
Abstract
Objectives
We aimed to evaluate emergency vascular complications of the lumbar disc reconstructive surgery in this study.
Method
Between March 2006 and February 2020, nine patients (six males and three females; mean age: 53.4 ± 9.6 years; range: 38–64 years) who underwent emergent vascular intervention during lumbar spinal disc reconstructive surgery in our clinic were included in this retrospective study.
Result
The left common iliac artery injury, the left common iliac artery and left common iliac vein injuries, bilateral common iliac artery and abdominal aortic injuries, and vena cava inferior injury with left common iliac vein and right common iliac vein injuries were detected in two, three, two, and two patients, respectively. In addition, 16 mm Dacron tube graft interposition and graft patch plasty were performed in one and two patients who had an abdominal aortic injury, respectively. Also, 8 mm polytetrafluoroethylene straight graft interposition was performed in two patients with left common iliac artery injury, and lateral wall repair was performed in other patients. Graft patch plasty and 8 mm polytetrafluoroethylene graft interposition were performed in one patient with vena cava inferior injury and left common iliac vein injury, respectively. Also, lateral wall repair was performed in other patients with venous injuries. Deep venous thrombosis had developed in three patients, and one patient of these had a pulmonary embolism.
Conclusion
The incidence of vascular injury after the lumbar disc surgery is relatively low; however, the emergency vascular operation should be performed as soon as possible.
Introduction
Major vascular injury is an important complication of spinal disc surgeries in the lumbar region which causes high mortality and morbidity. The incidence of vascular laceration during lumbar discectomy ranges from 0.01% to 0.17%. 1 Although major vascular injury is an unusual but well-recognized complication of vertebral disc surgery, 2 these complications may be serious. 3 On the other hand, Goodkin and Laska offered that its occurrence is probably more common than the medical community would expect. 4 The clinical course of developed vascular injuries is variable and can be divided into acute, subacute, and chronic, according to the duration of their appearance when they are detected. 5 Associated symptoms of this complication after the vascular injury may arise during the operation and/or immediately postoperative period. 6 This complication requires rapid diagnosis and emergency surgical treatment which can be life-saving. Moreover, prompt diagnosis and aggressive treatment can hope to improve the current mortality of more than 50%. 7
In this study, we aimed to evaluate emergency vascular complications of the lumbar disc reconstructive surgery.
Methods
Between March 2006 and February 2020, nine patients (six males and three females; mean age 53.4 ± 9.6 years; range: 38–64 years) who underwent emergent vascular intervention during lumbar spinal disc reconstructive surgery were included in this retrospective study. The medical records of the patients were reviewed and analyzed. Lumbar disc operations were performed by neurosurgeons in patients who had disc herniations at L4 ± L5 and/or L5 ± S1 intervertebral spaces (which was confirmed by magnetic resonance imaging). Physical examination was performed in the operating room after the requested vascular surgery consultation. Seven patients had deep hypotension (shock) during surgery and two patients had hypotension and unstable vital signs with active unstoppable bleeding in the operation site. All patients had tachycardia. Also, there were non-palpable lower limb pulses in patients with deep hypotension (shock), and there were weakening of these pulses in other patients. Emergency vascular intervention for iatrogenic injury of the abdominal vessels was simultaneously performed after the diagnosis was made based on the physical examination according to clinical suspicion during the lumbar disc operation without any further investigation. Blood products which were erythrocyte suspension, fresh frozen plasma, and fresh blood were used in patients with unstable vital signs, active bleeding, and hypotension after checking patients’ hemoglobin and hematocrit levels.
Results
Under general anesthesia, all patients were immediately turned supine position from the prone position, and emergency median laparotomy was performed. The retroperioneal fascia was cut vertically to explore the abdominal vessels. Inspection of all retroperitoneal vessels was made, and drainage of the retroperitoneal hematoma was successfully performed. Injured vessels were turned and hanged with vessel loops. Vascular clamps were placed proximal and distal to the injured site to control the bleeding after 5000 IU heparin was given for anticoagulation. Then, vascular repair of vessels was performed. One patient had only venous injury and five patients had only arterial injuries.
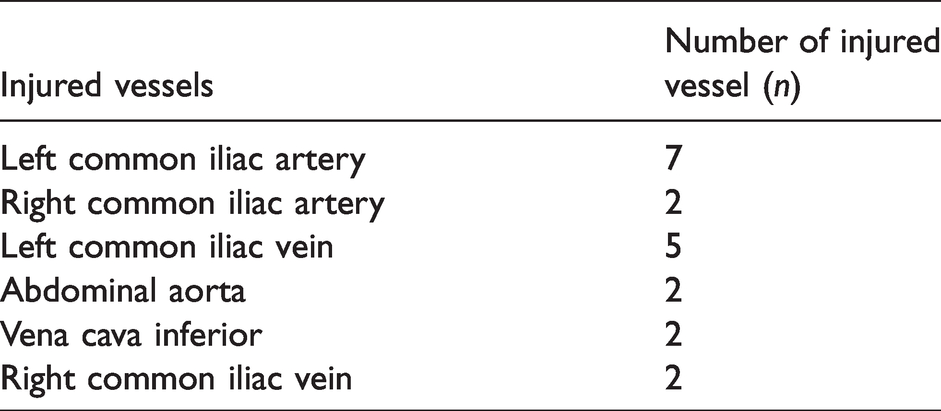
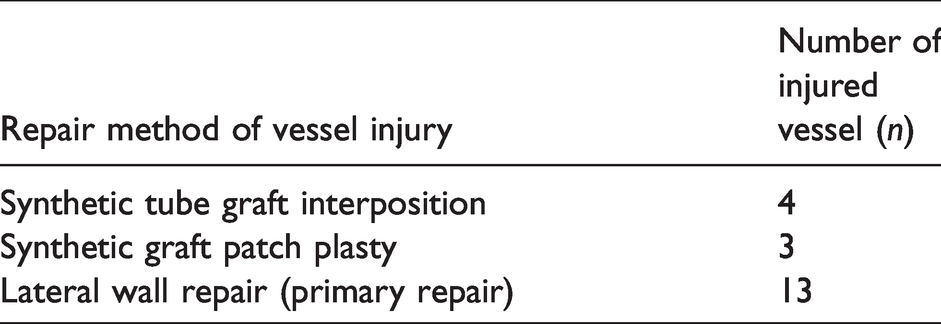
The left common iliac artery (CIA) injury, the left CIA and left common iliac vein (CIV) injuries, bilateral CIA and abdominal aortic injuries, and vena cava inferior injury (VCI) with left CIV and right CIV injuries were detected in two, three, two, and two patients, respectively. In addition, 16 mm Dacron tube graft interposition and graft patch plasty were performed in one and two patients who had an abdominal aortic injury, respectively. Also, 8 mm polytetrafluoroethylene (PTFE) straight graft interposition was performed in two patients with left CIA injury, and lateral wall repair was performed in other patients. Among patients with venous injuries, graft patch plasty and 8 mm PTFE graft interposition was performed in one patient with VCI injury and left CIV injury, respectively. Also, lateral wall repair was performed in other patients with venous injuries. Detected injured vessels due to lumbar disc surgery are shown in Table 1. Repair methods of vascular injuries are shown in Table 2 as well. In all patients, incisions were managed for bleeding and were completely closed. On the other hand, vascular injuries in three patients were eligible for endovascular intervention, but open surgery was preferred in these patients because the materials required for endovascular intervention were not available.
Detected injured vessels due to lumbar disc surgery.
Repair methods of vascular injuries.
Pulsatile arterial blood flow was detected in the control of the repaired arteries at the end of the vascular intervention. All patients were transferred to the intensive care unit after the operation. There were pulsatile pulses in the lower extremities in patients with arterial repairment in the physical examination. Then, they were transferred to the ward when their general condition improved and their vital signs became stable. The patients received 175 IU/kg/day low-molecular-weight heparin for three days in the early postoperative period. Then, antiplatelet therapy with acetylsalicylic acid 300 mg/day and/or clopidogrel 75 mg/day was given to all patients.
Deep venous thrombosis had developed in three patients during postoperative follow-up, and one patient of these had a pulmonary embolism. These patients were treated medically and healed. Two of these patients had left CIV injury and VCI injury with left CIV injury. Also, other patients developing deep vein thrombosis had only bilateral CIA injury and an abdominal aortic injury.
One patient died in the operation due to excessive bleeding who had left CIA artery injury and shock. During the follow-up period, patients’ vital signs remained stable, so the patients were discharged, and they were called to the outpatient clinic controls to perform magnetic resonance angiography or computed tomography angiography. The results were normal, which indicated that bypass grafts and repaired vessels were open, and their treatment was continued. Patients were followed up for approximately 24 ± 6 months. The longest follow-up was 96 months in one patient.
Discussion
Major vascular injuries in lumbar disc surgery can be seen in the abdominal aorta, VCI, and iliac vessels. Pillet et al. 8 offered that recording of the complications is underestimated, and their study results reduce the mildness reputation of lumbar disk surgery. Acute vascular complications can be manifested in the form of pre-shock and shock due to blood loss while the patient is still on the operating table. Fruhwirth et al. 9 reported that the risk of injuring the pelvic vessels intra-operatively can be explained by the close anatomical relationship between the retroperitoneal vessels and the vertebral column and furthermore not only by the fact that pre-existent deficiencies but also injury to the anterior longitudinal ligament give access to the retroperitoneal space. Most of the major vascular injuries are reported to occur during surgery either at the lumbar L4–L5 level or at the lumbar L5-sacral S1 level. 5 Bozok et al. 10 reported that the most frequent vascular injury is in the left CIA. The reason for this is the left CIA lies just in front of the L4–L5 level. 10 In addition, the left CIV can be injured. In that study, the authors also reported that left CIA injury was detected in 71.4% of patients, followed by the left CIV injury detected in 28.5% of patients. 10 We found that injuries to the left CIA and left CIV were in most of the patients in parallel with the literature. The pituitary rongeur is the usual cause of injury during disc surgery. 11 During disc removal, the rongeur may slip through the anterior longitudinal ligament and enter the retroperitoneal space of the abdominal cavity. 11 A deep bite can then injure the major vessels. 11 In this study, vascular injuries have emerged during the exploration and removal of the lumbar disc in the neurosurgical operation.
Clinical manifestation of such injuries may be extremely variable. 12 An isolated arterial laceration is the most common vessel injury and early manifestation can be seen in this injury due to retroperitoneal hemorrhage. On the other hand, there are often few external signs of blood loss in most patients and the diagnosis may not be recognized initially. Since the hemorrhage from vascular injury is generally hidden due to the absence of apparent bleeding in the retroperitoneal area, an anesthesiologist should carefully evaluate the changes in hemodynamic vital parameters, for example, blood pressure and heart rate during the surgery in order to prompt diagnosis. In addition, unexplained bleeding from the disc space not caused by epidural or bone bleeding, findings of fat, visceral or vessel wall in the specimen, and/or unexplained hypotension during surgery should lead the surgeon to suspect a vascular or visceral injury. 4
Acute blood loss may lead to sudden shock with the absence of femoral pulses, pallor, and decrease in the limb temperature. 5 This potentially fatal outcome which is associated with a mortality rate as high as 80%. 5 A high index of suspicion, a prompt diagnosis, and action will result in an improved patient salvage. 5 Therefore, the amount of bleeding from the patient should be followed up in the disc surgery, and blood products should be available before the surgery for possible vascular complications. Patients should be closely monitored postoperatively and evaluation of vital signs should continue in the intensive care unit and ward, especially in the first 24 h. The most important step is to make an early diagnosis and to switch to laparotomy immediately even in suspected cases.
On the other hand, especially in healthy young patients, hemodynamic changes will not occur without a 30%–40% loss in blood volume. In addition, bleeding may stop due to the buffer effect of internal organs or hematoma that may occur in vascular injuries. This is why the diagnosis of vascular injury could be missed in the surgery. Hemodynamic changes may occur in the wake-up room after extubation in such cases. If the patient has unstable vital parameters, the patient must be taken to the emergency operation. If the patient could tolerate, the diagnosis should be made by detailed physical examination and non-invasive and/or invasive radiologic imaging studies like arterial and venous Duplex Ultrasound, digital subtraction angiography, magnetic resonance angiography, and computed tomography angiography. Furthermore, the diagnosis may also be delayed for weeks or years due to formation of a pseudoaneurysm or an arteriovenous fistula which may be of gradual onset and produce initially only a few symptoms. 13 Moreover, Christensen and Bank reported an arteriovenous fistula complicating lumbar disc surgery. A case was presented in their study which the diagnosis was confirmed 18 months after a second lumbar disc operation. 14
In this study, mostly tachycardia and hypotension were detected and unstable vital signs with active unstoppable bleeding in the operation site, and non-palpable or weakened lower limbs pulses were also detected during surgery. Open surgical vascular intervention in the lumbar disc operation was performed to the suspected vascular injuries as soon as possible without any diagnostic investigation.
Kwinta et al. 1 reported that in the an era of minimally invasive surgery and interventional radiology, the frequency of endovascular procedures is still unexpectedly low. The emergency open surgical approach was preferred instead of minimally invasive surgery to prevent unnecessary delay, and this was compatible with the literature.
Conclusion
As a result, vascular injury to the major vessels is a potentially serious complication associated with lumbar disc surgery. The incidence of this complication is relatively low; however, the emergency vascular operation should be performed as soon as possible after the diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.