
Abstract
Objective
The number of office-based procedure centers with the capability of performing a wide range of endovascular procedures has substantially increased over the past decade. This shift in practice settings has occurred faster in the private sector as compared to the academic environment. The purpose of our study was to evaluate the clinical outcomes of endovascular procedures performed at a dedicated academic outpatient procedural center.
Methods
We reviewed the clinical data of 400 patients who underwent 499 endovascular procedures in a university-based, academic outpatient procedure center between November 2013 and December 2016. Outcomes analyzed included procedure-related complications, limb loss, mortality, and emergency department visits or hospital admissions that occurred within 30 days following the procedure.
Results
The 400 patients had a mean age of 65 ± 13 years with slightly more females (51%; n = 203) as compared to males (49%; n = 197). Most patients (71%; 284) were Caucasian while 80 (20%) were African-Americans. Associated comorbidities included hypertension (86%), diabetes mellitus (51%), chronic kidney disease (42%), and obesity (mean body mass index of 29 ± 6). Based on anesthetic risk, most were ASA class 3 (81%), while ASA 1 and 2 comprised 17% and ASA 4 only 2%. Medicare beneficiaries accounted for 254 (64%) of our patients. Pre-operative studies included mainly duplex ultrasound (62%) and other noninvasive arterial studies (57%).
The mean procedural time was 58 min (range, 7 to 200) with an overall technical success rate of 97%. There were no deaths. Complications developed in 10 patients following the 483 procedures (2.1%) being hospitalized with four of them transferred directly to the emergency room. The reasons for these hospitalizations included acute limb ischemia, arterial pseudoaneurysm, deep vein thrombosis, congestive heart failure, myocardial infarction, and lower extremity pain not vascular in origin. Financial reimbursement at the office-based center was higher than that seen with hospital-based procedures.
Conclusions
Endovascular procedures performed in an academic office-based procedure center are safe and associated with good clinical outcomes. A small minority of patients have subsequent ER visits or hospital admissions. Academic institutions should consider adding an office-based procedure center based on today’s competitive healthcare market.
Introduction
Office-based endovascular procedures have become an increasingly popular alternative to hospital-based procedures. 1 The initial outpatient endovascular experience was started more than 50 years ago by Dotter and colleagues. 2 In the beginning of the outpatient vascular experience, academic centers were a common place where these procedures were done. However, most were hospital-based outpatient settings. More recently, there has been a major shift with more procedures being done in an office-based environment due to technological advances and a favorable shift in reimbursement favoring outpatient and office practices. This shift in treatment location has been spearheaded by the private sector with academic practices being less involved.
Current advantages of outpatient non-hospital procedure centers include better reimbursement rates, more flexible case scheduling, and higher patient satisfaction compared to a hospital setting.1,3 Endovascular procedures performed in an outpatient setting include primarily venous, arterial, and dialysis access work.4,5 The complexity of an outpatient facility varies from an office-based facility without any anesthesia personnel involvement to fully equipped surgical centers with full anesthesia support and mechanical ventilation.
The safety of procedures performed in outpatient facilities by vascular surgeons have been reported in a few prior studies.4,5 The vast majority of these centers are high volume, privately owned facilities, often run without the involvement of vascular surgery trainees and not under university control.4–7 An academic outpatient office-based procedure center inherently will differ significantly from a private one in terms of management, bureaucracy, and trainee participation. The goal of our study was to evaluate the clinical outcomes and some financial aspects of endovascular procedures performed in an academic office-based procedure center.
Methods
Procedure center specifics
A surgery procedure center (SPC) was inaugurated in November 2013 as an extension of the office practice of the full-time academic physicians in a university-based department of surgery. Although physically separated from the surgical practice offices, it was located on the academic campus of the college of medicine and staffed by the regular administrative and nursing personnel of the surgery department. Conscious intravenous moderate sedation for most vascular procedures was provided by either a registered nurse certified for such procedures or contracted certified nurse anesthetists. Physician oversight was provided by the operating vascular surgeon. Medical students, general surgical residents, and vascular fellows participated in these procedures after the initial 3 months’ startup when procedures were standardized. Patient demographic data was prospectively entered and maintained in the electronic medical records. A registered nurse contacted all patients on the phone one to 3 days after each procedure to confirm that there were no complications. A quarterly quality analysis review was performed with participating physicians and patient complications discussed. A memorandum of understanding was established with a nearby hospital, at which the surgeons had admitting privileges for any emergency transfers that may be needed directly from the center. Although general surgeons also performed upper and lower endoscopy procedures at the center, this review encompasses only the vascular procedures that were performed.
Patients’ selection
Patients chosen for percutaneous endovascular interventions to be performed at the procedure center instead of the hospital were selected by the vascular surgeon based on the clinical evaluation that the patient, both anatomically and physiologically, could undergo the scheduled intervention with moderate sedation. The American Society of Anesthesiology (ASA) class was determined during the patient’s pre-intervention office visit with the general expectation that patients with ASA class 4 and 5 were not candidates for outpatient treatment at center. This classification was re-evaluated by the nurse anesthetist the day of the procedure.
Patients on anticoagulants were generally instructed to discontinue its use prior to the procedures. Those who were deemed to be high-risk for thrombotic events while off anticoagulation (5 days for warfarin and 2 days for newer anticoagulants, such as anti-factor X and direct thrombin inhibitors) were not scheduled at the center. Patients weighing more than 250 kilograms were also not candidates due to potential airway management risks under moderate sedation and operating table limitations.
Procedures and equipment
The endovascular procedures performed included percutaneous arterial diagnostic and therapeutic interventions with balloon angioplasty, stenting, and laser atherectomy; venography and inferior vena cava filter placement and removal, great and small saphenous vein ablation, stab phlebectomies, and sclerotherapy; hemodialysis access maintenance (fistulogram, fistuloplasty with and without stenting; catheter insertion and removal); and subcutaneous central venous port placement and removal.
The endovascular suite was equipped with a C-arm (Siemens; Malvern, PA) and a portable vascular ultrasound unit (ASUS; Taipei, Taiwan). A laser generator (Spectranetics; Colorado Springs, CO) was in place at the center. A radiofrequency ablation generator (Medtronic; Minneapolis, MN) was used for superficial endovenous thermal ablation procedures. Sterile surgical instrument sets were available for open cut-downs, thrombectomy, or vascular repair should they be needed on an emergent basis. This study was approved by our University Institutional Review Board (IRB) ethics committee.
Study protocol
This study reviewed the patients’ demographic characteristics, medical comorbidities, ASA class, imaging and noninvasive pre-operative evaluation, procedural data, and 30-day morbidity and mortality, including emergency room transfers/visits and hospital admissions. Technical success was defined as successful arterial and arteriovenous access interventions if there was < 30% residual stenosis and no flow-limiting dissection or occlusion, obliteration of the saphenous vein after thermal ablation, functional hemodialysis, and use of central venous port after placement. Patients reviewed were those that had at least one follow-up office or hospital visit within 30 days besides the follow-up phone call performed within 24–72 h following the procedure
Statistical analysis
Continuous variables are reported as mean and standard deviation while categorical variables are reported as frequency and percentages. A p-value less than 0.05 was considered statistically significant. Statistical analyses were performed utilizing JMP software (SAS Institute; Cary, NC).
Results
Patient characteristics
Clinical characteristics of patients.
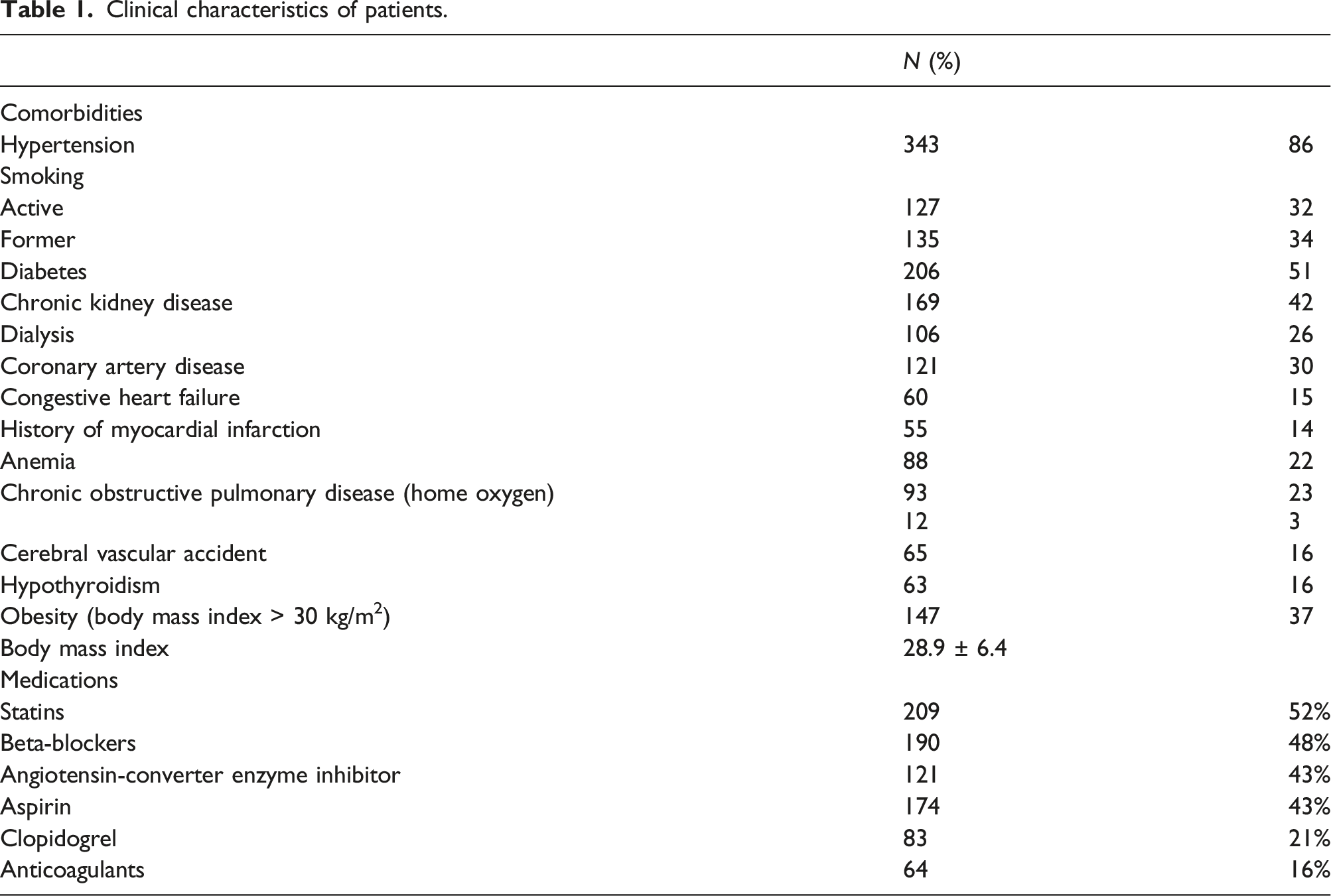
In terms of anesthetic risk, most of the patients were ASA class 3 (324; 81%). Patients classified as ASA classes 1 and 2 comprised 17% (N = 67). More than half of ASA 1 and 2 class patients underwent endovenous procedures (N = 42, 63%). There were 9 of the 400 (2%) patients considered ASA 4 by the CRNA on the day of the procedure, which were discussed with the surgeon performing the procedure and it was determined that the procedures could be safely carried out. Out of these nine ASA class 4 patients, seven underwent peripheral arterial procedures and two underwent an arteriovenous fistula intervention.
Procedures
Prior to the 499 endovascular procedures, most of the patients had prior noninvasive diagnostic physiologic and imaging studies performed (Figure 1). Arterial or venous duplex ultrasound was done before 249 (50%) procedures, anklebrachial index with segmental pulse volume recording was performed on 197 (39%) patients, while a small number of patients with aortoiliac or multilevel arterial disease had undergone computed tomography angiography (N = 61, 12%). Transcutaneous oxygen pressure test was performed in 6% of patients with critical limb ischemia and tissue loss for evaluation of possible healing or amputation site selection. Physiologic and diagnostic testing performed before procedures done at the procedure center.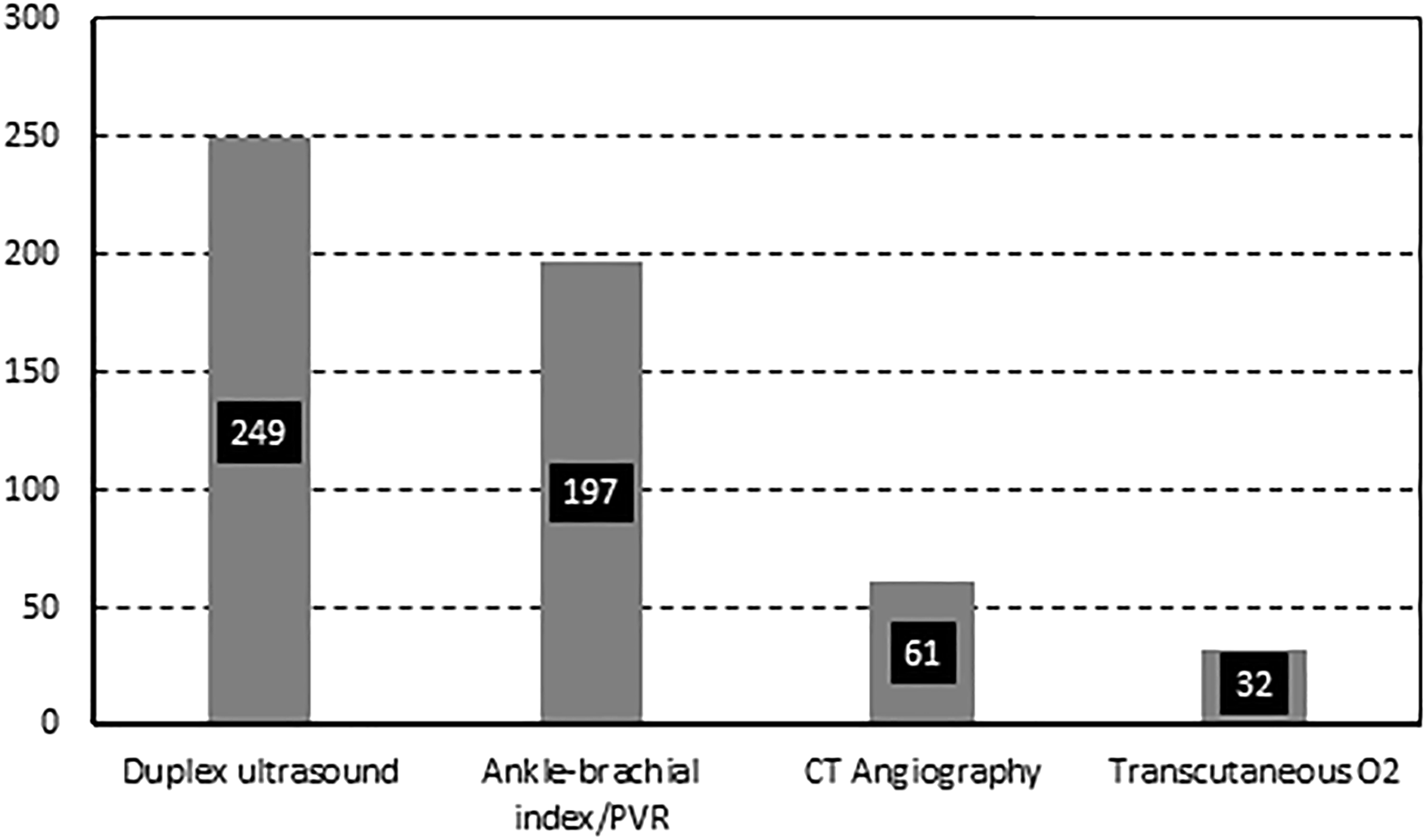
The most commonly performed procedure was arteriography with and without intervention accounting for more than half of the case volume (N = 267, 53%) (Figure 2). Of the lower extremity diagnostic arteriography performed (n = 127), it was most commonly done in patients with tissue loss (N = 50, 39%) and by pain at rest (N = 50, 39%). A considerably lower number of patients underwent angiography for lifestyle-limiting claudication (N = 27, 21%). Patients undergoing lower extremity intervention (n = 136) did so for tissue loss (63, 46%), rest pain (34, 25%) and limiting claudication (39, 29%). The remaining 211 (42%) of patients underwent endovenous interventions, hemodialysis catheters or central infusion ports, or IVC filter procedures (Figure 2). Distribution and types of procedures performed at the center during the 3-year period.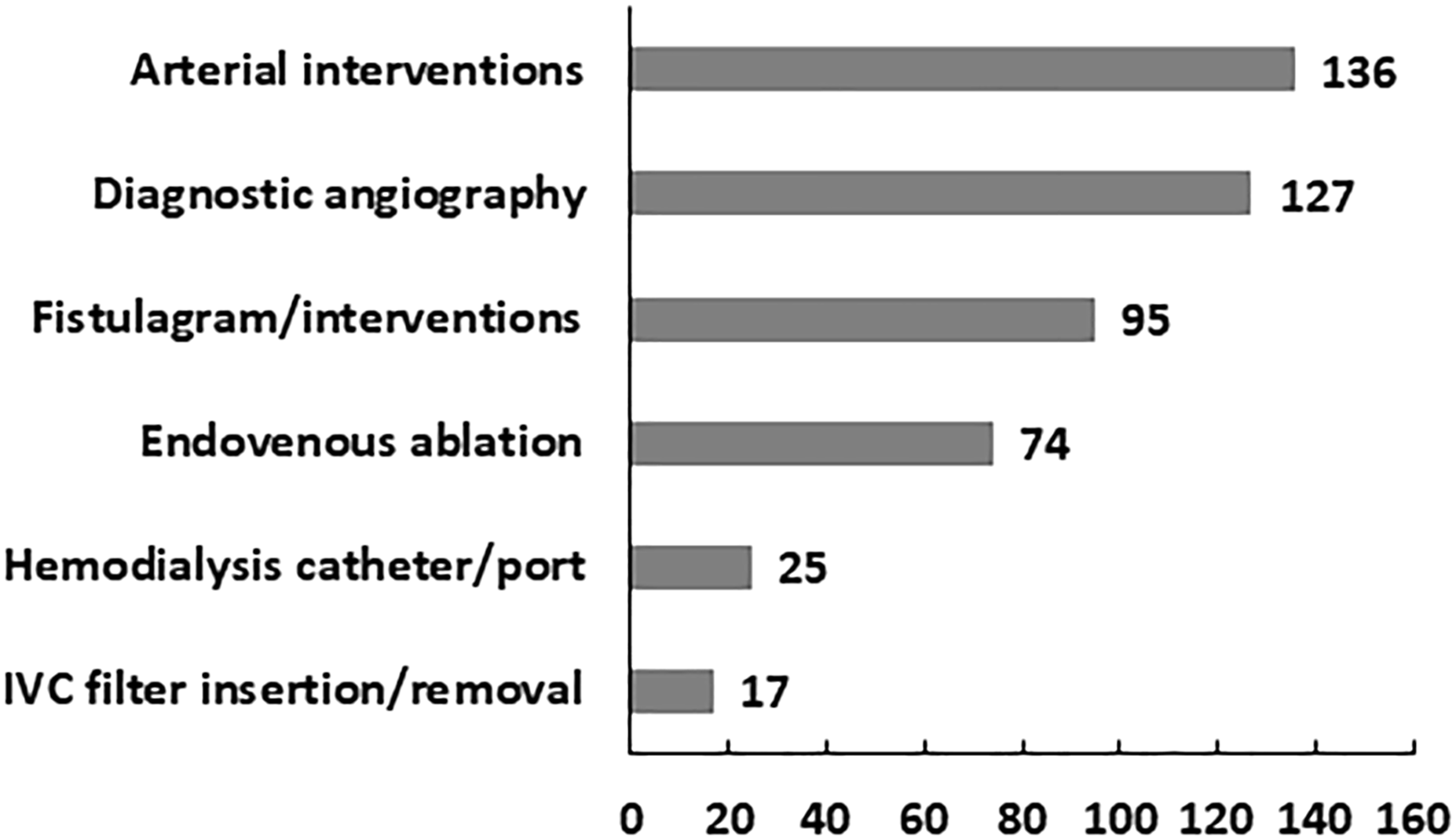
Procedures performed.
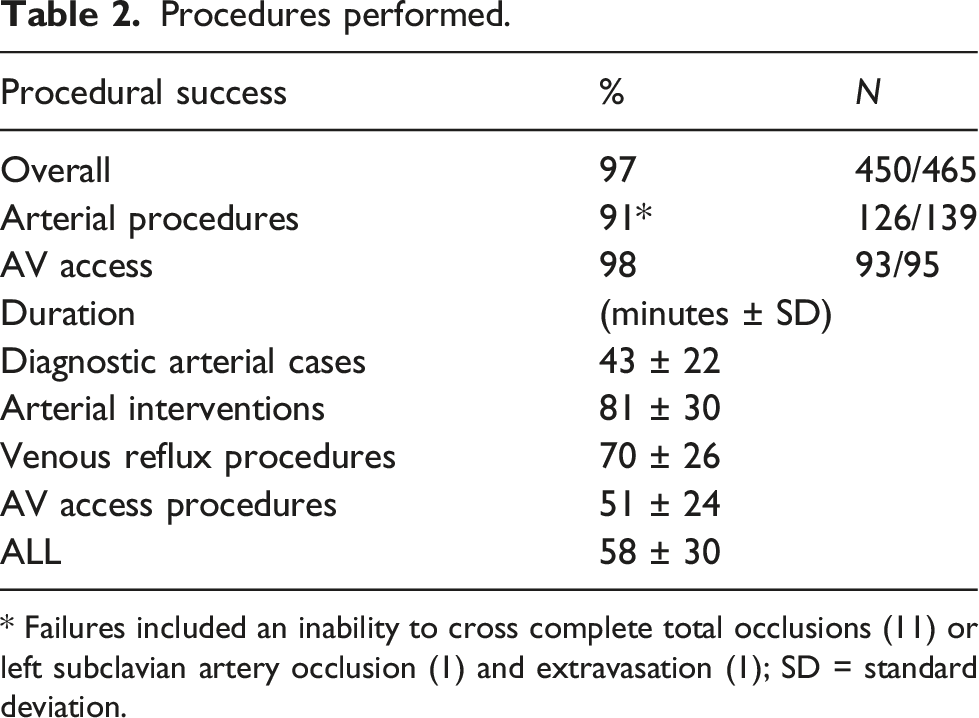
* Failures included an inability to cross complete total occlusions (11) or left subclavian artery occlusion (1) and extravasation (1); SD = standard deviation.
Clinical outcomes
A total of ten patients following the 499 procedures (2%) were admitted to the hospital within 30 days after their procedures. Eight of them were transferred from the center emergently to the hospital emergency room. The causes for their transfer and admission were: decompensated congestive heart failure (CHF), femoral artery pseudoaneurysm (2), acute limb ischemia, symptomatic bradycardia, arteriovenous access thrombosis, acute coronary syndrome, and right internal jugular thrombosis following hemodialysis catheter placement.
The patient with acute limb ischemia was operated upon emergently with thrombectomy and patch angioplasty after inadvertent intra-arterial deployment of a bioabsorbable plug from a vascular closure device. A successful thrombin injection was performed for the first patient with groin arterial pseudoaneurysm at the femoral access site. A second patient with femoral artery pseudoaneurysm secondary to misdeployment of vascular closure device was taken emergently to the operating room for femoral artery repair. The patient who had an episode of bradycardia, which was deemed to be related to sedation, was discharged after overnight observation. The patient with an acutely thrombosed AVF underwent successful thrombectomy. Anticoagulation was initiated for the hemodialysis catheter-related jugular thrombus with good clinical improvement. Lastly, the patient with decompensated CHF was treated medically with resolution of his acute clinical presentation, and the patient with ACS underwent placement of five coronary artery stents.
Two other patients were admitted to the hospital within thirty days of their procedure on post-intervention days 3 and 5. These two patients admitted for lower extremity pain following a diagnostic lower extremity angiogram were not found to have either arterial or venous pathology; the pain resolved prior to hospital dismissal. All patients were discharged within 48 h except for the patients with decompensated CHF, ACS, and one of the patients who underwent femoral artery repair which required a 3-day hospital stay. There were no deaths within 30 days from any of the procedures.
Financial aspects
Payor mix.
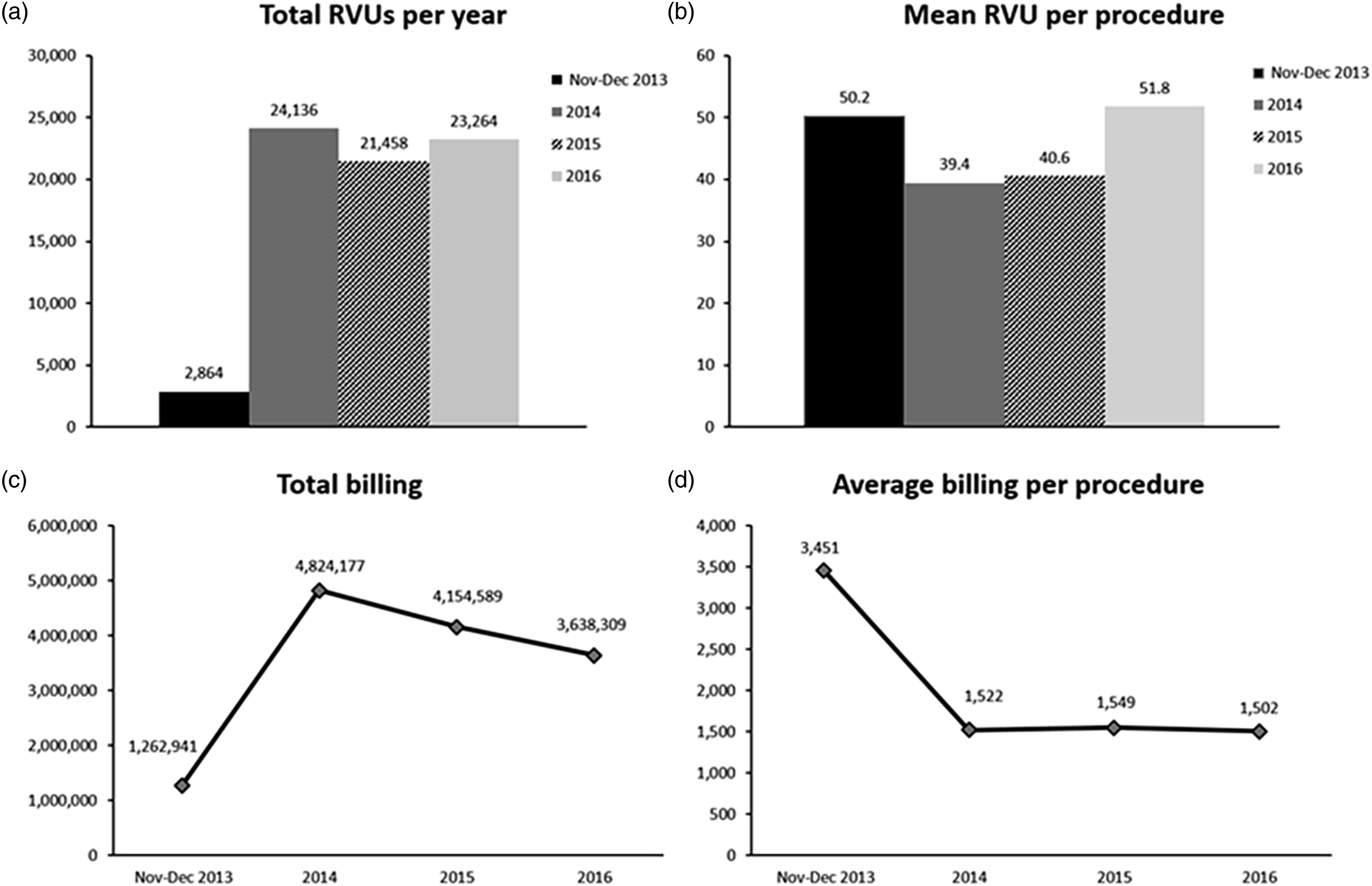
Financial activity during the study period demonstrating total relative value units (RVU) and associated billings from the vascular procedures performed.
There is a major difference between physician billings for procedures performed at the hospital as compared to the outpatient setting. Figure 4 depicts this and the associated wRVU for atherectomy cases performed at our hospital and at the office-based center (p < 0.001). Relative billing rates obtained for representative procedures at the procedure center as compared to those of the hospital.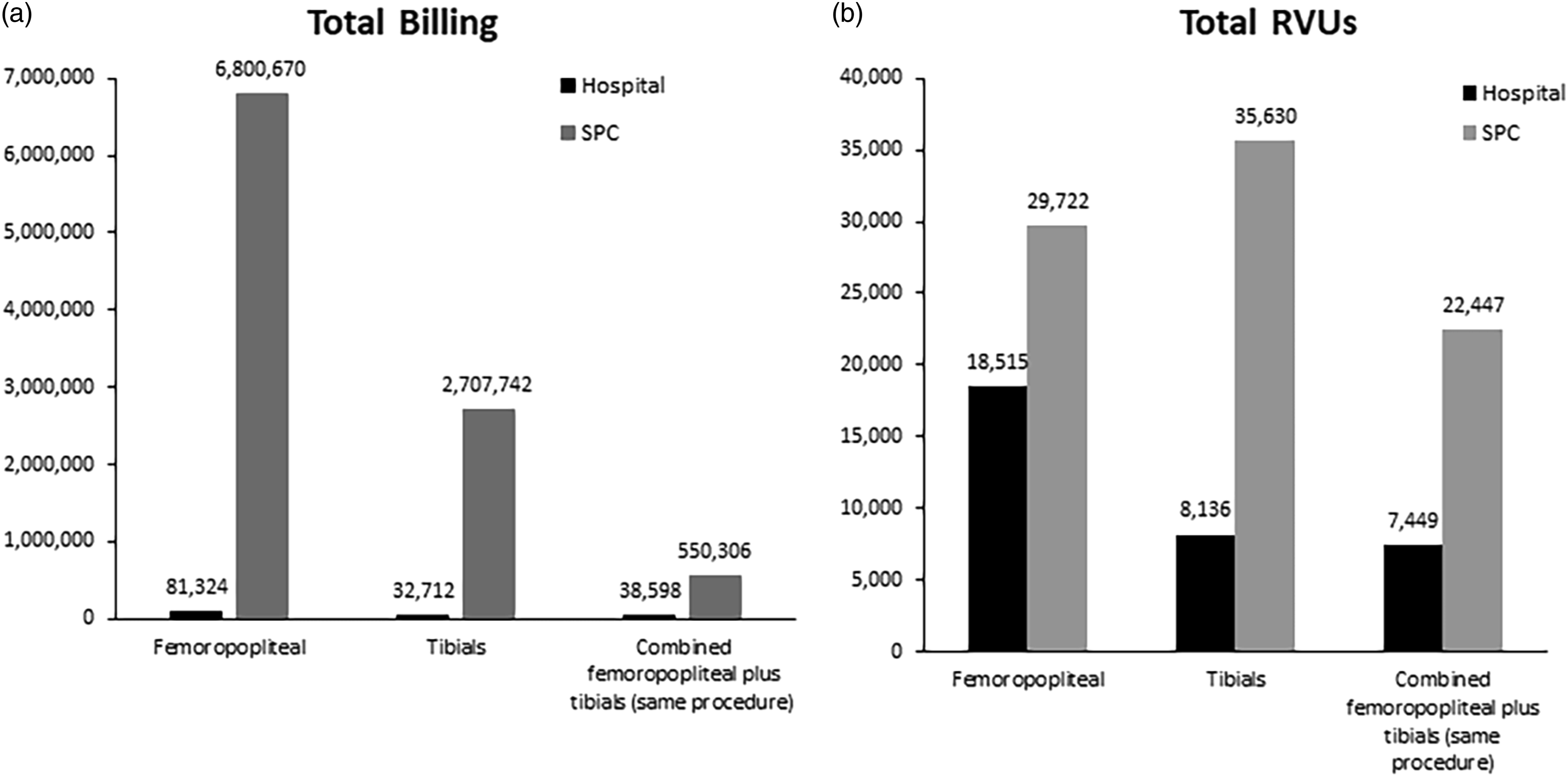
Discussion
Over the past two decades, the amount of outpatient facilities has increased substantially in America. 1 The vast majority of these facilities are run by private physicians’ groups, creating a parallel system to the traditional hospital-based concept.4–7 The most appealing advantages for these practices is the ability to retain the facility fees for all procedures and to provide a more flexible scheduling to their patients and physicians. A few OBLs reporting their results have some university affiliation, 4 but the number of current publications originated from fully dedicated academic SPCs run by vascular surgeons performing endovascular procedures is dismal. Further, endovascular procedures performed in an outpatient basis by vascular surgeons in dedicated academic centers is inexistent.
A variety of procedures can be safely performed in an OBL by several different specialized physicians (interventional radiologist, vascular surgeons, vascular medicine physicians, nephrologists, and interventional cardiologists). 8 Competition is fierce if several OBLs exist in a highly populated area. Specialized facilities dedicated to dialysis access work, the so-called “access centers” and to vein treatment (“vein centers”) are examples of outpatient facilities competing in this broad outpatient-based endovascular market.9,10 The most common type of procedures performed by a specific OBL rely on the regional healthcare needs surrounding the OBL, nearby presence of other specialized OBLs (vein and access centers), and its referral pattern. Jain and colleagues reported dialysis access work as the most common type of procedures performed in their OBL. 4 In a series of 5134 patients also treated by vascular surgeons in another two OBLs located in California and Texas, dialysis access work was also the most common procedure performed. 5 In our series, lower extremity angiography with or without intervention was the most common procedure performed. The reason for this pattern is the regional need for limb salvage interventions and several well-established dialysis and vein centers in our metropolitan area.
Lower extremity angiography was the most common procedure in our SPC. The infrainguinal arterial interventions were divided in balloon angioplasty alone, balloon angioplasty plus stenting, or atherectomy with or without stenting. Atherectomy was the most common arterial intervention device utilized, which is in consonance with national trends.11,12 The preference for atherectomy versus other procedures was mostly based on operator’s preference. Atherectomy was readily available in our OBL, and the vascular surgeons are very familiar with its use. Our outcomes following inhospital and outpatient atherectomy have been presented elsewhere. 13
The morbidity and mortality rates of OBLs have been reported as low. Jain and colleagues reported 18 (0.6%) deaths out of 2822 patients treated in their OBL and 26 (0.9%) other complications. Lin and colleagues also reported a very low mortality rate (18%, 9 patients) in the largest OBL series recently published; none of the deaths in this series were related to procedures.4,5 No death occurred in our OBL, but this is likely related to the smaller amount of procedures performed in our SPC compared to other large series. Our complication rate (1.1%) is also similar to other series. However, another smaller series of 235 patients reported a complication rate as high as 5% following peripheral vascular procedures . 14 Closure devices are utilized in large scale in ours and other procedure centers; the most common infrainguinal arterial complications in several publications remains pseudoaneurysms or access thrombosis, which nowadays can be potentially caused by the use of closure devices. The likelihood of having complications is related to the number of cases performed in an OBL according to Lin and colleagues’ findings. 5 Thus, smaller series tend to report higher complication rates which is largely based on a learning curve. Patient selection is heavily emphasized in all series reporting OBL results as a salutary selection bias. Our patient eligibility criteria are very similar to those of other OBL experiences.
The unique characteristic of our SPC as a university-based, dedicated academic facility makes our report relevant as it serves as a starting point for other future University-based endovascular OBLs run by vascular surgeons.12,15 As Figure 3 depicts, the appropriate case volume in the hospital will ultimately shift over time toward the OBL until it reaches a plateau. In our OBL, initial reimbursement helped to offset losses related to the academic division operations until profits were generated and a decision was made to pay out bonuses to those who strived to bring more business to the OBL. The Division of Vascular Surgery had complete control over the OBL financial landscape, which greatly differed from hospital administration control over overall finance and operation decisions. However, it is not possible to compare financial markers with other publications due to paucity of data from other academic OBLs.
Many would argue the billing amount, which correlates to a fraction in terms of collections, is much higher at the OBL compared to the hospital charges in Figure 4. The reason for this discrepancy is that the facility fees and other parts of reimbursement for service are collected by the OBL, while the hospital billing reflects only the physicians’ fees. Figure 4 provides a great correlation between the monetary potential of an academic OBL versus reimbursement obtained from a hospital. However, several major differences between an academic and privately owned OBL are the relationships between vascular surgeons and administration, which is virtually inexistent in private practice, flexible in regard to purchasing supplies and to widely negotiate prices, and regulations on relationships between OBL and the industry which is more strictly enforced in a university setting.
Limitations
The relative small number of patients gathered from our initial outpatient experience decreases the statistical power of some of our inferences. The low number of complications also hinders our ability to show significance of potential outcome predictors. The financial data provided was largely based on procedure codes which might have skewed upward the billing amount reported. The costs involved in running the SPC, the actual balance, and also the department taxation from the university administration were not available for analysis; therefore, we were not able to report the SPC profitability.
Conclusions
Vascular procedures performed in an academic outpatient office setting are safe. Patient selection is key to avert adverse outcomes. Peripheral arterial interventions are often performed in patients with critical limb ischemia. From a financial perspective, academic procedure centers can be successful if a clear communication among administration, doctors, and referring doctors exist.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.