
Abstract
Background/Objective
Temporary intravascular shunts are widely used in military surgery, representing a bridging until definitive vascular reconstruction. In civilian practice, shunts are mainly used as damage control and as a temporary measure until orthopaedic fixation. The objective of this report is to illustrate a new approach to the temporary restoration of perfusion during open management of extremity arterial injury.
Methods
The authors present a technique that uses sheaths introducers, instead of commercial or purpose-built shunts, which can be used through surgical or percutaneous approaches. Three clinical cases are presented where this technique was performed.
Keywords
Introduction
Vascular limb trauma is rare among civilians with a frequency between 1% and 4%. 1 Temporary intravascular shunts (TIVS) are widely used in military surgery, representing a bridging until definitive vascular reconstruction. 2 , 3 Possible indications for TIVS are damage control in an unstable patient, Type IIIC Gustilo fractures, complex vascular reconstructions or during vein harvesting, prioritizing thoracic/abdominal trauma before limb trauma, need for transferring a traumatized patient to a specialized vascular trauma centre for definitive surgical care, catastrophic scenario, or before limb reimplantation. 1 , 4 Several types of shunts are available (Javid®, Argyle®, Pruitt-Inihara®). However, chest or nasogastric tubes and intravenous flow lines have been successfully used, with no differences in terms of shunt patency when compared to commercial shunts. 5 , 6
Usually, proximal and distal surgical control of the damaged artery is performed and a TIVS with a similar corresponding artery diameter is placed after heparinization. The role of perioperative systemic anticoagulation in the presence of a TIVS is not understood and is dictated by other bleeding site occurrences. 7
The objective of this report is to illustrate a new approach to the temporary restoration of perfusion during open management of extremity arterial injury. The authors present a different technique, named extracorporeal sheath shunt (ESS), that uses sheaths introducers instead of the commercial or the purpose-built shunts. ESS is a hybrid technique that can be used through surgical or percutaneous approaches. The percutaneous approach avoids transecting the proximal and distal control arteries, which may reduce the time of shunt creation and be limb-saving in patients with traumatic limb ischemia.
Cases
The extracorporeal sheath shunt (ESS) technique was performed in three cases of arterial lower limb trauma in the setting of type IIIC Gustilo fractures.
In the first case, a 59-year-old patient was transferred from a peripheral hospital with lower limb fractures caused by a tiller cultivator. The patient was at the site of the accident for 3 h and performed a self-bilateral intermittent tourniquet. Hospital admission occurred after 5 h. The patient was in shock and presented an exposed fracture of the left distal femur and leg bones with extensive soft tissue damage. This patient had a Mangled Extremity Severity Score (MESS score) of 11. AngioCT revealed left popliteal artery occlusion with recanalization in the tibioperoneal trunk and ankle posterior tibial (PT) artery. A TIVS was created between superficial femoral artery (SFA) and PT artery. The patient was submitted to fracture reduction, plate femur osteosynthesis and leg external fixation and we proceed with the harvesting of the great saphenous vein (GSV) in the contralateral limb to perform an SFA-PT bypass. At the 12th day, and due to tissue devitalization, the patient was submitted to left thigh amputation.
In the second case, a 19-year-old male patient was transferred from a peripheral hospital with lower limb fracture after a bike accident 7 h earlier. The patient was hemodynamically stable. This patient had a MESS score of 7. The angioCT revealed left tibial plates fracture and popliteal artery occlusion. The patient was submitted to anterior leg compartment fasciotomy and percutaneous tibial plate osteosynthesis. Transection of the popliteal artery was confirmed intraoperatively. A SFA-popliteal TIVS was created and we proceed with harvesting the GSV in the contralateral thigh to perform a SFA-popliteal bypass. The shunt was patent till the end of the procedure. In the postoperative period, the patient progressively improved motor function and healed the fasciotomies.
In the third case, a 25-year-old male patient was transferred from a peripheral hospital with an exposed fracture of the lower limb caused by a forklift 4 h earlier. The patient was hemodynamically stable. This patient had a MESS score of 5. The angioCT revealed a complex left tibial and fibular fracture, in the middle third, with misalignment and no opacification of leg arteries. The patient was submitted to tibial external orthopaedic fixation. A TIVS was created between the common femoral artery (CFA) and the PT artery and we proceed with harvesting the GSV in the homolateral limb. The patient was submitted to a venous graft in both anterior tibial (AT) and PT arteries. The peroneal artery was ligated. The shunt remained patent till the end of the procedure. In the postoperative period, the patient had improved sensitivity and motility.
The ESS technique
In all three cases, two 5-French sheath introducers with a length of 10 cm were used to create an external bypass circuit and restore arterial perfusion (Figure 1). The proximal introducer was placed in a retrograde fashion and the distal introducer in an anterograde fashion. Depending on the length of the shunt, a long intravenous extension line may be used. The distal introducer was always positioned under direct visualization, i.e. after surgical approach, at the site where the distal anastomosis was going to be placed. This allowed a controlled introduction of the sheath in the distal arteries, by avoiding complications such as puncture of the posterior wall or dissection at the puncture site. In two cases, a Fogarty catheter was used to guide sheath introduction as it provides more support than a hydrophilic guidewire. When surgically approached, the proximal arteriotomy performed for sheath placement was sutured with a 6.0 Prolene and the distal arteriotomy became the site of the distal bypass anastomosis.

External bypass circuit.
In the first case, the patient had a popliteal artery occlusion in P2. We surgically exposed the SFA and PT artery, and performed thrombectomy of the PT artery with subsequent heparinization. We punctured the SFA retrogradely and stabilized the sheath with a silk tie. In the PT artery, the sheath was introduced into the artery following an arteriotomy with the guidance of a Fogarty catheter (no. 2) that had been preloaded inside the sheath without its internal dilator (Figure 2). The introducer was stabilized with finger compression as a silk tie could traumatize the artery. We used two 5-French sheath introducers and a long intravenous extension line with two male luer lock connectors to create the external circuit (Figure 3). No systemic or local heparin was administrated during the procedure. The total dwell time was 2 h and we verified that the shunt had thrombosed by the end of the procedure.
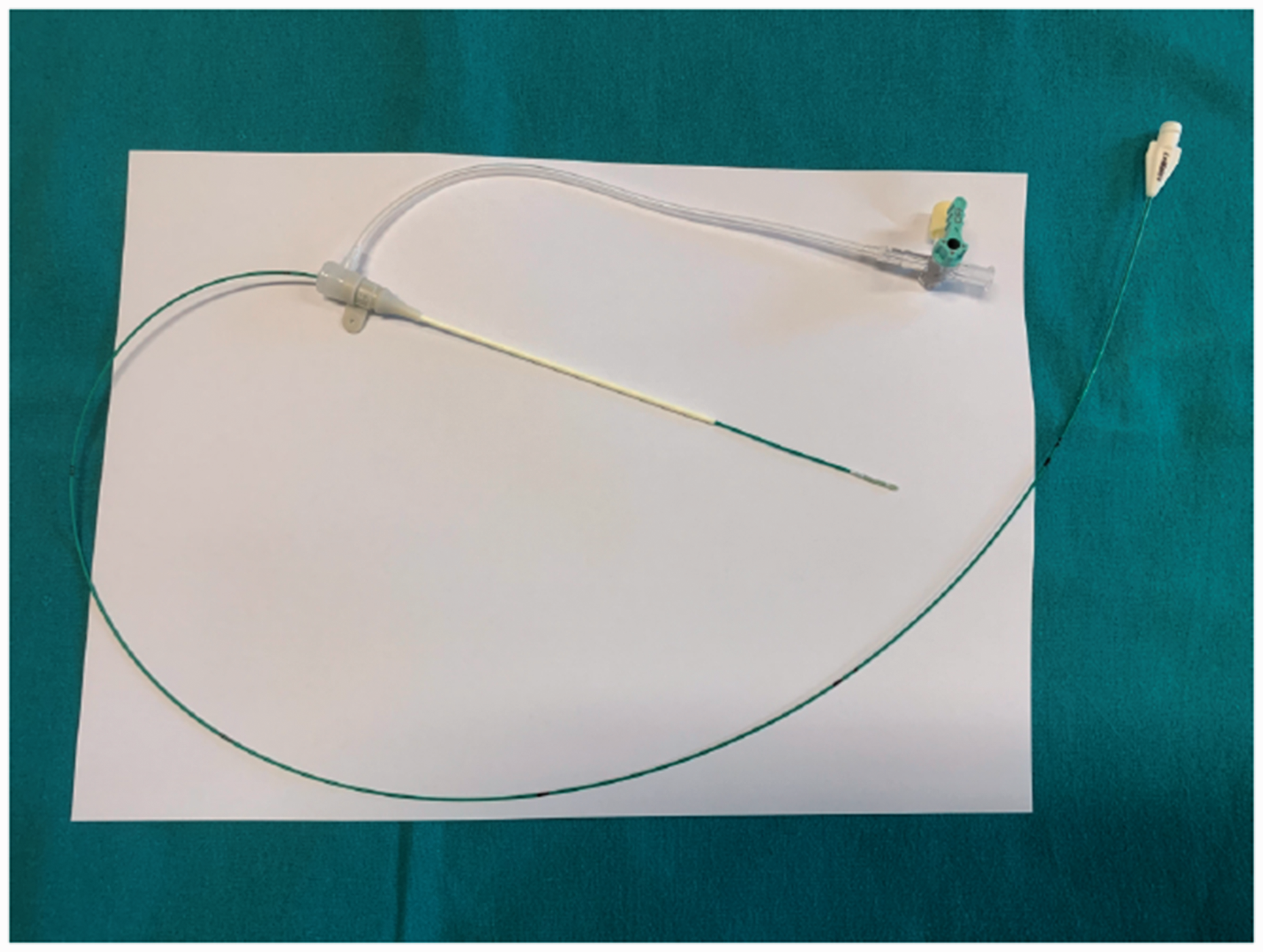
Fogarty catheter preloaded inside the sheath without its internal dilator.

Two 5-French sheath introducers and a long intravenous extension line with two male luer lock connectors.
In the second case, we performed a surgical approach of the SFA and popliteal artery (medial approach), where it was possible to confirm popliteal artery transection. SFA was retrogradely punctured and a sheath was introduced and stabilized with a silk tie. In the popliteal artery, after arteriotomy, the sheath was introduced through a Fogarty catheter (no. 3), without the dilator (Figure 2). The sheath was held in place with a silastic vessel loop and mosquito forceps to perform a tourniquet. A TIVS with two 5-French sheath introducers connected by the side port extensions was created (Figure 4). Two male luer lock connectors were used to connect both side ports, which were both females. No systemic or local heparin was administrated during the procedure. The total dwell time was around 1 h and 30 min. By the end of the procedure, the shunt was still patent.

Two 5-French sheath introducers connected by the side port extensions.
In the third case, the patient had transection of leg arteries. After surgical approach of ankle PT artery, we performed thrombectomy and heparinization. In this case, we directly introduced the sheath and did not use Fogarty to guide sheath introduction. The sheath was held in place with a silastic vessel loop and mosquito forceps to perform a tourniquet. Two 5-French sheath introducers and a long intravenous extension line with two male luer lock connectors were used to create the shunt between PT artery and CFA (Figure 2). However, in this case, we only performed surgical approach of the PT artery as the CFA was percutaneously punctured through ultrasound guidance. A three-way intravenous stopcock with male and female luer lock connectors was used and connected to the intravenous line, so it was possible to perform shunt heparinization and avoid shunt thrombosis. During the procedure, 15 cc of diluted heparin (5000 U in 100 cc of saline) was used to irrigate the shunt every 15 min. The total dwell time was 2 h and 45 min. The shunt was removed after performing AT artery graft and remained patent till the end.
In all cases, shunts remained in place until the proximal anastomosis was completed as the shunt was proximally placed to the proximal anastomosis, thus allowing the limb to remain revascularized as much time as possible. The shunt was removed when performing the distal anastomosis. Finally, in all patients, immediate limb reperfusion was verified through improved capillary refill time, distal venous refill and damaged vessel tissue haemorrhage. Also, progressive warming of the foot was noted.
Discussion
In the military field, TIVS is current practice and, therefore, there is more evidence supporting its use. 3 In civilian practice, despite lower evidence, most literature favours its use in selected cases.4–6 A similar concept has also been used in patients requiring venoarterial extracorporeal membrane oxygenation. Due to arterial femoral cannulation, acute inferior limb ischemia can occur in some patients. 8
TIVS placement in civilian trauma is commonly used during damage control of patients with the lethal triad (hypothermia, acidosis and coagulopathy) or as a temporary measure during orthopaedic fixation of bone fractures before limb revascularization.9 Moreover, shunts can offer a major benefit when transferring patients from hospital units without vascular surgery or trauma experienced surgeons by significantly reducing warm ischemia time. The three cases described were transferred from peripheral hospitals and warm time ischemia was at least 5 h until TIVS placement. The critical time interval for limb salvage due to limb ischemia is 6 to 8 h. In these cases, shunts allowed to reduce limb time ischemia (dwell times between 1 h 30 min and 2 h 45 min).
We performed a TIVS in patients with arterial laceration and after obtaining proximal and distal arterial surgical control. The creation of a TIVS involves arterial transection, which can be associated with shunt dislodgment or migration, some of the well-known complications. 9 We describe an approach (ESS) that avoids transection of the control arteries, which can reduce the aforementioned complications. As this technique can be performed percutaneously, one of its advantages is that it simplifies and shortens the time of shunt placement. When creating a shunt, the diameter of the shunt should be similar to that of the target artery, which might be difficult to encounter when using purpose-built shunts. Another advantage of this technique is that it avoids the mismatch between distal leg arteries and shunt size since the outer diameter of the introducer is approximately 2 mm. Understanding if patient’s blood loss is minimized with the ESS technique over conventional shunting would have been an interesting outcome; however, it was not possible to reliably address this question.
In all cases, we used a Fogarty catheter to guide sheath placement, as we experienced that it provided more support to advance the sheath, especially in small distal arteries. One could argue that there is a risk of arterial intimal lesion or dissection. However, we used reduced caliber introducers and the dilator outer diameter was similar to that of the Fogarty catheter.
In cases 1 and 3, an intravenous line was used as an adjunction to the introducers; in case 2 no intravenous line was used. Type of shunt, regardless of the material, has been shown to not influence clinical outcome and this includes intravenous lines. 6 Only case 1 presented with shunt thrombosis and the patient performed intermittent limb tourniquet for 3 h. In the emergency department, the patient was in shock and had a prolonged time ischemia. A long shunt from the SFA to the PT artery was created. We were unable to understand if the patient’s condition, length of the shunt or lack of heparinization was responsible for shunt thrombosis, as all these factors may have contributed to compromise its patency. However, we recall that the shunt was patent at a dwell time of 1 h and 45 min (total dwell time was 2 h), so it was patent almost till the end of the procedure. Overall, extensive soft tissue damage and associated infection contributed to major amputation, as the bypass remained patent in the postoperative period. Differently, in case 3, a long shunt from the CFA to the PT artery was also created, but we decided to perform frequent shunt heparinization and verified that it remained patent throughout the procedure.
The role of perioperative systemic anticoagulation in the presence of a TIVS is not usually performed since trauma patients are at or prone to a coagulopathic state. 7 Moreover, other trauma sites frequently restrict systemic heparinization. In these cases, we only performed local heparinization associated with thrombectomy and shunt heparinization. To our knowledge, even when using commercial intravascular shunts with flush side ports, there are no cases of shunt heparinization described. As such, the role of shunt heparinization is unknown. In cases where it is not desirable to give the patient heparin, another three-way intravenous stopcock can be placed next to the distal introducer. This allows heparinization of the intravenous extension line exclusively. In the postoperative period, patients were kept under low doses of anticoagulation and/or antiplatelet drugs. After discharge, patients were kept under single antiplatelet therapy.
The management of trauma patients is complex and there is still a lot to understand when dealing with vascular trauma. The main limitation of this paper is related to the paucity of cases, which difficult the conclusion of clinical outcomes. In our practice, intravascular shunts in civilian trauma are rarely used, despite having a positive outcome. Since most of our vascular trauma patients are transferred from other hospitals, we consider of major importance to reduce as much as possible time of limb ischemia.
Conclusion
The described technique may simplify TIVS placement since it can be performed percutaneously. This can reduce the time of shunt construction by avoiding artery surgical approach and facilitate the creation of TIVS among other than vascular surgeons and, hopefully, widespread its use.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.