
Abstract
Objectives
Chronic total occlusion (CTO) of the EVAR graft is a rare and serious complication. Traditionally, surgical intervention with prosthetic graft replacement or bypass graft implantation is performed. However, there are limited data in endovascular era.
Methods
We present a case of a 68-year-old male with a history of late EVAR graft occlusion treated with multiple surgical interventions (femorofemoral crossover, extra-anatomic bypass surgery, and thrombectomy) five years ago. Color Doppler ultrasound (CDUS) and computed tomography (CT) angiography revealed thrombosis of the entire bypass graft. Endovascular recanalization and remodeling of the abdominal stent graft CTO was performed with a combination of bare stents and stent grafts. Rupture of the stent graft occurred on the right limb. A second covered stent was placed.
Results
At 12-month follow-up, the patient was symptom free. Color Doppler ultrasound surveillance showed patent aortic stent graft and downstream arteries.
Conclusions
Endovascular recanalization of aortic stent graft CTO is a viable option in patients with failed bypass graft.
Keywords
Introduction
Endovascular repair of the abdominal aortic aneurysms (EVAR) has become the choice of treatment. 1 Compared to open surgery, EVAR has the advantage of being minimally invasive, with decreased risk of procedural morbidity—mortality and shorter hospital stay. 2
However, the reintervention rate after EVAR treatment is between 19%–24%. 3 Thrombosis of the graft limb or entire graft is a potential and serious complication. We report a case of successful endovascular recanalization and remodeling of chronic total occlusion (CTO) of the EVAR graft after five years subsequent to failed multiple surgical attempts.
Case report
A 68-year-old male was admitted with severe buttock claudication and increasing rest pain. He had a history of EVAR procedure ten years ago. Five years after the EVAR, femorofemoral crossover bypass was performed due to chronic total occlusion of the left limb of the stent graft. Two years after bypass surgery, the patient was admitted with recurrence of symptoms. Chronic total occlusion of the right limb of the stent graft was diagnosed, and the patient underwent extra-anatomic bypass surgery with insertion of a right-sided axillofemoral bypass. He also had a history of coronary bypass surgery, chronic obstructive pulmonary disease, and 30 pack years of smoking.
Physical examination and laboratory tests revealed no specific results. Color Doppler ultrasound (CDUS) examination showed total occlusion of the bypass grafts; common femoral artery and distal branches were patent. Computed tomography (CT) angiography confirmed CDUS findings (Figures 1 and 2). (a) Coronal MIP images of abdominal CT angiograhy reveals complete occlusion of the EVAR stent graft, iliac arteries, axillofemoral, and femorofemoral bypass graft. (b, c) DSA images confirm CT angiography findings. Strut dislodgement at the main body of the stent graft (arrow) and angulation at the right limb (arrowhead) can be seen (MIP = maximum intensity projection; CT = computed tomography; DSA = digital subtraction angiography). (a, b) Kissing stents with self-expandable stents and stent graft placement in the occluded EVAR graft limbs and iliac arteries. (c, d) Completion angiography revealed complete recanalization of the occluded segments while preserving renal flow. (e) Late phase of the angiogram shows contrast extravasation at the mid-third of the iliac artery (arrow). (f) Covered stent was placed, and final angiogram showed complete cessation of the leak at the location of strut dislodgment (arrowhead).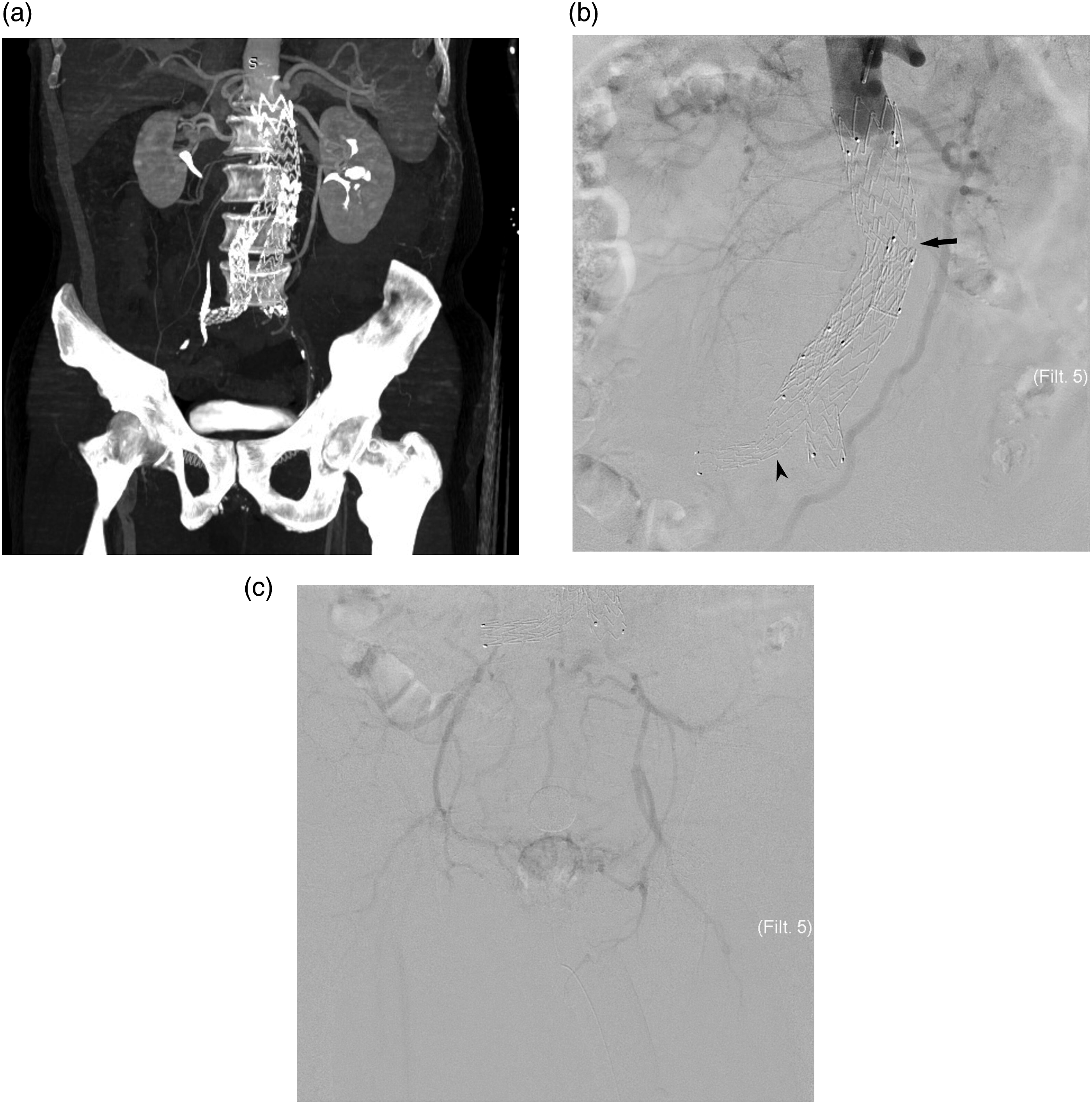

The patient was informed about his clinical situation and consent was obtained for endovascular intervention. The entire procedure was performed under sedoanalgesia. The left brachial artery was accessed under ultrasound (US) guidance, and bilateral femoral arteries were accessed by surgical cutdown. Initial bolus dose of intravenous 5000 IU unfractionated heparin was administered, and additional doses were injected to maintain an ACT level between 250–300 s.
A 5F pigtail catheter (Tempo, Cordis, Baar, Switzerland) was placed at the renal artery level, and angiograms were obtained. Retrograde catheterization of the right iliac arteries and right limb of the graft was attempted first but failed. The pigtail catheter was exchanged with a 90 cm–long guiding sheath (Destination, Terumo Medical Corporation, Tokyo, Japan). Antegrade catheterization of the occluded stent graft and iliac artery segments was achieved with a combination of a 0.035″ stiff hydrophilic guidewire (Radifocus, Terumo Medical Corporation, Tokyo, Japan) and 4F support catheter (NaviCross, Terumo Medical Corporation, Tokyo, Japan). Through-and-through technique was used to pass the guidewire from the femoral sheath. Subsequently, catheterization of the left iliac arteries and left limb of the stent graft was achieved in a retrograde fashion. Afterward, hydrophilic guidewires were exchanged for super stiff guidewires (Back-up Meier, Boston Scientific, Marlborough, USA) to attain better support.
Initially, two 14 x 50 mm self-expandable nitinol stents (EpicTM, Boston Scientific, Marlborough, USA) were deployed at the infrarenal level of the aorta, 1 cm superior to the occluded stent graft segment, in a kissing formation to secure the origins of the renal arteries. Subsequently, stent grafts (Endurant II endograft (Medtronic Inc, Minneapolis, Minn)) (16 x 124 mm in the left side and 16 x 199 mm in the right side) were placed in the occluded limbs, extending distal to the iliac arteries. A 12 x 60 mm balloon (Mustang, Boston Scientific, Marlborough, USA) was inflated to achieve adequate wall apposition. Completion angiograms showed complete recanalization of the occluded segments while preserving renal flow. Distal runoff was without any thromboembolic complication.
Hemostasis of the femoral access was achieved by surgical closure and brachial access by manual compression. The patient was kept under surveillance in the intensive care unit. At the sixth hour, tachycardia and hypotension occurred. US and CT examination revealed a large retroperitoneal hematoma (6 x 8 x 10 cm) at the right iliac artery level. Right common femoral artery was accessed under US guidance and a 5F introducer sheath was placed. Angiogram showed contrast extravasation at the mid-portion of the right limb of the stent graft. After three times of prolonged balloon inflation, contrast extravasation persisted. An 8 x 59 mm covered stent (Advanta V12, Atrium Europe B.V, Mijdrecht, The Netherlands) was placed. Completion angiogram showed cessation of the contrast leak.
Patient’s clinical status was stable during the hospital stay, and the patient was discharged on the fifth day of admission. Dual-antiplatelet therapy with aspirin (100 mg/d) and clopidogrel (75 mg/d) was prescribed.
Postoperative surveillance was scheduled at 1 week and 1, 3, 6, and 12 months. Physical examination, CDUS imaging, and blood tests including complete blood count and kidney function tests were planned. Claudication resolved significantly at the 1-week visit. The serum creatinine level was within normal limits. CDUS examination showed good flow in the stent graft and downstream arterial branches, and both renal arteries were patent.
Discussion
Most of the thrombotic events are encountered within two months after EVAR graft implantation. 4 Technical errors (malpositioning of the graft, extreme oversizing, and hemodynamically significant residual stenosis), type of graft, presence of thrombosis in the native aorta, smaller limb diameter, extensive angulation of the iliac arteries, and stent migration are possible causes of the obstruction. 5 In our case, late occlusion occurred in the postoperative fifth year. CT angiography and digital subtraction angiography images revealed strut dislodgement and angulation at the main body of the stent graft. Also, diameter mismatch between the limbs of the initial stent graft limbs and native iliac arteries, and steep angulation at the transition site was detected. Both iliac arteries were small and had a tortuous course, and showed chronic total occlusion. These findings might have contributed to occlusion of the stent graft.
Limb thrombosis is a relatively common complication with a reported incidence of up to 10.6%. 6 Results of percutaneous treatment have been reported to be comparable with surgery in the treatment of limb thrombosis.7–9 Spiliopoulos et al. reported a technical success of 90.9% in 11 graft limb occlusions with no major complications. Primary patency and symptom-free interval was 100% at 12 months and 83% at five years. 7 Van Zeggeren et al. treated 20 graft occlusions in 496 EVAR patients. Five (25%) of the interventions were performed percutaneously. Among the surgical group, in four patients, endovascular treatment with catheter-directed thrombolysis was attempted first but failed. Subsequently, open surgical treatment was performed. They found similar follow-up results between surgery and endovascular methods. 9
Complete graft thrombosis is rare. Traditionally, surgical treatment with excision of the graft and subsequent prosthetic graft placement or extra-anatomic bypass (axillofemoral with/without femorofemoral bypass) is performed. 10 Most of the patients undergoing EVAR have multiple comorbidities associated with high mortality and morbidity rates of surgical intervention. 11 Experience in the endovascular treatment of complete aortic graft occlusion is limited.11–13 Tatlı et al. reported a case of total graft occlusion which was treated with balloon angioplasty solely. Although intragraft thrombus load is high in EVAR patients, which carries a significant risk of distal embolus during percutanenous treatment, no sign of thromboembolism was encountered. 12 Debulking techniques might be useful to reduce thrombus burden. 14 In another case reported by Reis et al., a combination of lysis and balloon angioplasty was performed with successful results. However, the use of thrombolytic agents has the potential risk of endoleaks and retroperitoneal hemorrhage. 15 De Donato used covered stents in a kissing formation combined with bilateral renal chimneys to prevent bleeding while maintaining adequate flow. 11 CTO was the main concern in our case. Therefore, thrombolysis was not planned. The occlusion level was very close to the renal arteries. The patent segment of the infrarenal aorta was about 10 mm. The use of covered stents at this level might have inadvertently covered the renal artery origin. Additional methods like the chimney procedure would be required, which will increase the duration of the procedure and the cost. Self-expandable nitinol stents were preferred in the proximal part of the occlusion in order to not compromise renal flow while securing iliac remodeling with stent grafts. The proximal end of the stents was deployed at the infrarenal level. Hence, we did not use embolic protection devices. Unfortunately, following balloon dilation to achieve wall apposition, the stents migrated proximally a few centimeters above the renal artery level. Completion angiograms showed that both renal arteries were patent without any flow defect or embolic complication. Hence, renal artery stenting was not considered. Serum creatinine level showed no change during the hospital stay and follow-up period. Follow-up Color Doppler ultrasound examination was within normal limits.
In our case, a stent graft was placed through the right side initially. Multiple maneuvers were required to advance the stent graft through the preexisting EVAR stent graft limb. Though balloon angioplasty was performed with balloons with smaller diameters at low pressure to achieve wall apposition, contrast extravasation was encountered at the midportion of the stent graft. In retrospect, we observed that strut dislodgement was detected that might have contributed to a graft defect causing extravasation. The leak was then sealed with a second stent graft implantation.
Conclusion
In conclusion, CTO of EVAR graft is a severe and challenging complication. A meticulous treatment strategy should be tailored for each patient. Due to its minimally invasive nature, endovascular therapy might be a viable option in the treatment of CTO of stent grafts in patients with high risk for repeat surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declare that there is no funding for the research and/or publication.
Ethical approval
Ethic approval is waived in case reports by ethics review board
Informed consent
Informed consent was obtained from the participant. Consent for publication was obtained for individual person’s data included in the study.