
Abstract
Objectives
Behcet’s disease is a multisystem disorder of unknown etiology with vascular complications. This study reviewed the mid-term outcome of Behcet’s disease patients with carotid artery pseudo-aneurysms treated by endovascular stent-graft repair at our unit.
Methods
During a period of 11 years, six cases were included. Postoperative ultrasound duplex results were recorded along with computed tomography angiography report done a year after intervention.
Results
The mean age (±SD) was 38 (±5.2) years. The mean (±SD) pseudo-aneurysm size was 33 (±12.2) mm. Technical success was 83%; failed cannulation of the internal carotid artery was encountered in one case. On day 2 post-operative, a duplex ultrasound revealed complete exclusion and thrombosis of the false aneurysm in all cases. A year later, a computed tomography angiography revealed a primary patency rate of 80%, and only one case had a recurrent pseudo-aneurysm at the distal margin of the stent graft. All cases, however, had complete thrombosis in the pseudo-aneurysms lumen with a mean (±SD) regression in size of 18 (±6) mm. The mean (±SD) percentage of in-stent stenosis was 34.5% (±11.73%).
Conclusions
Stent graft repair for carotid artery pseudo-aneurysm in Behcet’s disease patients might be the preferable first line of treatment since it had a high technical success and mid-term primary patency rates, with additional fact that it obviously avoids the hazardous complications of surgery.
Introduction
Behcet’s disease (BD) is a multisystem disease of unknown etiology commonly found in Middle Eastern and Asian populations. 1 It may present with expanding aneurysms. 2 Aneurysms of the carotid arteries are infrequently reported; to our knowledge, 26 cases of carotid aneurysms due to BD have been reported.3–27 Rupture from carotid aneurysms is rare, and there are only two cases reported in the literature.23,25
The most commonly used criteria for diagnosis are those of the International Study Group for BD. 28 These require recurrent oral ulceration plus at least two of the following: recurrent genital ulcerations, eye lesions (such as uveitis), skin lesions (such as erythema nodosum or folliculitis), and a positive pathergy test. The pathergy test is a simple test in which the forearm is pricked with a small, sterile needle. The occurrence of a small red bump or pustule at the site of needle insertion constitutes a positive test.
There is no current consensus on the gold standard treatment for carotid pseudo-aneurysms in BD. Generally, aneurysms in BD respond poorly to medical treatment because of an apparent increased tendency to enlarge and rupture within a short time. 29 Although open surgical repair of these aneurysms is inevitable, BD patients are poor candidates for reconstructive arterial surgery because of the friable nature of the affected tissues, the potential risks of anastomotic pseudo-aneurysm formation (30–50%) as well as graft occlusion. 9 In attempts to avoid future pseudo-aneurysms at the anastomotic sites, suturing in healthy arterial segments is recommended, 22 an issue that is not always feasible in this pathology. Moreover, BD patients often have fibrosed saphenous veins owing to repeated attacks of superficial thrombophlebitis. 7 Adding to the complexity of the problem, some authors 30 have preferred synthetic grafts for bypass in these patients to avoid potential venous vasculitis that might cause late graft thrombosis. However, others 31 have found no difference in outcome between synthetic and saphenous grafts. Therefore, in order to potentially prevent complications from surgical repair, endovascular insertion of a stent graft has been suggested as a reasonable alternative. In this work, we present our experience in endovascular management of six BD patients with carotid artery pseudo-aneurysms.
Methodology
This study was approved by the Institutional Review Board of Alexandria University, on 30 October 2018. A retrospective study was done where BD patients treated by stent-graft exclusion for their carotid artery pseudo-aneurysms between 2007 and 2018 at Alexandria University Hospitals were included. All study subjects met the international study group criteria for the diagnosis of BD. 28 Table 1 shows the distribution of the criteria among the six study subjects. None of them had any previous open vascular repair of their aneurysms or suffered from end-stage renal disease. A computed tomography angiography (CTA) was done for all patients to set the plan of management according to the transverse diameter of both the common carotid artery (CCA) and the internal carotid artery (ICA) along with the pseudo-aneurysm site, size, neck size, and percentage of mural thrombus. Consent was taken after explaining the risks and benefits of the procedure and the possibility of the need for emergency conversion to open repair was clarified. All patients were subjected to rheumatological consultation and received immunosuppressive medications, starting at least one month prior to intervention in the form of pulsed high-dose steroid therapy (intravenous methylprednisolone 1 g/day for 4–5 days) followed by cyclophosphamide (intravenous 40–50 mg/kg divided over 2–5 days). Postoperatively, oral azathioprine (2–3 mg/kg/day) was administered to all patients until inflammatory markers (erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)) returned to normal levels and colchicine (1–2 mg/day) was given to all patients and was continued regardless of the inflammatory state. None of the patients were treated in the acute phase; this was accomplished by ensuring that ESR level was below 10 mm/h and CRP below 0.5 mg/dL.
Distribution of the international study group criteria for the diagnosis of BD among the patients.

All patients were managed by endovascular deployment of stent grafts under general anesthesia. This entailed an ultra-sound guided insertion of a 9 F sheath percutaneously into the groin after which 5000 IU of Heparin was administered intravenously. Then using a 0.035 hydrophilic guide-wire and a guiding catheter, the CCA was cannulated. Direct angiography was done to determine the proximal and distal landing zones. All stents used were FLUENCY Plus Stent Graft (Bard Peripheral Vascular, Tempe, Arizona, USA). Post-stent dilatation was not a routine practice; however, it was reserved only for those patients whom the completion angiography revealed filling of the pseudo-aneurysm from either ends of the stent graft. No Heparin reversal agents were used. All patients received therapeutic doses of low molecular weight heparin (LMWH) for two weeks and were kept on dual anti-platelet for life. No embolization protective devices were used during the procedures. No vascular closure devices (VCD) were used, alternatively, groin manual compression was done for at least 25 min.
On day 2 postoperative, all patients had a color duplex ultrasound (CDU) scan to verify exclusion of the whole pseudo-aneurysm and thrombosis of its lumen. After one year, all cases had a CTA to detect stent patency, any further aneurysmal formation or endoleaks, and to measure regression of the pseudo-aneurysm size and degree of lumen narrowing.
Results
Patients’ demography is summarized in Table 2. Six patients were included in the study; five were males. The mean age (±SD) was 38 (±5.2) years. Four cases had the pseudo-aneurysm originating from the ICA while two cases from the CCA. The mean (±SD) pseudo-aneurysm size was 33 (±12.2) mm.
Patients’ demography.
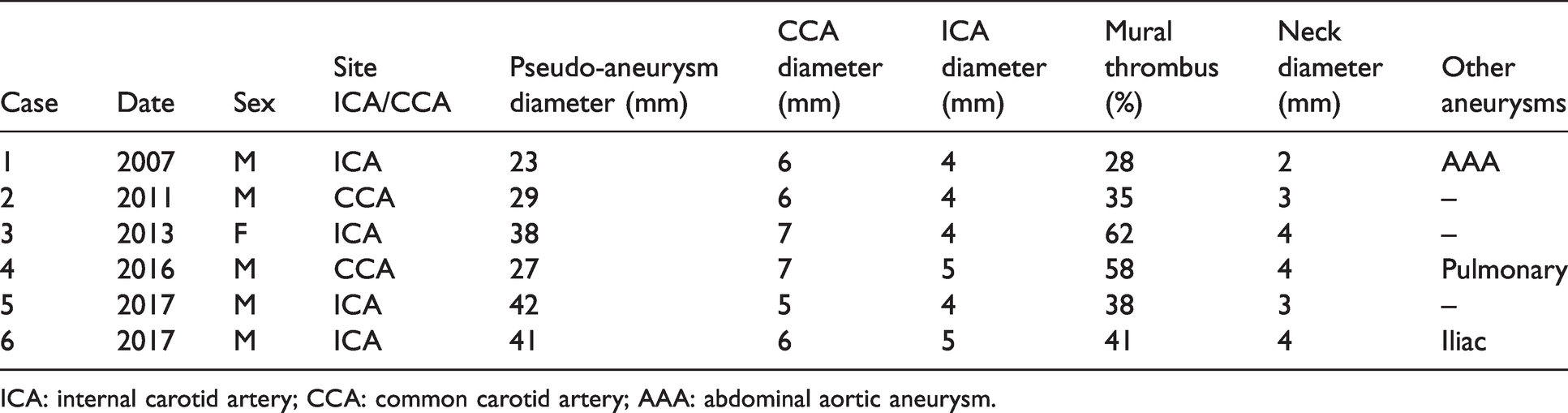
ICA: internal carotid artery; CCA: common carotid artery; AAA: abdominal aortic aneurysm.
Technical success was 83% (n = 5/6). In only one case with CCA pseudo-aneurysm (n = 1/6.17%), failure to cannulate the ICA was encountered; therefore, open surgical repair was resorted to in the form of aneurysm excision plus carotid artery repair by end-to-end anastomosis with suture line reinforcement by Teflon pledgets. Four patients had the distal landing zone of the stent deployed in the ICA; however, the patient with the CCA pseudo-aneurysm had it deployed in the CCA before the bifurcation. No embolization was done for the external carotid artery in any case of the ICA pseudo-aneurysms. As for the stent sizes, four cases had 9 mm diameter stents deployed and only one case had an 8 mm diameter stent used. All stents were 40 mm in length. None of the cases needed post-stenting dilatation. Figure 1(a) to (c) demonstrates the case of a left CCA pseudo-aneurysm treated by stent graft.
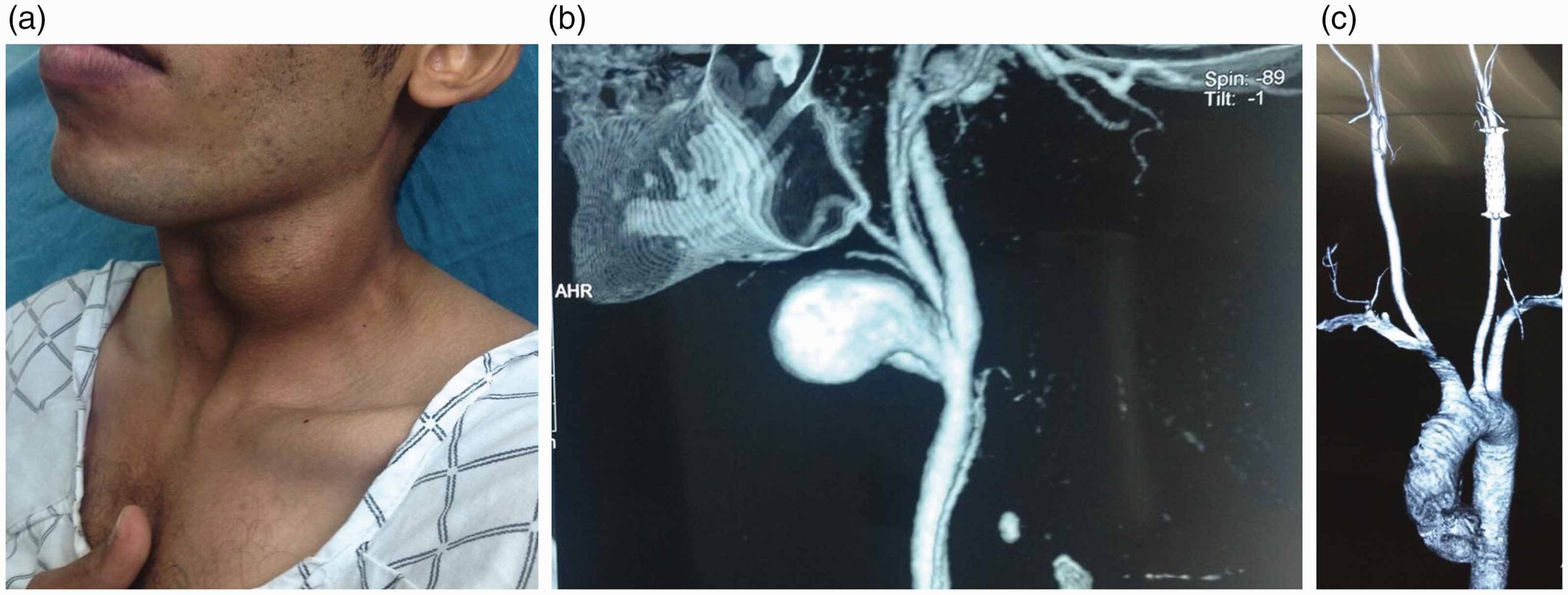
(a) Photo of left common carotid artery pseudo-aneurysm. (b) Computed tomography angiography scan. (c) Stent-graft successfully deployed.
Two patients had access site complications; one patient had a false aneurysm at the site of the groin puncture. He was followed up with CDU every three months and was not operated for his 2.2 cm groin pseudo-aneurysm. Another patient had the SFA thrombosed; he was managed conservatively after refusal of surgical thrombectomy and was discharged a week later with a viable limb.
Patients’ follow-up details are summarized in Table 3. On day 2 post-operative, a CDU revealed complete exclusion and thrombosis of the false aneurysm lumen in all cases. A year later, CTA revealed a primary patency rate of 80%; only one stent out of the five stents deployed was occluded. This patient was asymptomatic with rich intra-cerebral collaterals. He was kept on one anti-platelet medicine and one anticoagulant, and followed up by a CTA every six months without the need for any intervention during the first year. Only one case had a recurrent pseudo-aneurysm at the distal margin of the stent graft. This was a small-sized pseudo-aneurysm (11 mm) and had not caused any signs of refilling of the previously excluded lumen; thus, follow-up with a CDU every three months was recommended. The CTA also revealed complete thrombosis in all the pseudo-aneurysms lumen with a mean (±SD) regression in size of 18 (±6) mm and a mean (±SD) percentage of in-stent stenosis of 34.5% (±11.73%). None of the in-stent stenosis was hemodynamically significant, and thus, no secondary intervention was done to any of the cases.
Follow-up results.
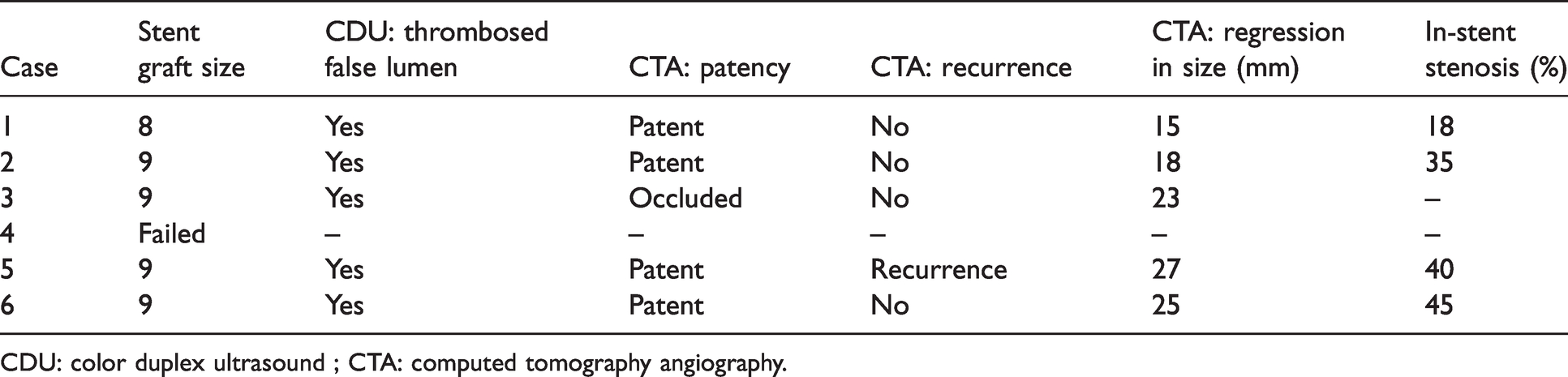
CDU: color duplex ultrasound ; CTA: computed tomography angiography.
Discussion
The study revealed that endovascular management of carotid pseudo-aneurysm in BD patients showed an 83% technical success rate and a one-year primary patency rate of 80%. Our methodology had a few limitations; the sample size of six subjects was relatively small to reveal countable data that could amend the practice in these cases. That being said, vascular practice in this part of the world – the Middle-East – allowed us to report a case series for a disease that is otherwise rarely seen in the western population. Additionally, it was not possible to compare between different types of stent grafts due to the unavailability of different types of stents at stock unit. Lastly, although the study period lasted for 11 years, a one-year period follow-up is a relatively short time to determine stent patency, fracture, late in-stent stenosis, and aneurysm recurrence in such a disease with chronic pathology. However, since the last two cases were done one year before the study was approved by the Institutional Review Board of the University of Alexandria, and to equally compare results with the previous cases done, we had to unify the period of follow-up.
As previously mentioned, according to availability, all five stent grafts used in this study were of the same type. Although normally there is an anatomical discrepancy between the CCA and the ICA diameters, there are no tapered stent grafts available in the market and no short-term complications were encountered from deploying the 9 mm stents in the 4–5 mm ICA. As regards the patient who had stent occlusion on follow-up, we believe that this is probably related to his active vasculitic state due to discontinuation of the immunosuppressive medications and not related to over-sizing or a particular anatomical issue or the fact that post-stent dilatation was not performed. This assumption is based on the idea that none of the other cases whom their stents remained patent after one year had post-stent dilatation. Meanwhile, all cases had the same range of stent sizes deployed (8–9 mm) that negates oversizing as a cause of occlusion. All stents were inserted percutaneously via a 9 F sheath into the CFA by ultra-sound guided approach. Neither groin cut-down nor VCD were used for fear of intimal injury in these friable arteries.
Open surgical repair of carotid artery pseudo-aneurysms in BD has been the sole modality of treatment before the endovascular era; however, results were not that promising. Tacal et al. 6 in 1993 reported a case of ICA pseudo-aneurysms in BD treated by resection and synthetic graft bypass that was thrombosed two weeks post-operative. In 2005, Hosaka et al. 32 reported their results for surgery on 10 BD patients operated on for various peripheral aneurysms over a period of 24 years. Five out of 21 grafts used got occluded and the incidence of formation of anastomotic pseudo-aneurysm was 12.9%.
To our knowledge, very few cases of carotid aneurysms in BD treated by endovascular techniques have been reported. Bonnotte et al. 12 in 1999 reported a case of a 30 mm ICA pseudo-aneurysm in a 47-year-old woman with BD that was successfully managed with a bare-metal stent and 19 coils for embolization. They reported a success period of four years with patent stent and no recurrence. However, we think that after more than 20 years now, treating carotid pseudo-aneurysms with such a technique is not well justified since it adds to the cost and carries a high risk of cerebral embolization. Early reports using covered-stents showed high rate of complications; in 2001, Park et al. 13 reported nine aneurysms related to BD, out of which only one case had a right CCA aneurysm treated previously by saphenous vein graft bypass that was complicated by two anastomotic pseudo-aneurysms after three months. He was then managed by two balloon expandable covered-stents (Jostent-graft; Jomed, Rangendingen, Germany) that became occluded after 28 months due to flow disturbance caused by double lesions. Kwon Koo et al. 15 in 2003 reported the use of a balloon-expandable Jostent stent-graft (Jomed, Helsingborg, Sweden) to treat a post-surgical recurrent carotid pseudo-aneurysm in a BD patient. Unfortunately, this patient stopped his immuno-suppressive medications and the stent was occluded within six months of implantation. From the last two mentioned reports one can understand that secondary re-interventions after open repair are not uncommon and although endovascular management is still feasible post-operative, it is not without complications. This is also supported by previous data reported on recurrence rate after surgical repair of peripheral aneurysms in BD reaching about 50%.11,33,34 However, other researchers have demonstrated promising results when using covered-stents in carotid aneurysms in BD. Ohshima et al. 21 in 2008 reported a case in which a covered stent was successfully used to treat a huge 6.5 cm CCA pseudo-aneurysm in a BD patient. An 8 × 60 mm stent graft was used, which kept patent for one year. A recent case report by Kassaian et al. 27 demonstrated the deployment of two overlapping Fluency self-expanding stent grafts (8 × 60 and 10 × 60 mm) in the CCA and ICA consecutively (Bard Peripheral Vascular, Tempe, Arizona, USA). Completion angiography revealed an iatrogenic dissecting flap, which was covered by a self-expanding 7 × 30 mm PRECISE Stent (Cordis, Johnson and Johnson, Miami, FL, USA). These stents were patent after six months on CTA.
Further studies are definitely needed in this area. There should be multi-central studies that involve sufficient numbers of patients in order to be able to yield valid international guidelines for such a rare disease. Future work should compare between different stent grafts in the market to allow vascular surgeons to provide the best care for the patients. Furthermore, the difference in patency between stent grafts deployed for pseudo-aneurysms in the ICA versus the CCA is unknown. Such a comparative study will aid interventionists in decision making. Finally, a consensus for post-operative anticoagulation/anti-platelets is clearly lacking, which calls for broad research in that respect.
Conclusion
The endovascular management of carotid pseudo-aneurysm in BD patients has a high technical success and mid-term primary patency rates. It also avoids the hazardous complications of surgery. We think it might be the preferable first line of treatment.
Footnotes
Acknowledgements
This work is presented at Leipzig Interventional Course (LINC) 2019, Leipzig, Germany, 22–25 January 2019.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.