
Abstract
Objectives
To evaluate the safety and feasibility of microwave ablation for treating venous malformations (VMs) with severe localized intravascular coagulopathy (LIC).
Patients and methods
Data for patients with the diagnosis of VMs coupled with severe LIC who underwent color Doppler-guided microwave dynamic ablation between January 2017 and June 2019 were retrospectively reviewed and analyzed. All patients had previously received sclerotherapy or other treatments with poor outcomes and gradual aggravation of coagulation abnormalities. Microwave treatment with “dynamic ablation” was performed with real-time color Doppler monitoring and was repeated if necessary after 3 months. Low-molecular-weight heparin (LMWH) was used to control consumptive coagulopathy. The therapeutic efficacy including coagulation function and lesion size was evaluated using the four-level scale developed by Achauer.
Results
Among 15 patients with extensive diffuse or multiple VMs, 10 patients presented with lesions in a single lower extremity, one in both lower extremities and the perineum, one in both upper extremities and the trunk, and three with multiple lesions. The patients underwent a total of 74 microwave ablation sessions, with an average of 4.9 sessions per person. Coagulation abnormalities were temporarily aggravated in 59 sessions within the first seven days post-ablation but improved to grade II (fair) a week later. From six months to three years after the ablation, the lesions improved to grade IV (excellent) in one patient, grade III (good) in six patients, and grade II (fair) in eight patients. Moreover, the coagulation function improved to grade IV in four patients, grade III in eight patients, and grade II in three patients, resulting in an efficiency rate of 80% (12/15). Post-ablation complications included fever, hemoglobinuria, and elevations in aspartate aminotransferase, lactate dehydrogenase, and alanine aminotransferase. The patients with fever and hemoglobinuria recovered after specific therapeutic measures, but elevations in aspartate aminotransferase, lactate dehydrogenase, and alanine aminotransferase recovered spontaneously without further interventions.
Conclusions
Ablation coupled with anticoagulation can effectively treat VMs in patients with severe LIC and improve the long-term coagulation function.
Keywords
Introduction
Venous malformations (VMs) are some of the most common vascular anomalies, with an incidence of approximately 0.01–0.02%. 1 Clinically, the thin-walled and deformed vascular pathologies present as either bluish or purplish lesions localized on the skin and mucosa of various organs. Most VMs are asymptomatic; however, expending or diffusing vascular lesions can easily lead to cosmetic disfigurement and organ dysfunction as the lesions progress.2–5
Abnormal blood flow in extensive and complicated VMs induces coagulation and causes localized intravascular coagulopathy (LIC),5,6 which clinically presents with spontaneous thrombus formation and fibrinolysis, as indicated by an increase in D-dimer levels, a decrease in fibrinogen (FIB), and the consumption of coagulation factors. Therefore, severe LIC bears a high risk of pulmonary embolism and poses a challenge to treatment.6,7
Inappropriate manipulations during sclerotherapy or other interventions may trigger the conversion of LIC to diffuse intravascular coagulopathy (DIC), endangering the life of patients.8,9 To date, only a handful of reports exist in the literature on the management of severe LIC. A few therapeutic modalities for the treatment of severe LIC have been proposed such as sclerotherapy, but the use of microwave ablation has not been reported. From January 2017 to June 2019, we used microwave ablation to treat 15 patients with VMs with severe LIC. Based on our experiences, we designed this retrospective study to evaluate the clinical effects and side effects of microwave ablation for the treatment of VMs with severe LIC.
Materials and methods
Selection of Patients
The medical records of all patients were retrospectively reviewed, and the demographic information was retrieved from the records. The diagnosis of VM was established by clinical evaluation with magnetic resonance imaging (MRI), which showed multiple small phleboliths as round hypointense signals of different sizes. A diagnosis of LIC was established for VM with D-dimer levels greater than 0.5 mg/L; however, the diagnostic criteria for VMs with severe LIC included both obviously elevated D-dimer levels (greater than 10 mg/L) and a decreased FIB level (less than 1.5 g/L, BD-Compact-X). Patients were excluded from this study if they presented with malignant tumors, infection, thrombosis, and VMs combined with other vascular malformations.
Preoperative preparation
Routine preoperative workups consisted of chest plain film, electrocardiogram (ECG), complete blood count (CBC), chemistry, liver function, kidney function, blood glucose, coagulation tests, and D-dimer level. The study was approved by the hospital research ethics committee, and all participants signed informed consent forms for the ablation procedure. Before ablation, a multidisciplinary team (MDT) developed an ablation plan that highlighted the location and scope of ablation.
Microwave ablation procedure
For the thermal ablation procedures, the MTC-3C microwave ablation system (Nanjing Weijingjiuzhou Medical Equipment Research and Development Center) with an MTC-3CA-II16 (diameter 1.6 mm) cool-tip microwave ablation needle (electrode) was used with an ablation power of 35–55 W. The LOGIQ E8 color Doppler ultrasonic diagnostic apparatus (General Electric, United States) was used at a frequency of 3–12 MHz for real-time monitoring and guidance.
All ablation treatments were performed under general anesthesia. Before the ablation, a color Doppler scan of the designated area was performed to determine the extent and depth of the lesions and adjacent vessels and nerves. The nerves were mapped with ultrasound to avoid injury. Nerves appeared as characteristic mesh patterns in the color ultrasound cross sections and always ran continuously at the same anatomical sites, which were mapped by experienced ultrasonographers. In addition, color ultrasound provided information on different sections and directions. Afterward mapping the nerves, the ultrasonic probe was adjusted to a real-time setting to help surgeons determine the depth and direction of the ablation needle.
During the process of ablation, the ablation needle was first inserted at approximately 2 cm from the lesion, through the lesion, and 1 cm beyond, with real-time color Doppler monitoring and guidance. Once the needle was in place, the ablation instrument was turned on at a power of 35 W to vaporize the lesions around the back of the needle tip (about 1.0 cm). If the lesions were not immediately vaporized, the power was increased to ensure the occurrence of vaporization, which lasted for 20 s–60 s. Afterward, the needle was withdrawn by 1 cm and fixed in the same position while the ablation continued. The ablation time varied based on the blood flow in the lesions; however, the actual ablation time was dependent on the real-time monitoring results. Once the ablation completed, the needle was withdrawn to the proximal end of the lesion and then inserted into an adjacent lesion through the same puncture point to repeat the next round of ablation as described above. The key operating strategy focused on the application of ablations through the same puncture point in different directions, forming an umbrella-shaped ablation area, as shown in Figure 1. (a) Schematic diagram of ablation technique, sagittal view. Positions of three different levels of puncture needles from deep to superficial layer. The ablations were performed sequentially from 1 to 2 to 3. (b) Schematic diagram of ablation technique, overlooking position. Positions of the puncture needles at three different directions from the center to the edge. The ablations were performed sequentially from 1 to 2 to 3.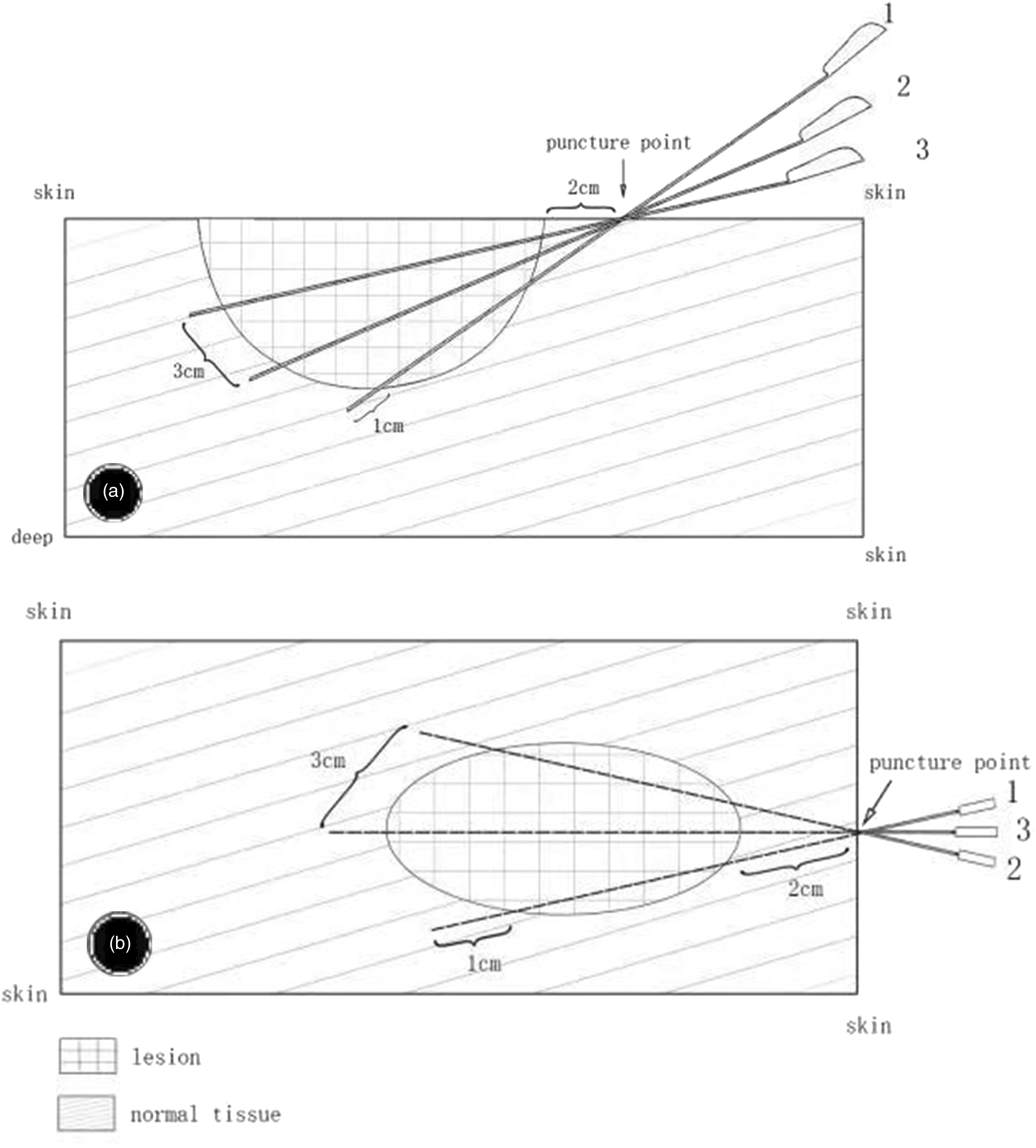
According to the scope of the lesions, three or four puncture points were created for one round of ablation. An average power of 45.0 W (ranging from 35 to 55 W) was used to ablate the lesions, with an average ablation time of 40.5 min and a range of 30–60 min. The next treatment was repeated after an interval of three months.
Post-ablation treatment
Low-molecular-weight heparin (LMWH, nadroparin calcium injection, Glaxo Wellcome Production, France) was subcutaneously injected twice a day at a dose of 100 units/kg for a total of seven to 10 days. Coagulation indicators and routine blood parameters were consecutively monitored during the treatments. For patients with increased menstrual volume, oral estrogen (estradiol valerate tablet from the Guangzhou Branch of Bayer Healthcare Co. Ltd, China) was prescribed at a dose of 2 mg three times a day for a total of seven days to promote uterine wound repair. For fever presentations, hydroprednisone (Jiangxi Sinopharm Co. Ltd, China) was administered intravenously at a dose of 0.5 mg/kg once a day for three consecutive days. Afterward, half of the dose was administered and the treatment was discontinued three days later.
Observation and follow-up
During the immediate postoperative period, body temperature, bleeding at the puncture point, skin ecchymosis in the ablation area, skin or tissue necrosis, and motor and sensory functions of the peripheral nerves in adjacent areas were carefully monitored for all patients. From the first day after surgery, coagulation tests and D-dimer levels were checked every three to five days. Three days after surgery, liver and renal functions were examined.
During the follow-up period, coagulation function, postoperative D-dimer levels, and liver and renal functions were evaluated one and three months postoperatively. MRI was performed to evaluate the lesion size every six months.
Criteria for the evaluation of therapeutic efficacy
Therapeutic efficacy was evaluated according to the coagulation function and lesion size. The lesion size was evaluated through physical examinations, and the MRI findings were used to classify the changes in lesion sizes based on the four-level classification system introduced by Achauer as follows 10 : grade I (poor), the lesion size decreased by 0–25%; grade II (fair), 25%–50%; grade III (good), 50%–75%; and grade IV (excellent), 75%–100%. The coagulation function was also evaluated and classified with Achauer’s system: grade I (poor): D-dimer level (immune turbidimetry) decreased by 0–25% and FIB was <1.0 g/L (BD-Compact-X); grade II (fair): D-dimer level decreased by 25%–50% and FIB was ≥1.0 g/L but <1.5 g/L; grade III (good): D-dimer levels decreased by 50%–75% and FIB was ≥1.5 g/L but <1.84 g/L; and grade IV (excellent): D-dimer levels decreased by 75%–100% and FIB was ≥1.84 g/L. The efficiency rate for the improvement of coagulation function was calculated using the following equation: (number of grade III cases + number of grade IV cases)/number of cases treated × 100%.
Results
Demographics of the patients.

All patients previously underwent sclerotherapy or other treatments several times with poor clinical effects and gradual aggravation of coagulation abnormalities. One patient developed a non-healing wound and frequent bleeding from an injury in the soft tissue of her lower limb, while two patients had increased menstrual flow, one of whom had excessive or prolonged bleeding and came to our hospital for emergency treatment. All 15 patients had low preoperative FIB levels (less than 1.5 g/L), and eight had FIB levels less than 1.0 g/L (minimum 0.52). Preoperative D-dimer levels were greater than 10.0 mg/L (maximum 124.4 mg/L).
All patients required hospitalization for a median of 10 days, ranging from 5 to 20 days. Fifteen patients underwent a total of 74 sessions of microwave ablations; one had three sessions, three had four sessions, seven had five sessions, and four had six sessions. The bleeding stopped in three patients within one week after the first ablation. Short-term evaluation of the coagulation function showed remission 14 days after the operation. Bleeding in the knee of a patient with knee contusion stopped five days after surgery and the wound healed two months later, whereas uterine bleeding stopped in the patients with increased menstrual flow six and seven days after surgery. Temporary coagulation abnormalities were aggravated 1 to 7 days after treatment in 59 sessions, reaching grade II (fair) 1 week after medical treatment.
After 6 months to three years of follow-up, postoperative evaluation of the treatment efficiency using MRI according to the changes in the lesion size showed one case of grade IV, six cases of grade III, eight cases of grade II, and zero cases of grade I lesion sizes. Further, in the evaluation of the coagulation functions, four grade IV, eight grade III, three grade II, and zero grade I cases were found, resulting in an effective rate of 80% (12/15) for post-ablation improvement of coagulation. The postoperative median D-dimer level was 6.9 mg/L (ranging from 1.2 to 20.1), compared to a preoperative median of 24.9 mg/L (ranging from 10.1 to 124.4). The postoperative median FIB level was 1.80 g/L (ranging from 1.45 to 2.89), compared to a preoperative median of 0.91 g/L (ranging from 0.52 to 1.45).
Eleven out of 15 patients developed a fever (body temperature above 37.2° Celsius) during the ablation treatment and subsequently recovered after symptomatic treatment with intravenous hydroprednisone as described earlier. Nine patients presented transient gross hemoglobinuria and recovered with therapeutic measures including hydration, diuresis, and alkalized urine. Seventeen patients exhibited significant increases (more than 100 U/L) in aspartate aminotransferase and lactate dehydrogenase, with a slight elevation (greater than 40 U/L, but less than 100 U/L) in alanine aminotransferase, but all recovered without any treatment. Skin lesions, tissue necrosis, and nerve damage could not be identified postoperatively.
Typical cases
Case 1
A 16-year-old girl with multiple VMs (more than 30 lesions) concomitant with LIC was brought to our department. The extensive VMs involved the chest, abdomen, limbs, head, neck, etc. (Figures 2(a), (c), and (e)). Microwave ablation and LMWH were performed to treat the VMs. After five sessions of ablation, multiple lesions disappeared (Figures 2(b), (d), and (f))), and the coagulation function was significantly improved. Her D-dimer levels decreased from 12.5 mg/L to 3.1 mg/L, and her FIB levels increased from 0.91 g/L to 2.28 g/L. Lesion size evaluation revealed a regression to grade III (good), while coagulation function evaluation revealed an improvement to grade IV (excellent). (a) Multiple masses in the back of a patient before treatment. (b) Disappearance of the masses after treatment. (c) Protrusion of an abdominal mass. (d) Disappearance of the abdominal mass after two ablation sessions. (e) Before treatment, MRI showed multiple hyperintense signals in the abdominal wall and bilateral retroperitoneal fossa iliaca on T2-weighted images ( ). (f) After treatment, MRI showed the disappearance or shrinkage of multiple hyperintense signals at the same locations (
). (f) After treatment, MRI showed the disappearance or shrinkage of multiple hyperintense signals at the same locations ( ).
).
Case 2
A 5-year-old girl presented with extensive VMs concomitant with LIC on her right thigh and perineum (Figures 3(a) and (c))). The lesions were significantly reduced after four sessions of ablation, and the circumference of the middle and lower thighs decreased by 5 and 6 cm, respectively (Figures 3(b) and (d))). Her D-dimer levels decreased from 124.4 mg/L to 6.9 mg/L, and her FIB levels increased from 0.63 g/L to 1.75 g/L. Her post-ablation lesion sizes were recorded as grade II (fair), and her coagulation function improved to grade III (good). (a, c). Appearance pretreatment ( ). (b, d) After treatment, the lesion was significantly shrunken and the circumference of the thigh was significantly reduced (
). (b, d) After treatment, the lesion was significantly shrunken and the circumference of the thigh was significantly reduced ( ).
).
Discussion
Large and/or deep VMs present with spontaneous thrombosis and thrombolysis. This presentation is known as LIC and manifests with a palpable phlebolith with localized pain as well as significantly elevated D-dimer levels. The D-dimer levels of patients with this condition are often very high, at >1.0 mg/L in some cases, and are used as a pathognomonic marker for LIC. Normally, LIC has minimal impact on the day-to-day activities of patients; however, a few patients are at risk of potential aggravation of LIC to DIC with dramatic bleeding and systemic thromboembolism during a surgical intervention. Mazoyer E et al. reported that coagulation disorders in LIC patients are worsened due to surgery, trauma, menstruation, and sclerotherapy.11–13 In this series, two patients experienced increased menstrual flow.
Most VMs with LIC are diffuse; thus, open surgery and even resection of some small superficial lesions are not recommended. In 2017, Hung JW 14 reported the case of a patient who underwent sclerotherapy, which reduced the number of lesions and significantly improved the coagulation function. Dompmartin A et al.15,16 also recommended sclerotherapy to treat LIC. In a study by Mason KP et al., 17 sclerotherapy reduced the volume of the lesions but aggravated coagulation abnormalities. Mack JM and others 18 reported that sirolimus therapy can significantly decrease the D-dimer levels of patients and improve coagulopathy. The application of LMWH or dabigatran etexilate can only improve coagulation function in the short term.19,20
Non-invasive therapy including sclerosis therapy and anticoagulants may improve short-term coagulation function, but the effects on long-term lesion reduction and improvement of coagulation function remain uncertain. To date, effective therapy to control the size of VMs and improve long-term coagulation is still lacking. The ideal treatment method should not only reduce the volume of the lesion by stages but also avoid the aggravation of coagulation disorders.
In this cohort, all patients were diagnosed with severe coagulation disorders, which eliminated surgical intervention as a treatment option. Perioperative D-dimer levels were greater than 10.0 mg/L, with the maximum level reaching 124.4 mg/L, and FIB levels were less than 1.5 g/L (minimum 0.52 g/L). Before admission to our hospital, these patients had undergone sclerotherapy several times with poor outcomes. Therefore, effectively removing or destroying the latticed VM lesions and reducing the consumption of coagulation factors in the lesions are two key problems that should be addressed in LIC treatment.
Since the 1990s, minimally invasive surgery (MIS) has been conceptualized and popularized for the management of various disease entities. Following the principle of MIS, ablation as one of the most advanced MIS techniques has been widely adopted for the treatment of various solid tumors, including lung, liver, uterine, and thyroid tumors.21–25 Recently, this technique was introduced into the field of vascular malformation treatment. 26 Technologically, microwave ablation involves the use of a needle as the transmitting antenna to vaporize and ablate lesions located approximately 1.0 cm behind the tip of the needle. Some advantages of microwave ablation have been noted, such as minimal invasion, a less demanding procedure for the operator, accurate range of action, ease of avoiding nerve injury, and a lower chance of thermal damage caused by the plate electrode.
In the treatment of LIC, microwave ablation can quickly cause the local latticed venous lesions to shrink, retract, and harden but not destroy coagulation factors in the lesions. In this cohort, the post-ablation changes lesion sizes were evaluated as grade IV (excellent) in one patient and grade III (good) in six patients. The efficiency rate for the improvement of post-ablation coagulation function was 80% (12/15). Coagulation disorders were slightly aggravated within a week after treatment, but remission was quickly achieved after the patients received short-term anticoagulation treatment (LMWH). Three patients with hemorrhage stopped bleeding within one week after one ablation session. Short-term evaluation of the coagulation function revealed primary remission within 14 days after ablation. Short-term application of nadroparin calcium is an important auxiliary method to treat coagulation disorders. In a word, microwave ablation combined with short-term LMWH administration can reduce the volume of the lesion effectively without seriously aggravating coagulation disorders, which enables continual ablation to further increase the treatment efficacy.
It should be noted that LMWH cannot destroy VM anomalies; hence, it is not an effective treatment modality for improving long-term coagulation function. Further, since the long-term application of LMWH can induce heparin-induced thrombocytopenia (HIT), the use of LMWH for more than three weeks is not recommended. All patients in this series were treated with LMWH (nadroparin calcium injection) for less than 3 weeks, and thrombocytopenia was not observed.
Post-ablation complications consisted of hyperpyrexia, transient hemoglobinuria, and abnormal liver function. No related complications, such as skin ulceration, tissue necrosis, or nerve damage were encountered. The absorption of necrotic tissues may cause postoperative fever, and hydroprednisone can be used as the treatment. Liver dysfunction mainly manifests as an increase in glutamic-oxalacetic transaminase and lactate dehydrogenase, with a slight elevation of glutamic-pyruvic transaminase. Transient hemoglobinuria should be taken seriously; in severe cases, it can block the small tubes in the kidney and induce acute renal failure. Hydration, diuresis, and alkaline urine should be applied during and after surgery.
In conclusion, VMs with severe LIC are difficult to manage. Inappropriate surgery or sclerotherapy may induce the aggravation of coagulation disorders and even facilitate progression to DIC, endangering the patient’s life. In this study, we reported a series of cases involving the treatment of severe LIC. We successfully performed microwave ablation on patients with VMs combined with LIC. As the number of treatment sessions increased, patients with severe coagulation disorders gradually experienced long-term improvement and remission. Additionally, anticoagulation with LMWH and the provision of coagulation factors are effective in alleviating the temporary aggravation of coagulation disorders during the perioperative period.
As a descriptive study, this case series inherited several pitfalls such as a small sample size, selection bias, and lack of a comparator for internal validity as well as hypothesis verification, all of which limit the application of our diagnostic and therapeutic methods in this series.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.