
Abstract
Objective
Treatment of aortic arch pathologies in redo cases is technically challenging. In this study, we assessed early and mid-term outcomes of total endovascular arch repair combined with a new method of in situ laser fenestration.
Methods
Between January 2018 and March 2019, five patients with a history of cardiovascular surgery underwent in situ laser fenestration procedures using the “squid capture technique” for aortic arch pathologies with dissection. All patients were followed up regularly and imaging examinations were performed. The technical success, procedural complications, as well as the early and mid-term mortality and morbidity rates were evaluated.
Results
All patients survived the operation and fenestration was technically successful in all of the patients. There was no in-hospital mortality. No patients developed major complications, such as peri-operative strokes, transient ischemic attacks, or spinal cord ischemia. The 11–22 months follow-up (mean, 17 months) was completed by all patients. No endoleaks were discovered; false lumen thromboses and subsequent positive remodeling of the aorta were demonstrated and all in situ laser-fenestrated arteries were patent.
Conclusions
In situ laser fenestration combined with “squid capture technique” was shown to may be an effective and safe option for reconstruction of aortic arch during thoracic endovascular aortic repair. In situ laser fenestration combined with “squid capture technology” was shown to be an effective treatment option for patients with prior history of cardiovascular surgery and who are at high risk for redo open operations.
Introduction
Reoperations on the proximal thoracic aorta remain a challenge. The mortality is at least three times higher than that for the initial surgery. 1 The complications after such procedures occur with a high frequency, leading to substantial morbidity and delayed recovery.
Thoracic endovascular aortic repair (TEVAR) of aortic arch diseases remains one of the most difficult challenges in vascular surgery due to the variable configurations of the three major branches of the aortic arch (the innominate artery, left common carotid artery [LCA], and left subclavian artery [LSA]).2,3
Recently, five patients with a history of cardiovascular surgery (range, 1–10 months) underwent TEVAR with in situ laser fenestration for total endovascular aortic arch repair to maintain supra-aortic trunk patency.
Methods
Patients
The clinical information of five patients.

AVR: aortic valve replacement; TEVAR: thoracic endovascular aortic repair; LCA: left common carotid artery; LSA: left subclavian artery.
Anesthesia, incision and cerebral perfusion
With patients under general anesthesia, laser fenestration was performed on the aortic arch. For the patients with LSA involved only, the right femoral and left brachial arteries were prepped and cannulated with an 8F sheath (Terumo Medical Corporation, Somerset, NJ, USA). For patients with involvement of the LSA and LCA, the LCA, the left brachial artery, and the left or right femoral artery were exposed surgically under sterile conditions and cannulated with 8F/9F sheaths (Terumo Medical Corporation). Intravenous heparin (5000 U) and a 30 U/min drip infusion of heparin were administered.
For patients with the involvement of innominate artery, LSA, and LCA, bilateral carotid arteries and brachial arteries were exposed surgically under sterile conditions. Femoral vein-bilateral carotid bypass was established by femoral vein (20 F cannula; Edward Lifesciences LLC, Draper, USA) and bilateral carotid (16 F cannula; Kangxin Medical Instruments Co., Ltd., Changzhou, Jiangsu, China) cannulation (Figure 1). We cannulated the carotid about 1cm of proximal carotid bifurcation with ntravenous heparin (3 mg/kg) and a 10 mL/kg heparin perfusion flow. A cerebral perfusion was provided with a 15 mL/kg/min flow when blocking the branches of aortic arch. The target hemodynamics is around 70 mmHg monitored by invasive blood pressure. The establishment of the femoral vein-bilateral carotid bypass. (a) The bilateral carotid was exposed. (b) The right femoral vein was cannulated. (c) The right carotid artery was cannulated. (d) The bypass was ready before deploying the aortic graft.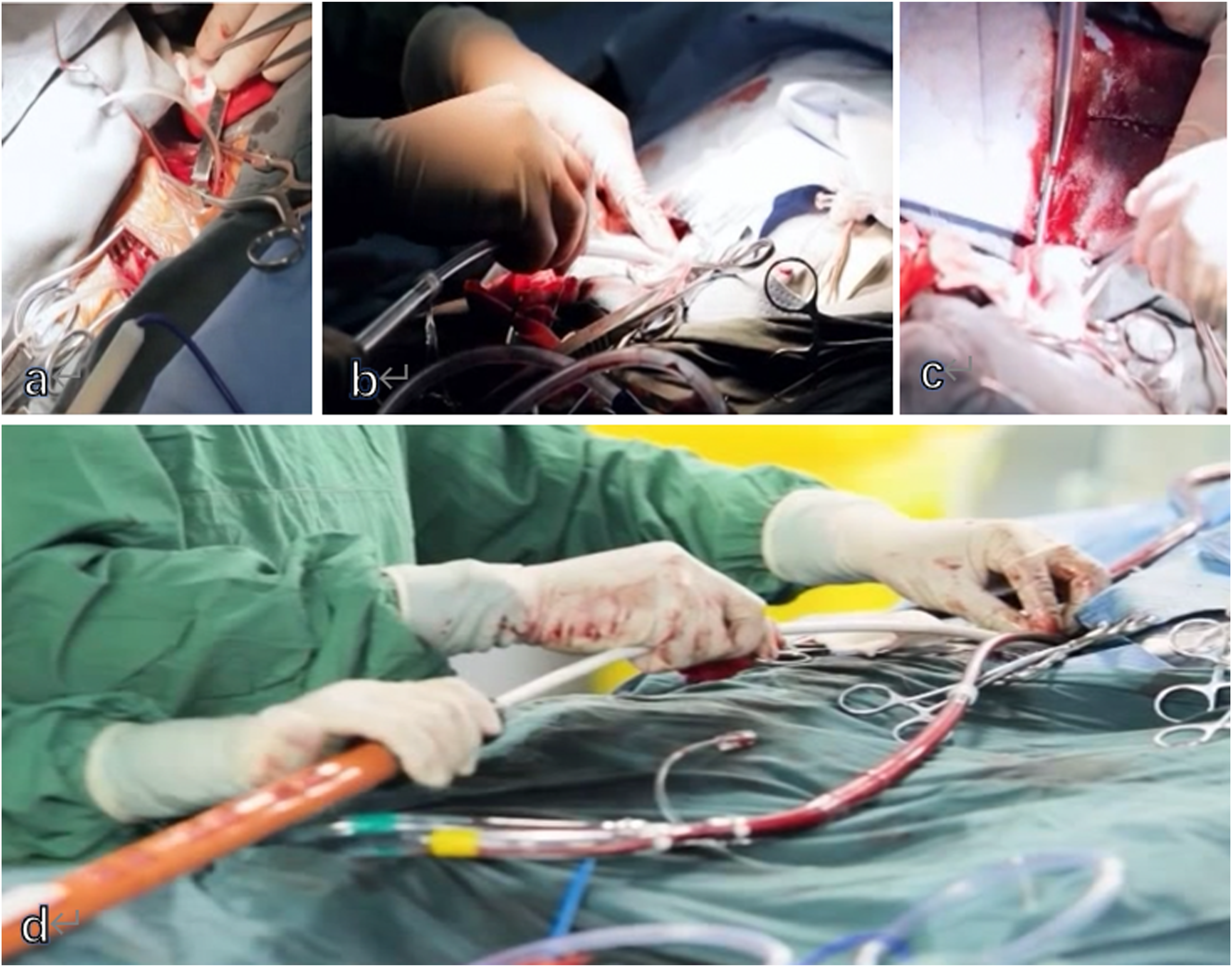
Stent implantation
A 150-cm 5F pigtail catheter (Cook Medical, Inc., Bloomington, IN, USA) over a 0.035-inch stiff guidewire (Terumo Medical Corporation) was advanced to the ascending aorta. The diameters of the ascending aorta and arch branches were measured using angiography and CTA. Thoracic endografts were deployed utilizing NBS (Terumo Medical Corporation) or TAG stent grafts (W. L. Gore & Associates, Flagstaff, AZ, USA).
Laser fenestration procedure
After the thoracic endograft was deployed, a 4 x 40-mm balloon catheter (Mustang; Boston Scientific, Boston, MA, USA) was used, followed by a 550-nm optical fiber (SlimLine EZ550; Lumenis Ltd, Yokneam, Israel) that was gently advanced in a retrograde fashion through the corresponding branch artery to be close to the thoracic endograft. Then, laser energy application was performed for 5 Hz with 0.8 J energy to create the fenestration. The laser energy was activated, and an in situ fenestration was created, thus directing flow to the artery. Either the whole laser fiber or the wire was passed through the newly created fenestration. A proximal fenestration was created and the balloon catheter was advanced into the true lumen over the fiber. After confirming reverse blood flow, balloon dilatation was performed to enlarge the fenestration. A 0.035-inch stiff guidewire was exchanged, and after endograft pre-dilation using a 8-mm balloon (Mustang), a covered stent (8–12 in diameter, 39-mm balloon stent; Abbott Laboratories, Clonmel, Country Tipperary, Ireland) was deployed through the fenestration into the endograft lumen and 10 mm into the branch vessel.
The squid capture technique
To make the fenestration easier, we used the “squid capture technique.”
4
At the beginning of the operation, we used a 260-cm loach guidewire (Terumo Medical Corporation) folded in half to enter the ascending aorta from the branch vessels, thus forming a loop in the arch (Figure 2(a)). The pigtail catheter came from femoral artery into the aorta and needed to enter the preset loop (Figure 2(b)), so the covered stents released in the aortic arch later were caught in the loop (Figure 2(c)). The loop wire was pulled to provide tension (Figure 2(d)) when fenestrating, and referred to as “squid capture technique.” Once we undo the “squid capture,” we send one end of the loach wire in and pull the other end out both as gently and slowly as possible, also we perform the DSA angiography to make sure of the result. The “squid capture technique” for in situ laser fenestration. (a) Three 260-cm loach guide wires folded in half to enter the ascending aorta from the branch vessels, thus forming a loop in the arch.(b) The pigtail catheter came from femoral artery into the aorta and enter the preset loops.(c) The covered stents released in the aortic arch later was caught in the loop. (d) The loop wire was pulled to provide tension when fenestrating.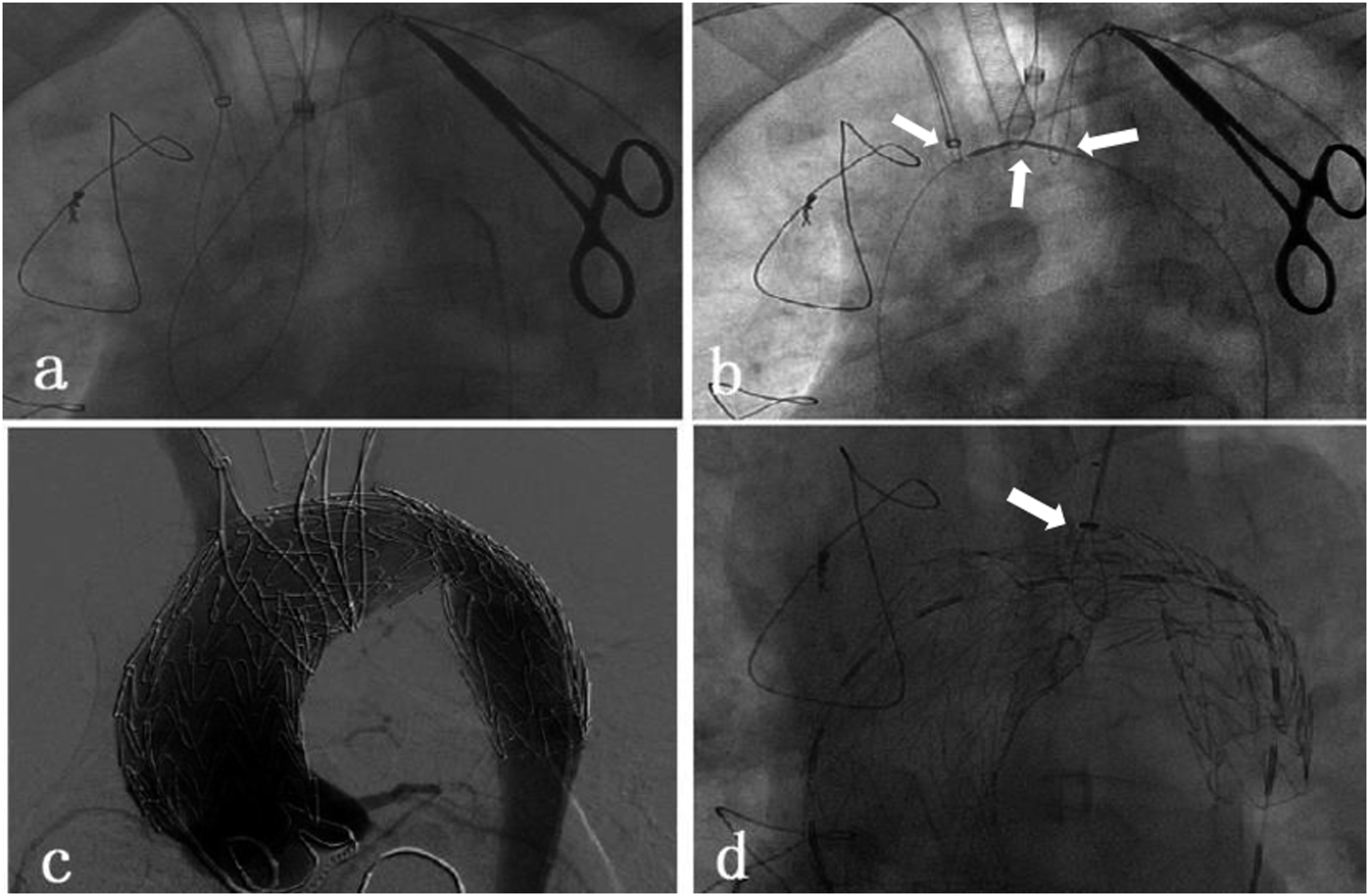
Follow-up outcome
Completion of DSA angiography was performed to demonstrate patency of the aortic stent and LSA or carotid fenestration. After the appropriate procedures, the incisions were closed. CTA was performed at 1, 3, 6, and 12 months post-surgery to evaluate fenestration patency, endoleaks, and aneurysm, as well as dissection exclusion.
Results
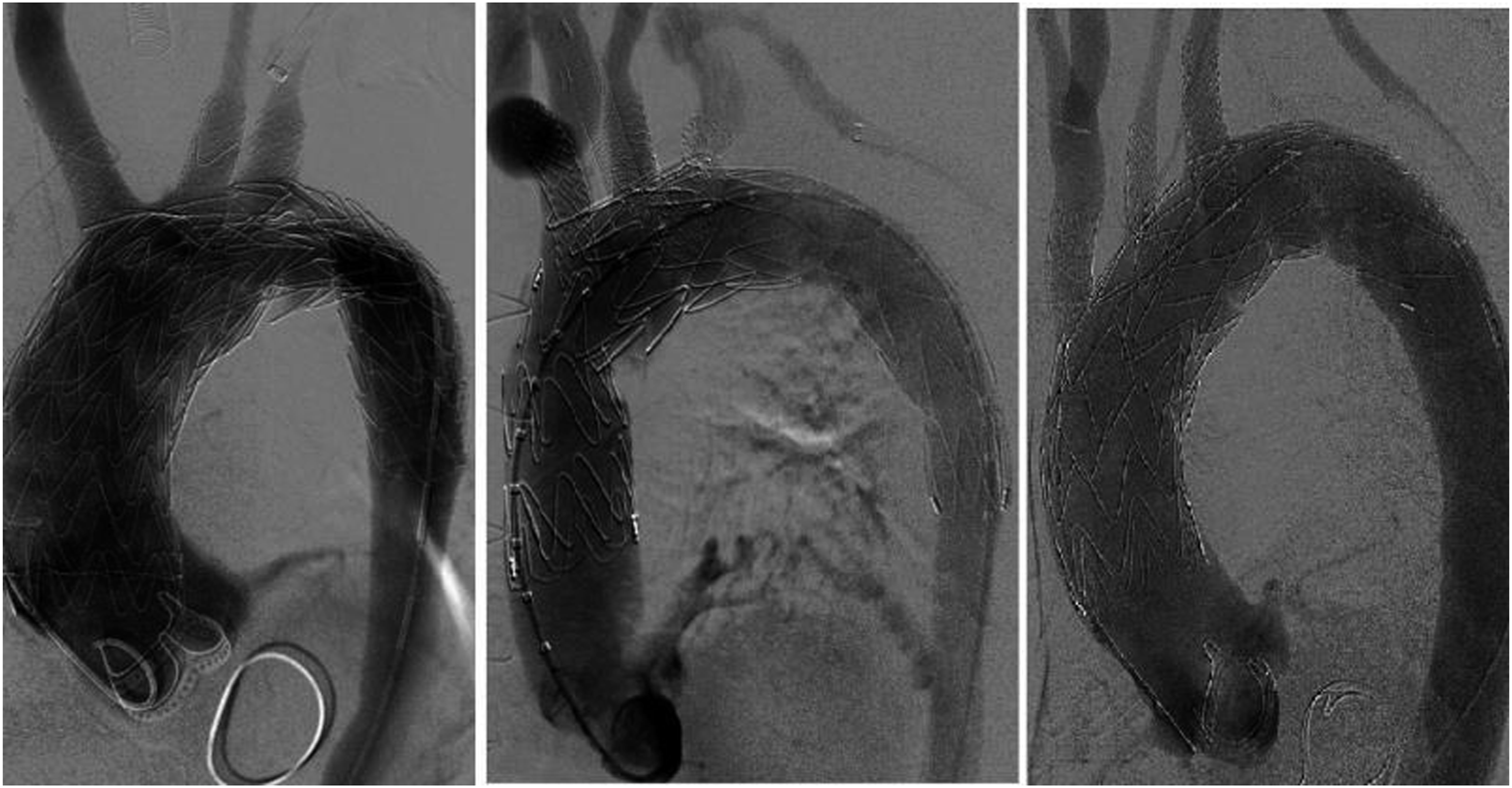
Thoracic endovascular aortic repair was technically successful in all five patients and the survival rate was 100%. An average of 3.4 endografts (range, 2–4) was implanted during TEVAR. Terumo NBS endografts were used in three patients, Gore TAG devices were placed in two patients, and one patient who had a type І endoleak after TEVAR underwent zone 2 deployment with in situ LSA fenestration (Figure 3). A zone 1 TEVAR placement was used in one patient who had an arch dissection after ascending aorta and innominate artery replacement and underwent in situ laser fenestration of the LSA and LCA (Figure 4). Three patients had a type A aortic dissection and underwent TEVAR with zone 0 deployment and in situ laser fenestration of the LSA, LCA, and innominate artery (Figure 5). A patient who had a type І endoleak after TEVAR underwent zone 2 deployment with in situ LSA fenestration.(a) After the first time of TEVAR, computed tomographic angiography (CTA) scan presented the endleak. (b) and (c) CTA scan was performed after redo TEVAR combine with in situ LSA fenestration demonstrated no endoleak. TEVAR: thoracic endovascular aortic repair; LSA: left subclavian artery; CTA: computed tomographic angiography. A zone I TEVAR placement was used in a patient who had an arch dissection after ascending aorta and innominate artery replacement and underwent in situ laser fenestration of the LSA and LCA. (a) Aortography was performed to measure the diameters of the ascending aorta and arch vessels; (b) Aortography was performed after stent implantation and in situ laser fenestration demonstrated no endoleak and dissection. TEVAR: thoracic endovascular aortic repair; LCA: left common carotid artery. Three patients had a type A aortic dissection and underwent TEVAR with zone 0 deployment and in situ laser fenestration of the LSA, LCA, and innominate artery. Aortography was performed after stent implantation. TEVAR: thoracic endovascular aortic repair; LCA: left common carotid artery; LSA: left subclavian artery.

The LSA fenestration bare stents ranged from 10 to 12 mm in diameter. The LCA and innominate artery covered or bare stents ranged from 8 to 10 mm in diameter. The operative time for TEVAR with in situ laser fenestration was 268 ± 138 min, the mean contrast volume was 200 ± 51 mL, and the mean bleeding volume was 230 ± 164 mL; none of the patients required a transfusion. An average of 40 min of the total case time was required to achieve innominate artery, LCA, and brachial artery or SCA access (Table 1).
No patients developed major complications, such as peri-operative strokes, transient ischemic attacks, or spinal cord ischemia. All patients recovered uneventfully and were discharged to home; there was no in-hospital mortality. The hospital stay after TEVAR was 8.4 ± 4.5 days (range, 4–15 days) and the length of ICU stay was 2 ± 1.4 days. The follow-up time was 11–22 months (mean, 17 months). No endoleaks were demonstrated. False lumen thrombosis and subsequent positive remodeling of the aorta were confirmed. All of the in situ laser-fenestrated arteries were patent based on post-operative follow-up CTA imaging (Figure 6) and clinical findings. CTA presented appropriate access sites of fenestration, stent placement, patency of the aortic arch branches. CTA: computed tomographic angiography.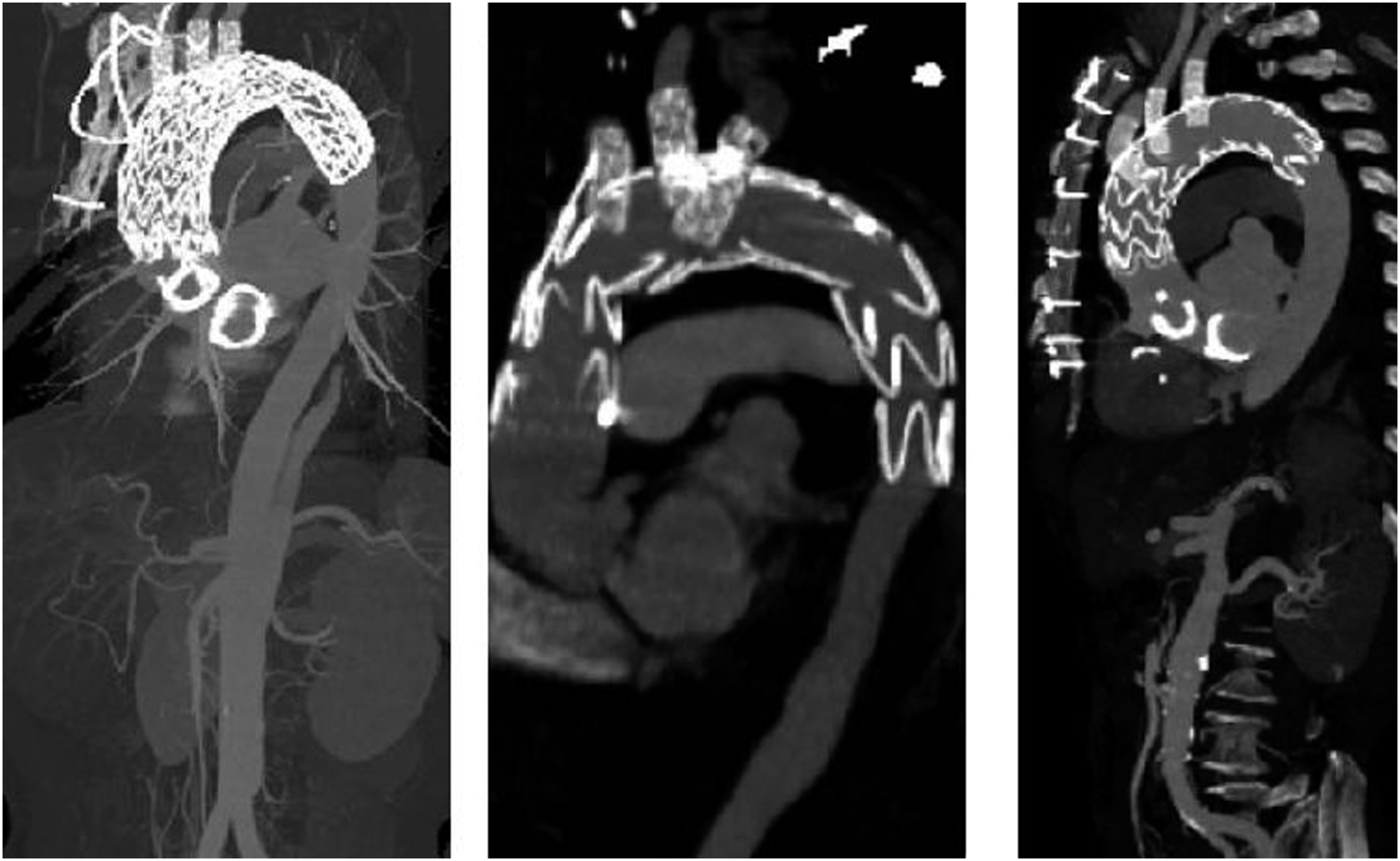
Discussion
Type A aortic dissection has a finding associated with high morbidity and mortality.5,6 Type A aortic dissection can occur during or after cardiac procedures at sites of mechanical trauma owing to pre-existing aortic wall pathology. Treatment for patients with a previous cardiac procedure carries a higher risk. 7 Classic teaching has been that patients of type A aortic dissection with aortic arch involved and with entry in the proximal thoracic aorta may undergo the total arch replacement combined with stented elephant trunk implantation as a total surgical arch repair procedure 6 ; however, even in centers of excellence, this procedure is associated with increased chances of mortality and major cerebrovascular disorders. Owing to advancements in catheter-based techniques, endovascular management has evolved to be a useful tool for select patients with type A aortic dissection. 8
Among patients with post-operative iatrogenic type A aortic dissection, the intimal tear is usually located in an area of surgical manipulation (e.g., aortic clamping or cannulation), 7 which provides an opportunity for intervention because the stent must be positioned above the coronary artery. In our cohort, three patients with type A dissections after cardiac operations had intimal tears located in the ascending aorta > 3 cm above the coronary artery, which provided a strong and sufficient landing zone for stenting.
A branched and fenestrated endograft seems to be the most promising approach for total endovascular arch repair; however, waiting for custom made devices is time-consuming, thus hindering the applicability. In situ fenestration is another potential technique for arch vessel revascularization. Different fenestration techniques have been reported, including radiofrequency probes, 9 the use of needles or sharp guidewires, 10 in situ retrograde fenestration, 11 and laser. 12 All of the techniques have known advantages and disadvantages. A needle or radiofrequency probe is effective if the distance from the access site to the fenestration site is straight and short, such as a surgically exposed LCA; however, this application is limited for LSA, which often exhibits an acute angle between the origin and the aortic arch. A laser provides a rapid and repeatable method of in situ fenestration of the endograft membrane and penetrates 0.3 mm into tissues, which expands the TEVAR application as a stable and safe procedure. In addition, the laser fiber is soft and can pass through various types of complex aortic arch anatomic findings. 13 Our data showed that in situ laser fenestrations did not lead to peri-operative strokes, myocardial infarction, transient ischemic attacks, cerebral infarction, or other neurologic complications and no endoleaks were observed. Therefore, we assume that this method is sufficiently safe, unlike the chimney graft, which can cause gutter endoleaks.
There were two difficulties with the fenestration: 1. How to avoid damaging the branch vessels when the laser power is activated? 2. The balloon catheter is difficult to enter the new hole because the catheter is thicker than the laser fiber. To solve these problems, we adopted a new method referred to as “squid capture technique.” We pulled the loop wire to provide tension when performing the fenestration to assure that the fiber fired only on the membrane and avoid the laser fiber from slipping forward proximally from the graft to the aorta, regardless of the arch anatomy, which differs from the report that patient selection is paramount for in situ fenestration. 13 Also, the tension makes it easier when the balloon catheter enters the new opening. This is the first report using this method of fenestration.
We applied some bare stents in these cases as bridging stents. All the patients had their lesions on the lesser curvature side of the aortic arch, so we assumed the bare stents may be safe in these cases. Bare stents have a better passing ability versus covered stents, making it easier to be deployed through the fenestration, therefore to shorten the operation time. Moreover, it reduced the operation expenses. Once the endoleak occurs, we can also remedy it by deploying an additional covered stent within the previous bare stent. Fortunately, we have not observed the endoleak in these locations in the follow-up. So, we infer that it is simple and safe to choose bare stent in specific cases; still, it remains to be proved.
For cerebral artery ischemia involving innominate artery and LCA reconstruction, we use femoral vein-bilateral carotid bypass with a flow of 10 mL/kg/min to assure cerebral perfusion.
There are no publications comparing open and total endovascular techniques of the aortic arch in redo cases. Although the results of open surgical treatment are superior, mortality may still reach 41.7%. 7 In our group, no cases died in-hospital. Moreover, analysis of mid-term outcomes revealed no aortic disease- and intervention-related deaths and adverse events during the follow-up period. The small size of our group was definitely a limitation.
In situ laser fenestration offers many potential benefits over surgical operation in redo cases, and no major complications were observed. In summary, in situ laser fenestration represents a breakthrough in treating redo aortic pathologies and “squid capture technique” provides an easier and safer method for fenestration.
Conclusion
This study demonstrates that in situ laser fenestration combined with the “squid capture technique” is an effective and safe technique for reconstruction of the aortic arch during thoracic endovascular aortic repair, which might be available to revascularize the three branches of the arch. The high technical success and good early outcomes expand this application to more patients with a stable and safe procedure. Our experience demonstrates that in situ laser fenestration may be a considerable method in the treatment of patients, especially patients with a history of cardiovascular surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by national natural sciense foundation of China (Grant No.81601709) and Scientific Research Foundation of the National Health Commission of China (WKJ-ZJ-2121).