
Abstract
Objectives
The aim of this study was to determine the relationship between preoperative nutritional status and wound healing in patients undergoing surgical reconstruction for ischemic tissue loss.
Methods
The preoperative nutritional status of patients who underwent surgical reconstruction for ischemic tissue loss for the years 2011–2018 was retrospectively estimated using the Controlling Nutritional Status (CONUT) score. Patients were allocated to two groups: Group I, normal nutrition or mild malnutrition (CONUT score ≤4), and Group II, moderate-to-severe malnutrition (CONUT score ≥5). Wound healing was set as the primary endpoint and major amputation and death as the secondary endpoints. The wound healing, limb salvage, and overall survival rates were calculated after two years using the Kaplan–Meier method, and Cox proportional hazards regression analysis was performed to determine which variables were independently associated with these outcomes.
Results
Forty-eight patients with missing values for the CONUT score were excluded. A total of 174 limbs in 147 patients were studied (Group I: 115 limbs in 100 patients; Group II: 59 limbs in 47 patients). The mean duration of the study was 519 ± 270 days. The Kaplan–Meier curves showed that wound healing in Group I was superior to that in Group II (Group I vs. II: two-year wound healing, 97% vs. 79%; time to 50% wound healing, 83 vs. 150 days, p < 0.001), and multivariate analysis showed that the CONUT score was an independent predictor of wound healing (hazard ratio, 0.63; 95% confidence interval, 0.41–0.98; p = 0.038).
Conclusions
Patients with better preoperative nutritional status are more likely to experience wound healing earlier than those with excessive malnutrition.
Keywords
Introduction
Nutritional status is an important predictor in the prognosis of patients with various medical conditions, including patients with peripheral artery disease (PAD). Several previous studies have shown that objective nutritional indices, calculated using multiple simple parameters, are associated with the prognosis of patients with PAD.1–7 However, in the studies conducted to date, death, major amputation, or cardiovascular events were set as the endpoints, and none have described the relationship between nutritional index and wound healing (WH), which is one of the most important goals of treatment for ischemic tissue loss.
The Controlling Nutritional Status (CONUT) score is a widely used nutrition index that is calculated using two simple biochemical parameters and one immune system indicator. The serum albumin (Alb) and total cholesterol (T.Chol) concentrations reflect protein reserves and caloric depletion, respectively, and both may be closely related to tissue repair. The total lymphocyte count (TLC) is an indicator of immune status, which may be impaired by undernutrition, resulting in poor healing of wounds complicated by infection. Therefore, the CONUT score may be able to predict WH.
The aim of the present study was to determine the relationship between preoperative nutritional status, assessed using the CONUT score, and WH in patients who underwent surgical reconstruction following ischemic tissue loss.
Patients and methods
The institutional review board of Kokura Memorial Hospital, Kitakyushu City, Japan, approved the study design (No. 20052901; 29 May 2020).
Database and patient selection
The records of patients who underwent open surgery because of tissue loss from PAD at Kokura Memorial Hospital from January 2011 through December 2018 were reviewed. Patients with a history of surgical reconstruction in the ipsilateral leg but not of endovascular therapy (EVT) were excluded.
Variables used in the analyses
The following variables were retrieved from the electronic medical record: age; sex; date of surgery; preoperative laboratory data for Alb, T.Chol, TLC, serum C-reactive protein (CRP) concentration; left ventricular ejection fraction (LVEF); ambulatory status; history of diabetes mellitus (DM), coronary artery disease (CAD), cerebrovascular disease (CVD), or end-stage renal disease (ESRD); current smoking status; Rutherford classification; body mass index (BMI); surgical method; the affected angiosome; postoperative medication (a statin or cilostazol); and details of the patent graft.
Evaluation of nutritional status
Preoperative nutritional status was assessed using the CONUT score. The CONUT score is the sum of the score given to each of the three constituent parameters: Alb (score) ≥3.5 g/dL (0), 3.0–3.4 g/dL (2), 2.5–2.9 hx00A0;g/dL (4), <2.5 g/dL (6); T.Chol (score) ≥180 mg/dL (0), 140–179 mg/dL (1), 100–139 mg/dL (2), <100 mg/dL (3); and TLC (score) ≥1600/µL (0), 1200–1599/µL (1), 800–1199/µL (2), and <800/µL (3). 8
Grouping of participants
Stratification of the CONUT score was performed in accordance with the original report of Ulibarri et al.: 8 normal (0–1), mild (2–4), moderate (5–8), and severe (9–12) malnutrition. The participants were allocated to two groups on the basis of their CONUT score: Group I, normal or mild malnutrition, and Group II, moderate-to-severe malnutrition. Patients with missing values for any of the nutritional indices were excluded from the analysis.
Outcome measures
The primary endpoint was WH in the indicated limb, and the secondary endpoints were major amputation, all-cause mortality, and patency of the revascularized artery within 30 days of surgery. WH and limb salvage (LS) were assessed for each limb, and overall survival (OS) was assessed for all the participants. When patients underwent bilateral surgical reconstructions on different dates, the records of the initial surgery alone were used for the analysis of OS.
Follow-up of the patients
During hospitalization, the wound and patency of the revascularized artery were checked once a day. After discharge, the patients were monitored as outpatients by measurement of ankle–brachial pressure index and duplex ultrasonography at intervals of one to three months. The conditions of the wound and limb, and survival, were verified by phone interview of the patients or their local physician when the patient was unable to visit the hospital. A final review was conducted between September and December 2019, and then up to two years’ worth of data was analyzed.
Definitions
Ambulation was defined as the ability to walk to the lavatory without any assistance. DM was defined as a fasting blood glucose ≥105 mg/dL or ongoing therapy with oral hypoglycemic agents or insulin. CAD was defined as a history of angina pectoris, myocardial infarction, percutaneous coronary intervention, or coronary artery bypass grafting. CVD was defined as a history of transient ischemic attack, cerebral infarction, cerebral bleeding, or revascularization of a carotid artery or intracranial artery. Patients with a smoking habit who had continued smoking up to just before surgery were defined as current smokers. Infrapopliteal revascularization was defined as a bypass or patch angioplasty of the crural or foot artery. The angiosome was defined in accordance with the definitions of Attinger et al. 9 Cases without complete revascularization of the foot were defined using the indirect angiosome. Patent graft was defined as the secondary graft patency that was maintained until WH. Major amputation was defined as the loss of the leg above the ankle. WH was defined as complete epithelialization of the ischemic ulcer of the foot or stump of the amputated toe or forefoot.
Statistical analyses
Data are presented as the median ± standard deviation for continuous variables and the number (percentage) for categorical variables. In the survival curve, values are expressed as the survival rate ± standard error. Continuous and categorical data were compared between the groups using the unpaired t-test and Fisher’s exact test, respectively. Survival curves were calculated using the Kaplan–Meier method, and comparisons between the two groups were evaluated using the log-rank test. Multivariate analysis was performed using Cox proportional hazards regression analysis. Initially, a univariate analysis using all the variables listed in Table 1 was performed, and multivariate analysis was then performed using the variables with p < 0.1 in the univariate analysis, plus age and sex as the independent variables. WH, major amputation, or death was used as the dependent variable. p < 0.05 was considered to indicate the statistical significance. Statistical analyses were performed using JMP, version 14.2, for the Mac (SAS Institute, Cary, NC, USA).
Characteristics of 174 limbs in 147 patients.
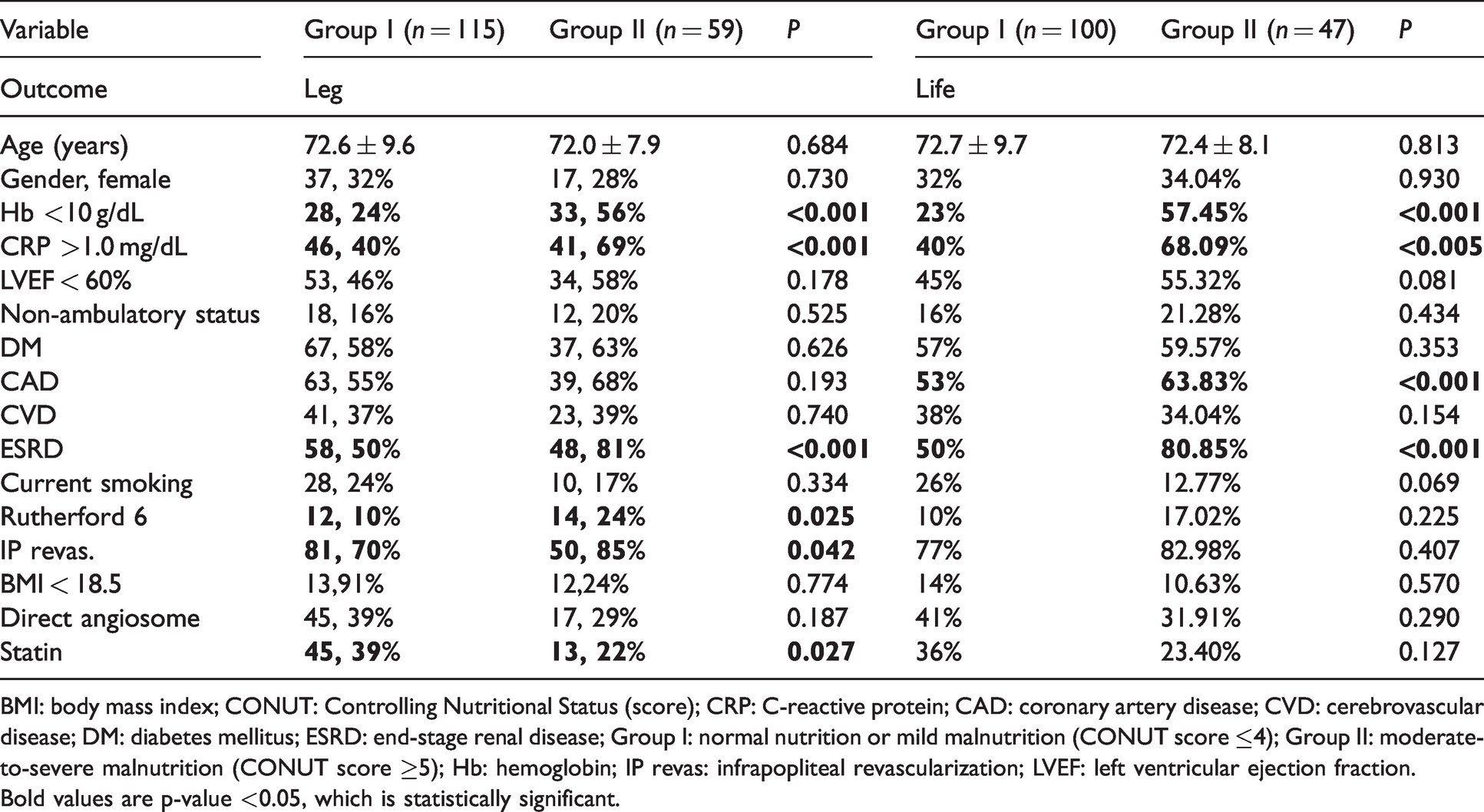
BMI: body mass index; CONUT: Controlling Nutritional Status (score); CRP: C-reactive protein; CAD: coronary artery disease; CVD: cerebrovascular disease; DM: diabetes mellitus; ESRD: end-stage renal disease; Group I: normal nutrition or mild malnutrition (CONUT score ≤4); Group II: moderate-to-severe malnutrition (CONUT score ≥5); Hb: hemoglobin; IP revas: infrapopliteal revascularization; LVEF: left ventricular ejection fraction.Bold values are p-value <0.05, which is statistically significant.
Cox proportional hazard regression analyses of WH, LS, and OS rates.
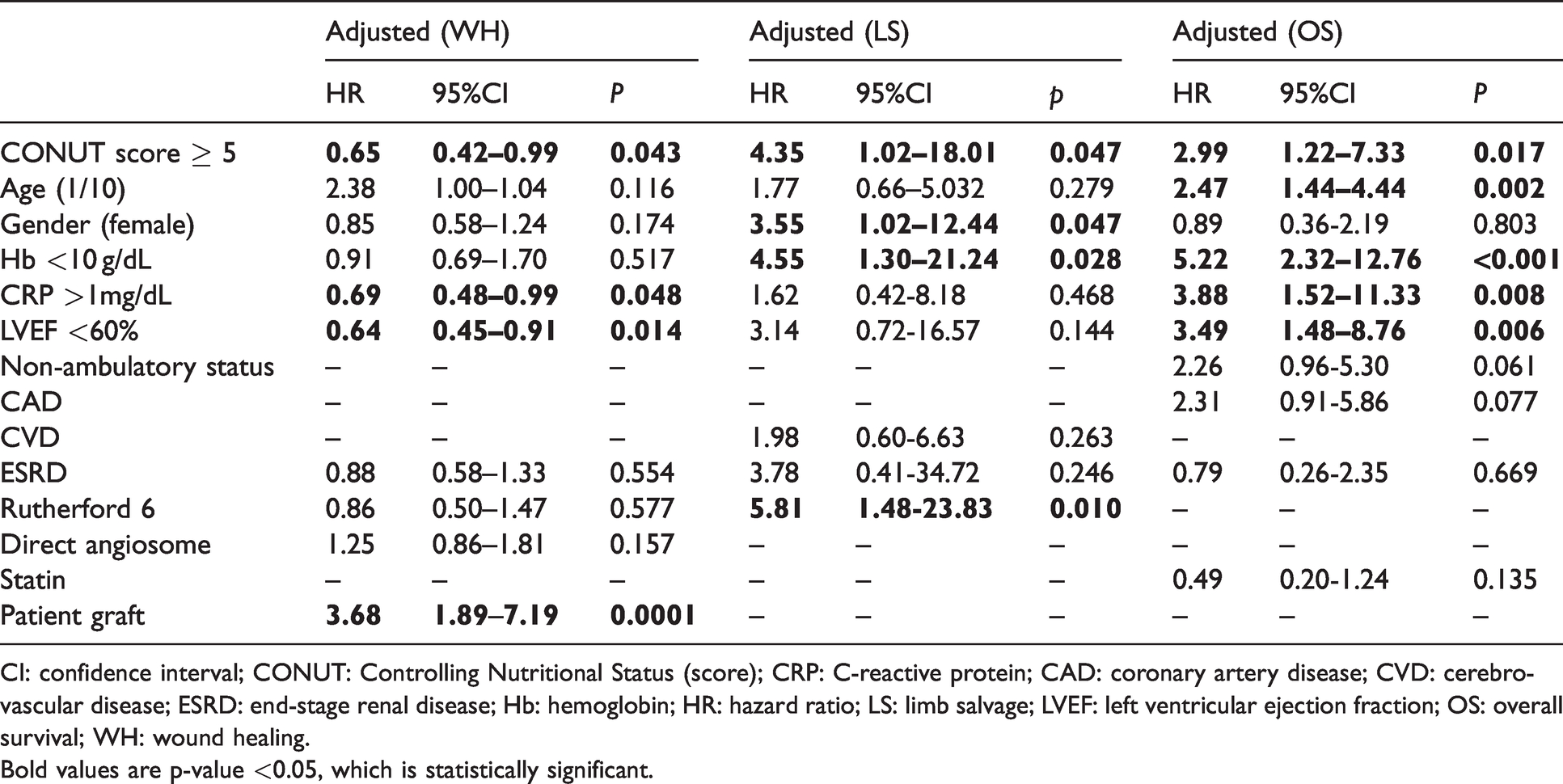
CI: confidence interval; CONUT: Controlling Nutritional Status (score); CRP: C-reactive protein; CAD: coronary artery disease; CVD: cerebrovascular disease; ESRD: end-stage renal disease; Hb: hemoglobin; HR: hazard ratio; LS: limb salvage; LVEF: left ventricular ejection fraction; OS: overall survival; WH: wound healing.Bold values are p-value <0.05, which is statistically significant.
Results
Inclusion of patients in the analysis
A total of 222 patients who underwent surgical reconstruction for tissue loss because of PAD were consecutively recruited. However, 48 patients were excluded because of missing data; therefore, WH and LS were evaluated in 174 participants. Groups I and II comprised 115 (normal nutrition, 29; mild malnutrition, 86) participants and 59 (moderate malnutrition, 52; severe malnutrition, 7) participants, respectively. Because 27 of the 174 participants underwent bilateral open surgery, OS was analyzed in 147 participants. Of these, Groups I and II comprised 100 (normal nutrition, 27; mild malnutrition, 73) participants and 47 (moderate malnutrition, 42; severe malnutrition, 5) participants, respectively (Figure 1).
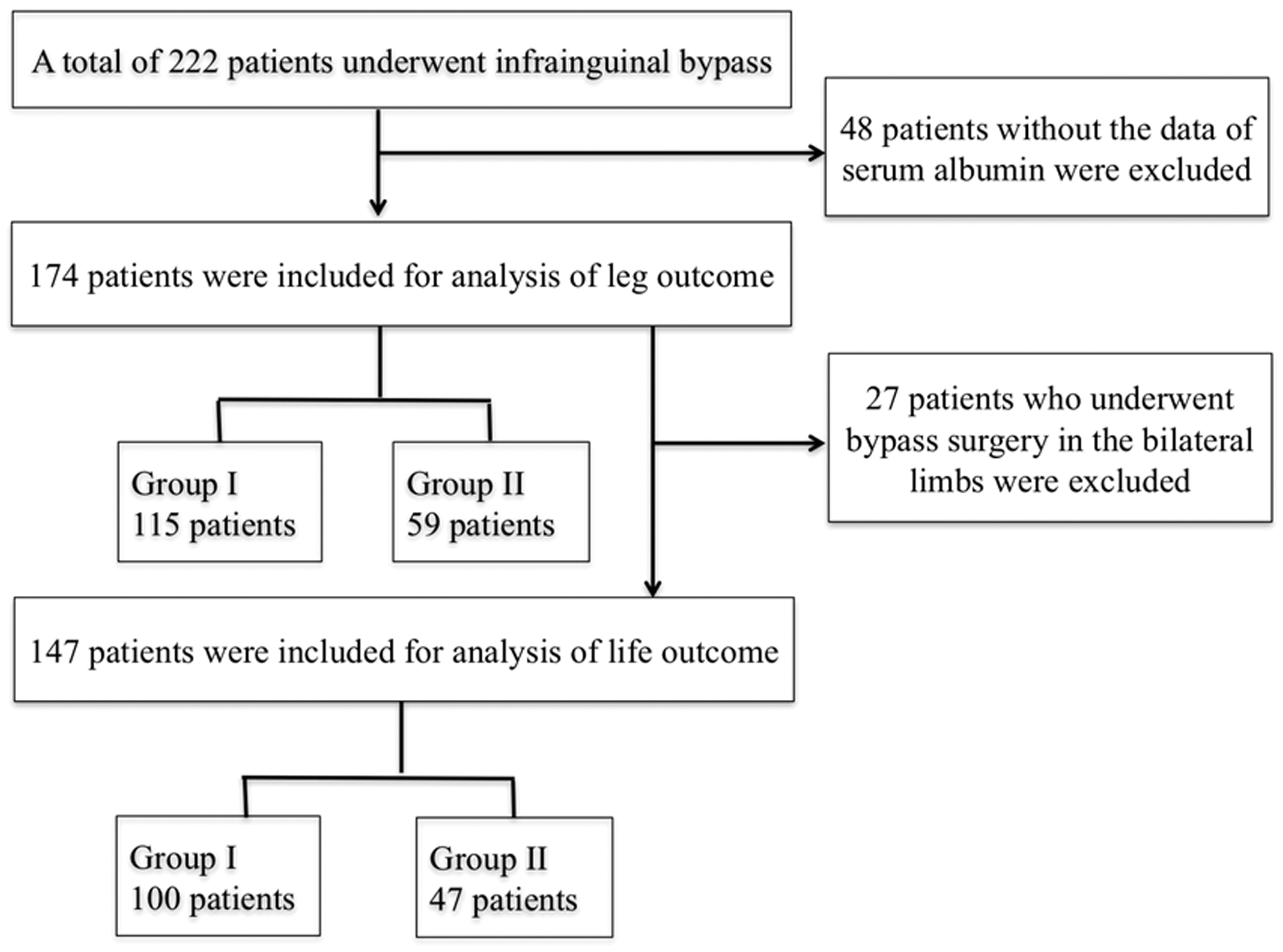
Patient participation flowchart.

Wound healing (a), limb salvage (b), and overall survival (c) rates.
Baseline characteristics
In the 174 limbs in which WH and LS were analyzed, Group II showed significantly higher percentages of hemoglobin (Hb) <10 g/dL, CRP >1 mg/dL, ESRD, Rutherford classification 6, infrapopliteal revascularization, and statin use than Group I. In the 147 participants in which OS was analyzed, Group II showed a significantly higher percentage of Hb <10 g/dL, CRP >1 mg/dL, and ESRD than Group I (Table 1). Surgical reconstruction consisted of suprainguinal bypass in three limbs, endarterectomy of the common femoral artery in eight limbs, patch angioplasty of the crural artery in one limb, popliteal artery bypass in 33 limbs, tibialis anterior artery and dorsalis pedis artery bypass in 64 limbs, tibialis posterior artery and plantaris artery bypass in 49 limbs, and peroneal artery bypass in 5 limbs.
Adverse events within 30 days of surgery
Seven patients with seven affected limbs (four in Group I and three in Group II) died within 30 days of surgery. Four limbs (three in Group I and one in Group II) required major amputation within 30 days of surgery (the participants were alive for over 30 days). One graft lost patency within 30 days of surgery (the patient was alive and had not required major amputation during this period).
Survival curves for late outcomes
Twelve limbs that had the adverse events described above were excluded from the analysis of WH and LS, as were five participants (four in Group I and one in Group II) who died within the first 30 days following surgery (two participants who had undergone bilateral surgery had already been omitted) were excluded from the analysis of OS. Consequently, 162 limbs and 142 participants were included in the analysis of WH and LS, and OS, respectively.
Wound healing
The prevalences of WH after 3, 6, 12, and 24 months in Groups I and II were 56 ± 5% and 31 ± 6%, 79 ± 4% and 55 ± 7%, 89 ± 3% and 70 ± 7%, and 97 ± 2% and 79 ± 6%, respectively. The time taken to achieve a 50% prevalence of WH in Groups I and II were 83 and 150 days, respectively (p < 0.001) (Figure 2a).
Limb salvage
The prevalences of LS after 3, 6, 12, and 24 months in Groups I and II were 99 ± 1% and 90 ± 4%, 98 ± 1% and 86 ± 5%, 97 ± 2% and 81 ± 6%, and 96 ± 2% and 81 ± 6%, respectively (p < 0.001) (Figure 2b).
Overall survival
The overall prevalences of survival after 3, 6, 12, and 24 months in Groups I and II were 100% and 89 ± 5%, 97 ± 2% and 76 ± 6%, 93 ± 3% and 66 ± 7%, and 87 ± 4% and 52 ± 8%, respectively (p < 0.01) (Figure 2c).
Cox proportional hazard regression analysis
For WH, CONUT score ≥5 (hazard ratio (HR), 0.65; 95% confidence interval (CI), 0.42–0.99; p = 0.043), CRP >1 mg/dL (HR, 0.69; 95% CI, 0.48–0.99; p = 0.048), LVEF < 60% (HR, 0.64; 95% CI, 0.45–0.91; p = 0.014), and a patent graft (HR, 3.68; 95% CI, 1.89–7.19; p = 0.0001) were significant predictors. For LS, CONUT score ≥5 (HR, 4.35; 95% CI, 1.02–18.01; p = 0.045), female sex (HR, 3.55; 95% CI, 1.02–12.44; p = 0.047), Hb <10 mg/dL (HR, 4.55; 95% CI, 1.30–21.24; p = 0.028), and Rutherford classification 6 (HR, 5.81; 95% CI, 1.48–23.83; p = 0.010) were shown to be significant predictors. For OS, CONUT score ≥5 (HR, 2.99; 95% CI, 1.22–7.33; p = 0.017), age (HR, 2.47 per 10-year increase; 95% CI, 1.44–4.44; p = 0.002), Hb <10 mg/dL (HR, 5.22; 95% CI, 2.32–12.76; p < 0.001), CRP >1 mg/dL (HR, 3.88; 95% CI, 1.52–11.33; p = 0.008), and LVEF <60% (HR, 3.39; 95% CI, 1.48–8.76; p = 0.006) were significant predictors (Table 2).
Discussion
We showed that prior to surgical reconstruction, patients with normal nutritional status or mild malnutrition according to the CONUT score had a much better prognosis with respect to WH than those with moderate-to-severe malnutrition. Multivariate analysis demonstrated that good nutritional status is an independent predictor of WH. Furthermore, the same results were obtained with respect to LS and OS.
There have been many studies regarding the association between nutrition and WH in patients with critical limb ischemia (CLI). Most of these studies used Alb as an indicator of nutritional status,10–13 but Alb can be affected by infection or other disease states. Therefore, the assessment of nutritional status using Alb alone may not provide an accurate prognosis, especially in patients with ischemic tissue loss.
Several groups have described the use of nutritional indices calculated using multiple parameters to predict both early and longer-term outcomes in patients with PAD.1–7 However, to the best of our knowledge, there have been no studies of the relationship between preoperative nutritional status assessed using a nutritional index and WH. Therefore, we believe that this is the first study to show a positive relationship between these parameters in patients with tissue loss.
Many factors influence the process of WH. Azuma et al. 14 defined five categories that influence WH: (1) systemic factors; (2) the clinical status of the tissue defect; (3) infection; (4) the wound management strategy; and (5) the revascularization strategy. Adequate blood supply to the area of ischemic tissue loss is one of the most important factors required to permit complete WH and to shorten the time taken. In the present study, according to the multivariate analysis, a patent graft is the most important factor.
This study also showed that the preoperative nutritional status is a systemic factor that reflects the overall systemic disease status, which in turn affects WH. However, the nutritional status of patients can be modified after surgery by the efforts of the patients themselves. In a real-world clinical setting, we often experience poor or delayed WH in patients with poor nutritional status. However, those who increase their food intake improve their protein reserves and immune function and prevent calorie depletion. They achieve a lower CONUT score and their WH accelerates. Therefore, nutritional status after revascularization, in addition to the preoperative status, may have an important effect on WH. Although we did not investigate the connection, patients with superior preoperative nutritional status may also have superior postoperative nutritional status and better WH.
In addition to the CONUT score, CRP, LVEF, and a patent graft are independent predictors of WH. Infection, which is usually accompanied by an increase in serum CRP concentration, is one of the factors that affect WH, 14 and it is common for improved cardiac function to promote WH. Moreover, there is no doubt that maintenance of blood flow is necessary for WH after revascularization.
Therefore, in this study, patent graft was a positive factor, and malnutrition, infection, and low cardiac function were negative factors for WH. We have also shown that preoperative nutrition is an independent predictor of LS and OS. Two previous studies conducted in Japan demonstrated a relationship between nutritional indices and major amputation. Shiraki et al. 12 showed that in patients who were followed up for three years after EVT, the Geriatric Nutritional Risk Index (GNRI), which is another widely used nutritional index, is an independent predictor of the avoidance of major amputation in patients with CLI. 2 Conversely, Mii et al. 3 found that neither the GNRI nor the CONUT score was independently associated with five-year LS in patients undergoing infrainguinal bypass for CLI. In the present study, we have shown that LS is positively related to preoperative nutritional status, which is consistent with the finding that it is a significant predictor of WH. However, to maintain LS over a longer period, patency of the revascularized artery is important to prevent the recurrence of tissue loss. The duration of the study and the sample size were insufficient to assess the recurrence of tissue loss in the present study. Therefore, it would be premature to draw conclusions regarding the effect of preoperative nutritional status on LS on the basis of the available data.
It is clear that preoperative nutritional status has an important influence on the mortality of patients with PAD. A number of studies, including the present one, have demonstrated close relationships between nutritional indices and survival and mortality-related outcomes. Shiraki et al. 2 showed that GNRI is independently associated with all-cause mortality in patients with CLI undergoing EVT, and Mizobuchi et al. 5 showed that a CONUT score ≥ 5 is an independent predictor of three-year OS in patients with PAD undergoing EVT. Mii et al. 3 also demonstrated that both the GNRI and CONUT scores have close relationships with early and long-term survival and mortality-related outcomes in patients with CLI undergoing open bypass. In addition, Matsuo et al. 6 demonstrated a significant relationship between GNRI at admission and five-year OS, and Mont et al. 7 showed that malnutrition, demonstrated using the GNRI and Mini Nutritional Assessment, is associated with poorer early outcomes in patients hospitalized for CLI. Although the present study was shorter than the previously reported studies, 2 , 3 , 5 , 6 similar results were obtained. Taking these findings together, there is mounting evidence that preoperative nutritional status is an independent predictor of long-term mortality in patients with CLI.
The present study had several limitations. First, it was a retrospective study performed at a single center. Second, the sample size was small. Third, 48 sets of data were excluded because of incomplete data. Fourth, patient compliance with medication was not assessed; therefore, changes in medication may have been made during the follow-up period. Fifth, the exact date of complete WH could not be objectively confirmed. After the patients had been discharged with an unhealed ulcer, healing was reported by the patient while being cared for in an outpatient setting or by phone with their local physician. Sixth, it took an average of 10.5 days (1–38 days) from blood collection (nutritional evaluation) to surgical revascularization, and the time lag was long in some cases. Finally, the Society for Vascular Surgery Wound, Ischemia, and foot infection (WIfI) classification system, which is useful for prognostic analyses,16,17 could not be used in the present study because there were significant numbers of missing data points.
Conclusions
Compared with those having poorer preoperative nutritional status, patients with good preoperative nutritional status, according to the CONUT score, are more likely to achieve WH and to achieve WH earlier. Patients with good preoperative nutritional status are also likely to survive and not undergo amputation for a longer period of time after surgical bypass for ischemic tissue loss.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.