
Abstract
Introduction
The aim of this study was to evaluate the influence of pedal arch quality on 5-year survival and limb salvage in diabetic patients with foot wounds undergoing peripheral angiography.
Methods
Between January 2014 and December 2014, 153 diabetic patients with foot wounds underwent peripheral angiography. Final foot angiograms were used to allocate patients according to pedal arch: complete pedal arch (CPA), incomplete pedal arch (IPA), and absent pedal arch (APA). Five-year survival and limb salvage rates were analyzed with Kaplan–Meier curves and compared by means of Gehan–Breslow–Wilcoxon test. Associations of patient and procedure variables with overall survival and limb salvage outcomes were sought with univariate and multivariate analyses.
Results
A below-the-knee (BTK) artery was the target vessel in 80 cases (52.3%). Five-year Kaplan–Meier rates of survival were similar in all groups (p = 0.1): CPA 30%, IPA 27.5%, and APA 26.4%. Five-year limb salvage rates were significantly better in patients with CPA/IPA (p < 0.001): CPA 95.1%, IPA 94.3%, and APA 67.3%. In the whole population study, multivariate analysis showed significant association of smoking (p = 0.01), chronic renal failure (p = 0.02), and severity of foot wounds (p < 0.001) with survival. Coronary artery disease (p = 0.03), severity of foot wounds (p = 0.001), and pedal arch status (p = 0.05) showed strong association with limb salvage.
Conclusions
Pedal arch quality significantly affected limb salvage but not survival at 5 years in patients with diabetic foot ulcers. Smoking, chronic renal failure, and severity of foot wounds affected overall survival, whilst coronary artery disease, and severity of foot wounds limb salvage.
Introduction
There is a global burden of diabetic foot disease. 1 The epidemiological growth means a financial burden too. 2
The majority of diabetic foot ulcers (DFUs) are preventable. 3 However, when a foot wound develops, the risk of death for diabetic patients is 12.1 per 100 person-years. 4
Recent articles reported that the overall 5-year mortality associated with DFUs is up to 35%.5–7 Mortality and direct costs of care are comparable to cancer. 5 In addition, diabetic patients with foot wounds fear major lower extremity amputations more than death. 8 Incidence of all forms of lower extremity amputation ranges from 46.1 to 9600 per 100,000 in the population with diabetes. 9
Several factors have been associated with increased risk of mortality and major amputation, including age, sex, chronic kidney disease, and coronary artery disease.10–12
In diabetic patients with ischemic ulcers no “morphological” data has been strongly associated with the long-term risk of death and limb loss. However, vascular involvement in diabetic patient is diffuse and aggressive in the below-the-knee (BTK) arteries with high percentages of long occlusions. 13
In the last years, there was a great interest not only in the tibial vessels but also in the foot vessels.14,15 Pedal arch patency seems to affect tissue loss and time to healing. 16 However, no impact of pedal arch quality on the long-term clinical outcomes in diabetic patients has been well established.
The aim of this study is to evaluate the effect of pedal arch quality on 5-year survival and limb salvage in diabetic patients with foot wounds undergoing peripheral angiography.
Methods
Population study
Between January 2014 and December 2014, 153 consecutive patients with DFUs underwent peripheral angiography at our center for Vascular Surgery including two tertiary care hospitals.
All endovascular interventions were performed in a hybrid operating room under local anesthesia. The endovascular procedure was tailored on each patient on the basis of the preoperative diagnostic assessment consisting of wound examination and Duplex scan; a computed tomography (CT) scan was performed in the presence of suspected aorto-iliac lesions.
Technical success was defined as the restoration of flow in the target vessel directly to the foot (“in-line flow”) without residual stenosis >30% or flow-limiting dissection.
All patients gave their written consent to the procedure.
The grade of ischemia was classified according to Rutherford classification. 17
Wounds were globally classified according to Texas University Classification (TUC) 18 and WIfI (Wound Ischemia foot Infection) classification. 19
When suspected, infections were preoperatively diagnosed with a specimen for aerobic and anaerobic cultures (swabs for fluid cultures). Wound infections were classified according to Infectious Diseases Society of America (IDSA) classification. 20
Pedal arch: three groups
Final angiograms of the foot were used to allocate the patients into three groups according to status of pedal arch: complete pedal arch (CPA-group), incomplete pedal arch (IPA-group) and absent pedal arch (APA-group).
The CPA was defined when both dorsalis pedis artery and at least one of the plantar arteries are patent and joined each other; the IPA was defined when the dorsalis pedis artery or one of the plantar arteries are patent but not joined each other; and APA was defined when neither dorsalis pedis artery nor at least one of the plantar arteries are patent but the circulation of the foot was instead established through collateral vessels (Figure 1). Pedal arch status: CPA (left), IPA (middle), and APA (right). PedA, pedis artery; Arch, pedal arch; PlaA, plantar artery. Note: CPA: complete pedal arch; IPA: incomplete pedal arch; APA: absent pedal arch.
A successful foot revascularization was defined as the restoration of flow inside the pedal arch with a re-established connection between the dorsalis pedis artery and one or both the plantar arteries.
Timing of patients’ evaluation
Patients’ vascular surveillance included a clinical examination and duplex ultrasound scan in the following steps of the study: pre-procedural, 1 month, 6 months, 1 year, and yearly thereafter.
In the present study, all patients lost at follow-up received a phone interview at 5 years from the index procedure in order to obtain data regarding survival and limb salvage.
The follow-up protocol included medications in an advanced wound care setting (foot clinic managed by nurses with high expertise in wound care). Foot surgery was performed when necessary by a multidisciplinary team including a vascular surgeon, a diabetologist, and an orthopedist.
In all cases, dual antiplatelet therapy was administered continuously for at least 3 months after the procedure.
Outcome measures and statistical analysis
All data concerning the patients and their procedures were prospectively collected in a dedicated database. The information included demographics, preoperative risk factors, clinical and diagnostic preoperative assessments, procedural findings, and early (30-day) and follow-up outcomes.
Continuous data were expressed as the mean ± range. Categoric data were expressed as percentages. The nonparametric Pearson chi-square test was used when necessary to compare variables.
Five-year outcomes in terms of secondary patency, survival, and limb salvage rates were analyzed with Kaplan–Meier curves and compared between the three groups (CPA, IPA, and APA) by means of Gehan–Breslow–Wilcoxon test. Outcomes were given with the 95% confidence intervals (CI).
In the overall population, uni- and multivariate analyses of the preoperative factors affecting the survival and limb salvage rates were performed by means of log-rank test and Cox regression analysis. Results of the regression analyses were presented as the hazard ratio (HR) and 95% CI.
Statistical significance was defined at the p < 0.05 level.
Statistical analysis was performed using SPSS software (version 24.0 for Apple; IBM Corporation, Armonk, NY, USA).
Results
Demographic and morphological data
The 153 patients were predominantly male (98, 64.1%) with a mean age of 74.9 years (range 46–94).
Demographic and intraprocedural data.

Continuous data are presented as the means; categorical data are given as the counts (percentage).
Note: TUC, Texas University Classification.
aGlomerular Filtration Rate, GFR <30 mL/min.
bCritical stenosis means one or more stenosis more than 70% with peak systolic velocity (PSV) ratio >2.5.
Eighteen patients (11.7%) had the maximum level of WIfI classification (333).
A wound infection was diagnosed in 76 patients (49.7%). According to IDSA classification, infection was classified as mild in 16 cases (21%), moderate in 33 cases (43.4%), and severe in 27 cases (35.6%).
Perioperative outcomes
A BTK artery was the target vessel in 80 cases (52.3%). In most of the patients (96, 62.7%), two or more vessels were treated. No stent in BTK vessels was deployed. A successful foot artery revascularization was performed in 32 cases (20.9%), and a pedal-plantar loop technique was performed in 9 cases (5.9%).
Table 1 also summarizes the intraprocedural “endovascular” data.
Technical success according to “intention-to-treat” vessel (“in-line flow” to the foot) was achieved in 143 cases (93.5%).
Post-procedural angiography showed CPA in 44 patients (28.7%), IPA in 70 patients (45.8%), and APA in 39 patients (25.5%).
Demographic and intraprocedural data: comparison of the three groups.
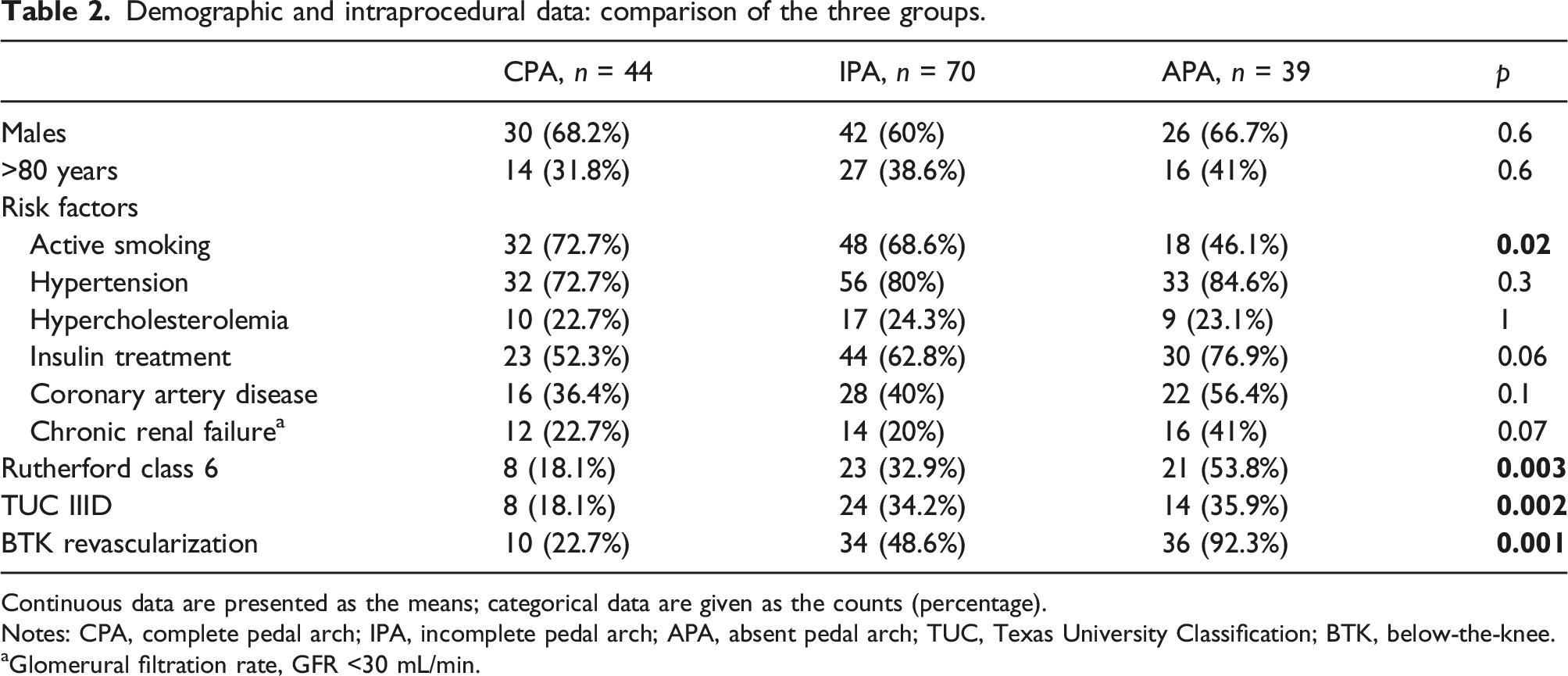
Continuous data are presented as the means; categorical data are given as the counts (percentage).
Notes: CPA, complete pedal arch; IPA, incomplete pedal arch; APA, absent pedal arch; TUC, Texas University Classification; BTK, below-the-knee.
aGlomerural filtration rate, GFR <30 mL/min.
Mean hospital stay was 4.1 days (range 2–9). All patients underwent strict wound management; wound treatment consisted of debridement without bone resection in 51 cases (33.3%), toe/ray amputation in 13 cases (8.5%), Lisfranc amputation in 1 case (0.7%), and transmetatarsal amputation in 6 cases (3.9%).
During the hospital stay, two patients had an acute limb ischemia due to superficial femoral artery thrombosis treated with open surgery in both cases (one thrombectomy and one femoro-distal vein bypass).
At 30 days, 2 patients died (acute heart failure and sepsis), and 2 patients underwent major amputation (sepsis in both cases).
5-year outcomes
Follow-up was available in all patients. Mean duration of follow-up was 31 months (range 1–72).
During the follow-up, 94 deaths and 15 major amputations occurred. All major amputations were performed within 2 years from the index procedure.
The overall 5-year rates of secondary patency, survival, and limb salvage were 41.1%, 28.2%, and 88.2%, respectively.
At 5 years, secondary patency was significantly better in CPA-group versus IPA/APA-groups (p < 0.001): CPA 72.7% (95% CI 68.5%–76.8%), IPA 33.2% (95% CI 30.3%–36.1%), and APA 24.8% (95% CI 19.9%–29.7%), respectively.
Five-year Kaplan–Meier rates of survival were similar in all groups (p = 0.1): CPA 30% (95% CI 22%–59.4%), IPA 27.5% (95% CI 8.4%–38.8%), and APA 26.4% (95% CI 0%–44.4%), respectively (Figure 2). Five-year survival and limb salvage (Kaplan–Meyer curves with number of patients at risk and standard error values for each group).
In addition, 5-year limb salvage was significantly better in patients with CPA/IPA (p < 0.001): CPA 95.1% (95% CI 80.7%–100%), IPA 94.3% (95% CI 92.9%–100%), and APA 67.3% (95% CI 63.8%–85.2%), respectively (Figure 2).
Univariate analysis for survival and limb salvage at 5 years.
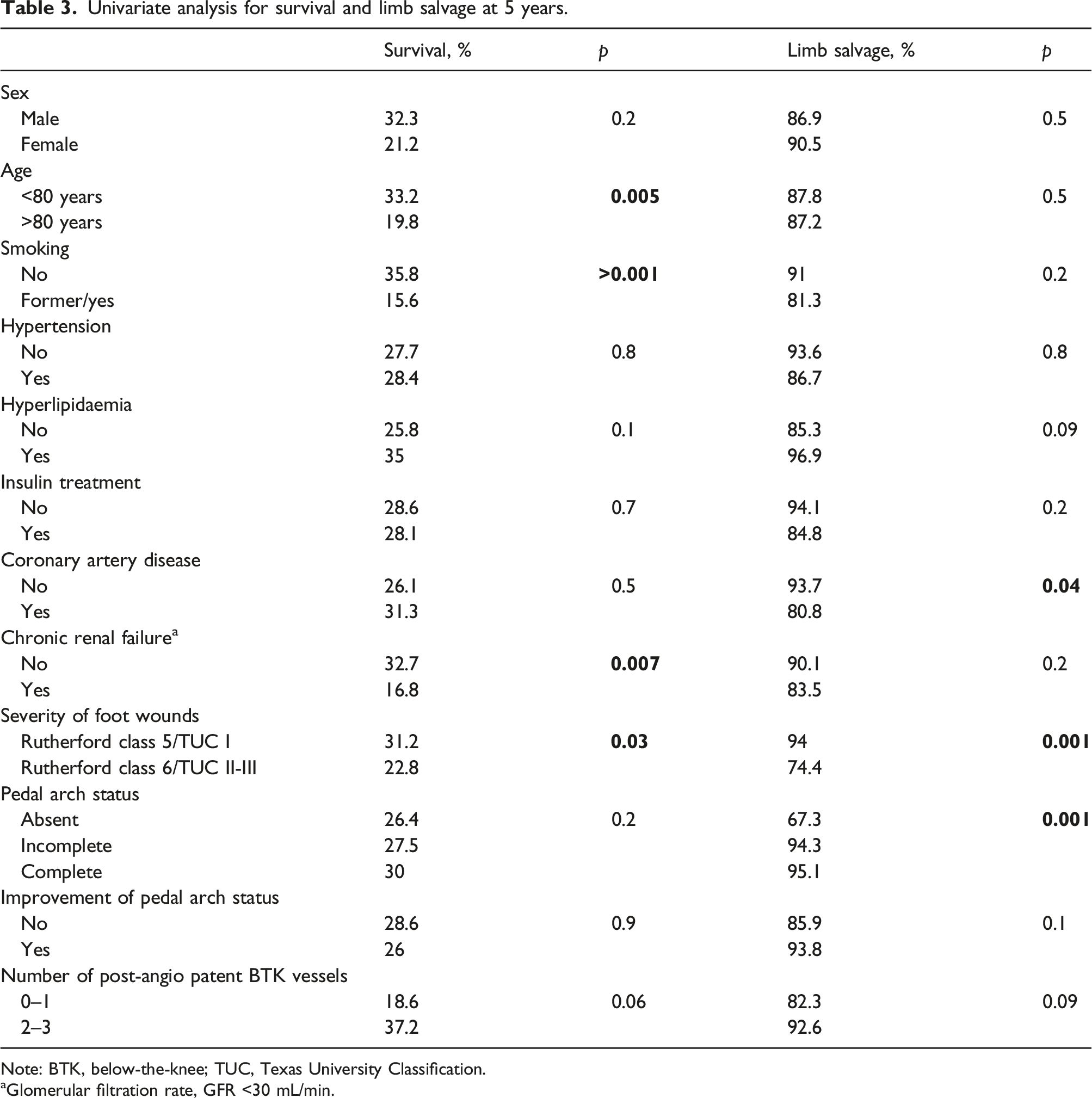
Note: BTK, below-the-knee; TUC, Texas University Classification.
aGlomerular filtration rate, GFR <30 mL/min.
Multivariate analysis confirmed the association of smoking (HR 6.7, 95% CI 4.1 to 9.3, p = 0.01), chronic renal failure (HR 5.8, 95% CI 3.7 to 7.9, p = 0.02), and severity of foot wounds (HR 12.6, 95% CI 8.6 to 16.6, p < 0.001) with 5-year survival rate. Furthermore, coronary artery disease (HR 4.8, 95% CI 1.4 to 8.2, p = 0.03), severity of foot wounds (HR 11.7, 95% CI 3.4 to 20, p = 0.001) and pedal arch status (HR 3.4, 95% CI 0.1 to 6.7, p = 0.05) confirmed their significant association with 5-year limb salvage rate.
Discussion
The presence of DFUs is strongly associated with an increased risk of death. The risk increases over the years. In 1990s, Boyko et al. 4 reported that the risk of death for diabetic patients with foot wounds is 12.1 per 100 person-years. 4 More recently, Walsh et al. 21 analyzed 20,737 foot ulcers in 414,523 diabetics enrolled in practices associated with The Health Improvement Network in the United Kingdom; they reported a 5-year mortality of 42.4% for patients with DFUs.
Other recent articles5-7 reported an overall 5-year mortality up to 35% in patients with DFUs. Some authors reported different rates of mortality according to ulcer type. 7 In the present study, we reported an overall 5-year mortality rate higher than those reported in literature (about 70%). This could be explained with a bias selection. Our population study was very elderly (mean age about 75 years) and affected by severe vascular complications of diabetes (all patients had an ischemic foot wound).
Regarding factors affecting 5-year mortality in patients with DFUs, Al-Rubeaan et al. 22 reported that presence of diabetic nephropathy was the only significant independent risk factor for all-cause mortality among patients with DFUs. Amadou et al. 7 demonstrated that age and severity of foot wounds increased the risk of death at 5 years. Moreover, Jeyaraman et al. 23 in Australia reported that age, chronic kidney disease, and low albumin levels increased the risk of death at 5 and 10 years in DFUs patients. In our series, insulin treatment (“more aggressive diabetes”) was not associated with worse 5-year survival rate.
In the present study, age more than 80 years, history of smoking, chronic renal failure, and severity of foot wounds are factors associated with 5-year survival. Multivariate analysis did not confirm the association of the age. In our study, smoking is an additional risk factor of lower survival rate in diabetic patients with foot wounds.
Concerning limb salvage, major amputation ranges from 5.6 to 600 per 100,000 in the population with diabetes. 9 In a recent meta-analysis, 24 the lower extremity amputation rate has been reported ranging from 6% to 78%. A wide variability in incidence exists. In the present study, the overall 5-year limb salvage is 88.2%, which is higher than previously reported.
Ischemia, hemodialysis treatment, and HbA1c level were considered independent risk factors for major amputation in diabetic patients with foot wounds. 25 Furthermore, age, male gender, chronic kidney disease, presence of peripheral vascular disease, and coronary artery disease were associated with poor outcomes in terms of amputation-free survival in diabetic patients.10–12,26 Revascularization is mandatory in diabetic patients with ischemic lesions.
In our population, study including only diabetic patients with ischemic wounds undergoing peripheral angiography the 5-year amputation-free survival rate was affected by history of coronary artery disease and severity of foot wounds. Insulin treatment did not affect 5-year limb salvage.
In addition, in our study pedal arch quality has been found as a predictor of poor limb salvage at 5 years. A successful foot artery revascularization was performed in about 20% of the cases; however, the upgrading of pedal arch quality did not improve the 5-year limb salvage rate.
Regarding secondary patency, 5-year data demonstrated an improvement of maintenance of “in-line flow” in patients with complete pedal arch. The presence of an adequate outflow may play an important role in maintaining the patency of the revascularized inflow vessels during the follow-up.
In literature, no morphological data have been reported as factors associated with limb loss in patients with DFUs.
Since the 1980s, the importance of a patent pedal arch in patients with critical limb ischemia has been well established. Several authors27,28 demonstrated the angiographic correlation of pedal arch patency with distal bypass patency. In addition, Davidson et al. 29 demonstrated that an aggressive surgical approach in patients with occluded BTK arteries and patent pedal arch was possible to maintain a functional extremity in the majority of the patients.
Beginning from 2000s, the evolution of endovascular techniques guaranteed a growing attention to the pedal arch patency in diabetic and non-diabetic patients with foot wounds.30,31 In the present study, a successful pedal-plantar loop technique was performed in about 6% of the cases.
More recently, the clinical importance of pedal arch patency over the angiosome revascularization has been reported. In open surgery, independent of angiosome revascularized, high percentages of wound healing have been reported in patients with complete/incomplete pedal arches. 32 Regarding endovascular surgery, pedal arch patency seems to be a key factor to obtain good outcomes in terms of wound healing and 1-year limb salvage rather than direct angiosome revascularization in diabetic patients undergoing peripheral revascularization. 33 Moreover, pedal arch quality has a positive impact on 1-year limb salvage in diabetic patients with foot wounds undergoing infrainguinal endovascular revascularization. 16
In the present study, the 5-year data analysis demonstrated that pedal arch status affected limb salvage but not survival rate.
The study has some limitations. First of all, it is a retrospective single-center analysis on a selected diabetic population with foot ischemic wounds who underwent peripheral angiography. This should be considered a bias of selection. Second, the study population is quite small; further analyses with a larger population study and longer follow-up are needed. Third, follow-up data about “in-line flow” to the foot are lacking and only secondary patency rates have been considered and related to the pedal arch status.
Conclusions
Pedal arch quality significantly affected limb salvage but not survival at 5 years in diabetic patients with foot wounds undergoing endovascular peripheral revascularization. In the whole population, some preoperative factors significantly affected the overall survival including smoking, chronic renal failure, and severity of wounds. In addition, coronary artery disease and severity of foot wounds demonstrated a strong association with 5-year limb salvage rate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.