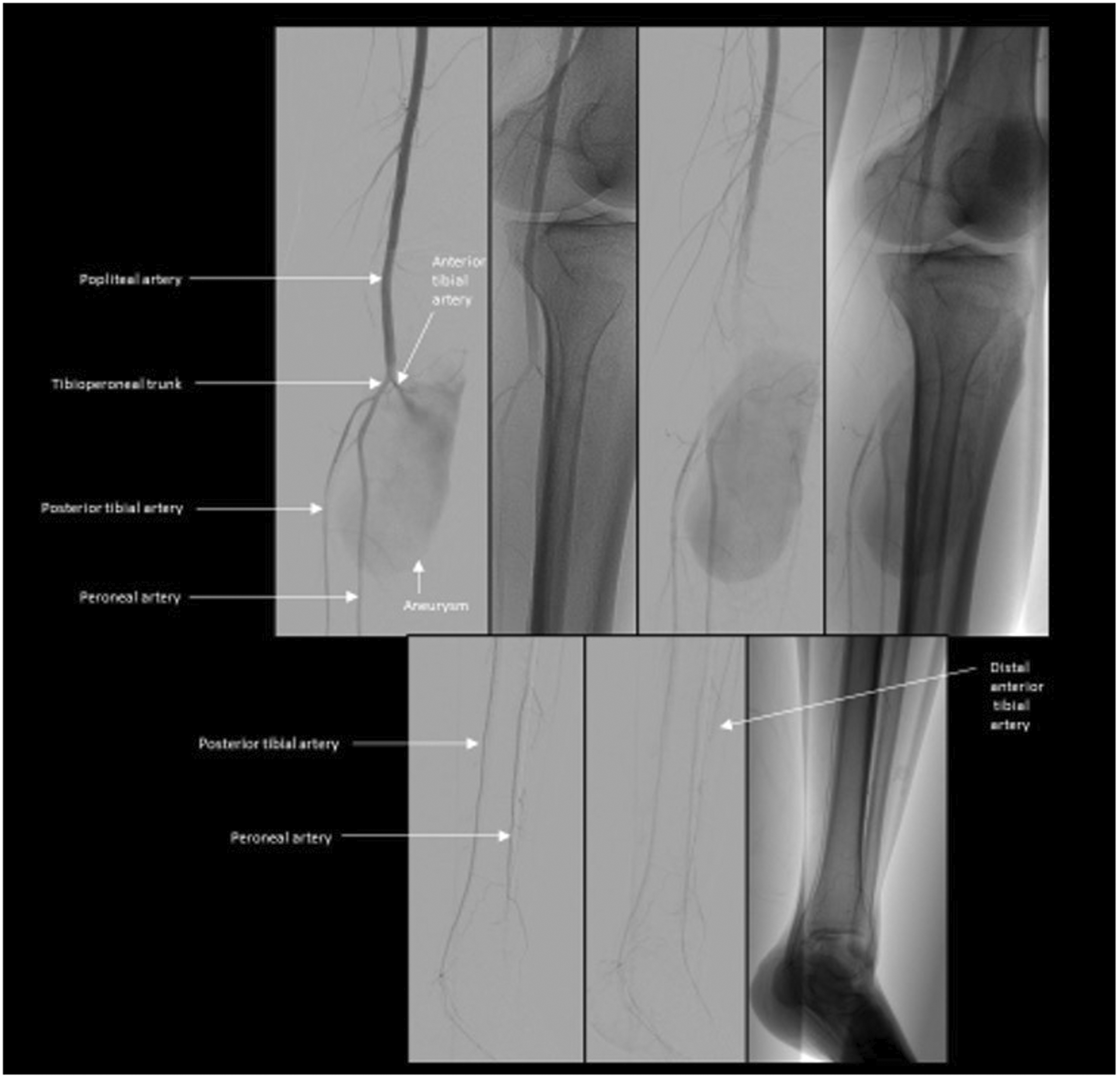
Conventional angiogram aneurysm of the proximal anterior tibial artery and distal runoff.
The patient was admitted to the cardiac intensive care unit for suspected infective endocarditis. He underwent a bioprosthetic aortic and mitral valve replacement. The following day, the patient underwent repair of the left anterior tibial artery aneurysm. A longitudinal incision was made along the medial aspect of the left leg. The infrageniculate popliteal artery was controlled proximally. The posterior tibial and peroneal arteries were controlled distally. Using a lateral incision in the mid leg, the anterior tibial artery was controlled distally. Next, from the medial incision, the anterior tibial vein was ligated and divided and the tibioperoneal trunk was controlled. The origin of the anterior tibial artery was controlled. After heparinizing the patient, the popliteal artery, tibioperoneal trunk, and distal anterior tibial artery were each clamped. The origin of the anterior tibial artery was transected off the popliteal artery. The anterior tibial artery aneurysm was dissected out (Figure 3(a)) and a portion of the aneurysm sac was removed for histological evaluation. The anterior tibial artery became aneurysmal within a centimeter of its origin. The anterior tibial artery was transected off the popliteal artery at its origin. The popliteal artery and tibioperoneal trunk were primarily repaired using a transverse closure of interrupted 7–0 prolene sutures (Figure 3(b)). The anterior tibial artery was transected off the popliteal artery at its origin. The popliteal artery and tibioperoneal trunk were primarily repaired using a transverse closure of interrupted 7–0 prolene sutures (Figure 3(b)). The anterior tibial artery was definitively ligated through the lateral incision. The dorsalis pedis and posterior tibial pulses were palpable and unchanged from the baseline pulse examination after ligation of the anterior tibial artery. Since the preoperative angiogram demonstrated opacification of the dorsalis pedis artery via peroneal collaterals, pulses were unchanged, and he had no symptoms of ischemia, we did not feel that reconstruction of the anterior tibial artery was necessary. The patient had an uneventful post-operative course and was discharged home on low-dose acetylsalicylic acid and an extended course of antibiotics. The patient’s peripheral blood cultures grew Cardiobacterium hominis (C. hominis). However, the pathology of the aortic valve leaflet and the anterior tibial artery aneurysm did not show any microbial growth. Follow-up arterial duplex imaging demonstrated patency of the popliteal artery and tibioperoneal trunk, without recurrence of the aneurysm. The posterior tibial and peroneal arteries were patent, and the distal anterior tibial artery reconstituted via collaterals.
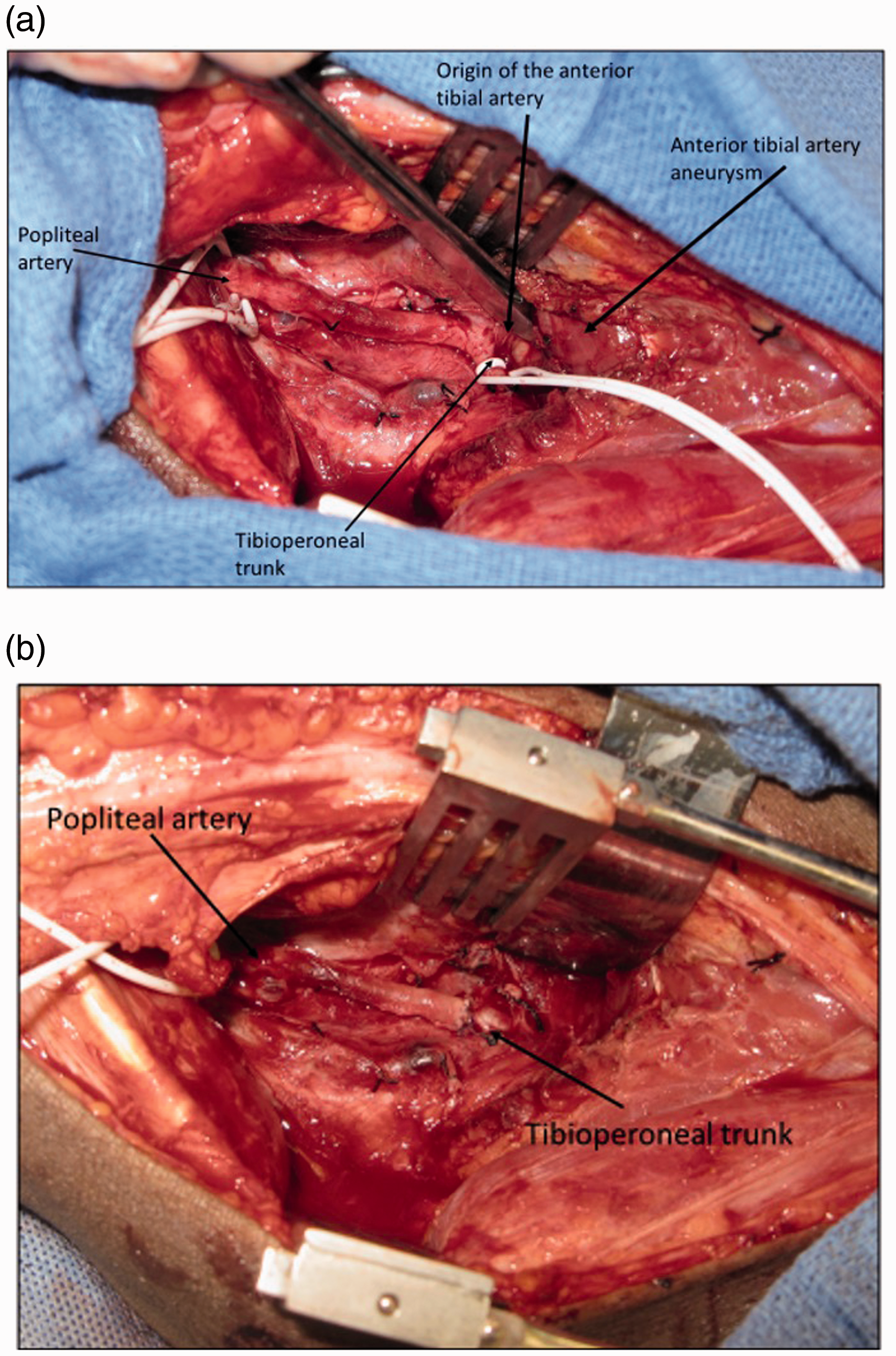
(a) Intraoperative exposure of anterior tibial artery aneurysm. (b) Intraoperative image after transection of origin of anterior tibial artery and transverse repair with interrupted sutures.
Discussion
Anterior tibial artery aneurysms associated with an infectious etiology are rare. 5 Patients more commonly present with pseudoaneurysms to the infrapopliteal vessels resulting from injury to the lower extremity. Known risk factors for aneurysmal degeneration are smoking, male sex, collagen disorders, infection, and trauma. 3
Patients with infrapopliteal aneurysms may present with symptoms of calf pain, paresthesia, pulsatile mass, ischemia, or hemorrhage. These symptoms raise concern for expanding size, thromboembolism, or rupture of the aneurysm. Patients may also present without symptoms. Work-up of infrapopliteal aneurysms should include a thorough history, physical examination, blood cultures, and consideration of echocardiography. Imaging of the peripheral vasculature can be done with duplex US, CTA, and/or Magnetic resonance imaging.
Aneurysms due to infectious etiology, or mycotic aneurysms, have an incidence of 1%–3.7% with Staphylococcus aureus being the most commonly involved organism. 5 Blood cultures of the patient presented in this case study grew C. hominis, a gram negative bacillus, which is a rare cause of infective endocarditis. C. hominis has low virulence and a frequently indolent course, with vague symptoms preceding diagnosis for up to 169 days on average. 6 Mycotic aneurysms due to C. hominis have been reported in the cerebral vasculature and the mesenteric arteries. Malani et al. reported that there are only 61 cases of C. hominis infective endocarditis in the literature and, of these cases, 9% are found to have a complication of a mycotic aneurysm. 7 The patient we present in this case study developed an aneurysm of the anterior tibial artery in the setting of infective endocarditis and bacteremia. It is possible that this aneurysm was related to the infective endocarditis, but the cultures of the aneurysm wall had no microbial growth. Preoperative antibiotic therapy may have sterilized any infection. It is also possible for the aneurysm to be unrelated to the infection, but less likely.
Once the diagnosis of a tibial artery aneurysm is made, management should be tailored to the patient’s symptoms and physical examination findings. In the setting of the asymptomatic, small aneurysm, close follow-up and imaging to monitor for growth or symptom development have been reported. 3 Leoce et al. proposed that if an infrapopliteal arterial aneurysm is larger than three times the normal limit, intervention is recommended. 3 Prospective data about the risk of rupture, and threshold for intervention is not available, presumably due to the rarity of this diagnosis. If the patient is symptomatic, either due to mass effect or limb ischemia, an intervention is recommended. If infection is suspected, intervention is indicated for the prevention of aneurysm rupture.
There are several approaches to treating infrapopliteal arterial aneurysms. Endovascular therapy can include embolization (using coils, vascular plugs, or injection of occlusive agents) or stent graft placement. However, in the setting of infection, surgical therapy is preferred, as a mycotic aneurysm can be excised for source control of the infection. Surgical therapy includes ligation and resection of the mycotic aneurysm, with or without revascularization. If adequate collateral circulation is present or if there is significant degeneration of the arterial wall such that it would jeopardize the graft, surgical ligation without bypass is possible. In a setting where bypass is required, an autologous reversed saphenous vein graft is the preferred conduit. In the case presented, an aneurysmal resection with primary transverse repair of the defect in the popliteal artery and tibioperoneal trunk was performed. In our patient, there were palpable pulses in the foot despite anterior tibial artery ligation, due to robust collateral circulation. Arterial bypass was not required. Furthermore, the added operative time required for performing an arterial bypass would have placed the patient at risk for increased perioperative complications.
Conclusion
Anterior tibial artery aneurysms are extremely rare. In a patient with a diagnosis of endocarditis or bacteremia with a symptomatic unilateral leg mass, a mycotic aneurysm should remain high on the differential diagnosis. We advocate for either percutaneous or operative intervention with management strategies tailored to the patient’s specific needs. The combined medial and lateral approach provides complete vascular control in an aneurysm of the proximal anterior tibial artery. In symptomatic patients, patients meeting size criteria, and those with suspicion of mycotic aneurysm, we recommend surgical repair of the aneurysm given the risk of rupture or thromboembolism to mitigate the complication of limb loss in the future.
Footnotes
Authors’ note
All authors attest that they meet the current ICMJE criteria for Authorship.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Consent to publish the case report was obtained.