
Abstract
Objective
This study aims to investigate the methods for rat spinal cord ischemia injury models with a high long-term survival rate.
Methods
The rats were divided into three groups: the treatment group, the control group, and the sham operation group. The treatment group had a blocked thoracic aorta (landing zone 3 by Ishimaru – T11) + aortic bypass circulation for 20 min. In the control group, the thoracic aorta at the landing zone 3 was blocked for 20 min. In the sham operation group, only thoracotomy without thoracic aortic occlusion was performed. The mean arterial blood pressure (MABP) of the thoracic aorta and caudal artery before and after thoracic aortic occlusion was monitored intraoperatively. Spinal cord function was monitored by a transcranial motor evoked potential (Tc-MEP) during the operation. Spinal cord function was evaluated by the BBB scale (Basso, Beattie, & Bresnahan locomotor rating scale) scores at multiple postoperative time points. The spinal cord sections of the rats were observed for 7 days after surgery, and the survival curves were analyzed for 28 days after surgery.
Results
After aortic occlusion, the MABP of thoracic aorta decreased to 6% of that before occlusion, and the MABP of caudal artery decreased to 63% of that before occlusion in the treatment group. In the control group, the MABP of both thoracic aorta and caudal artery decreased to 19% of that before occlusion. The Tc-MEP waveform of the treatment group disappeared after 6 min, and that of the control group disappeared after 8 min until the end of surgery. There was no change in the Tc-MEP waveform in the sham operation group. The BBB score of the treatment group decreased more obviously than the control group, and there was a significant difference. There was no decrease in the sham group. Spinal cord sections showed a large number of degeneration and necrosis of neurons, infiltration of inflammatory cells, and proliferation of surrounding glial cells in the treatment group. In the control group, multiple neurons were necrotic. The histology of the sham operation group was normal. The 28-day survival rate of the treatment group was 73.3%, which was higher than the control group (40.0%), and there was a significant difference (p < 0.05).
Conclusion
Thoracic aortic occlusion combined with aortic bypass is an effective modeling method for rats with accurate modeling effects and high long-term survival rates.
Introduction
The anatomical structure of spinal cord vessels in rats is roughly similar to that in humans, and surgical infection is relatively rare, so rats are the most commonly used spinal cord ischemia injury (SCII) treatment animals.1,2 Current methods for establishing rat SCII models include occlusion of the aortic arch., thoracic aorta, and abdominal aorta, and occlusion methods include open surgery or interventional techniques.1,3–5 In the occlusion of the aortic arch. or thoracic aorta, ischemia of the spinal cord at the distal end of the occlusion site will cause ischemia of the abdominal organs, resulting in the animal’s death.3,5,6 Although occlusion of the infrarenal aorta can avoid the ischemia of the abdominal organs, the scope of the spinal artery blocked in this way is small and cannot cause sufficient SCII.7–9 Moreover, the mechanism of this method is different from that of clinical SCII, which leads to the deviation between animal experiments and clinical studies.
In this study, we explored the preparation method of a simulated clinical long-term survival rat model of SCII, namely thoracic aortic occlusion and bypass circulation method. The traditional method of thoracotomy occlusion of the thoracic aorta was used as a control to establish the rat model of long-term survival of SCII, and the effect was better. Our study is reported as follows.
Materials and methods
Treatment animals and grouping
The Animal Experiment Ethics Committee of Kunming Medical University (2017) reviewed and approved this study, ethical review L No. 36, following the 3R principle. A total of 73 SD (Sprague Dawley) healthy male rats, weighing 450–500 g, aged 13 weeks and rated SPF (specific pathogen free), were purchased from the treatment Animal Center of Kunming Medical University (SCXK(Yunnan)K2020-0004). Before the experiment, the rats were fed with standard feed and free drinking water for 1 week in the Laboratory Animal Center (SYXK(Yunnan)K2020-0006) of Kunming Medical University. The humidity was 50–60%, the room temperature was 24 ± 1°C, the day and night cycle was 12 h, and the light and ventilation were good. As shown in Figure 1(b), all rats were randomly divided into three groups (25 rats in the treatment group, 25 rats in the control group, and 23 rats in the sham operation group). Then, the rats from each groups were randomly divided into three experiments, including measurement of MABP, Tc-MEP monitoring and BBB score. (a) Schematic diagram of thoracic aortic occlusion and aortic bypass circulation. A bypass tube supplies the distal aorta during thoracic aortic occlusion. (b) The flow diagram: All rats were randomly divided into treatment group (group-T), control group (group-C) and sham operation group (group-S). Then the rats from each groups were randomly divided into three experiments, including measurement of MABP, Tc-MEP monitoring and BBB score.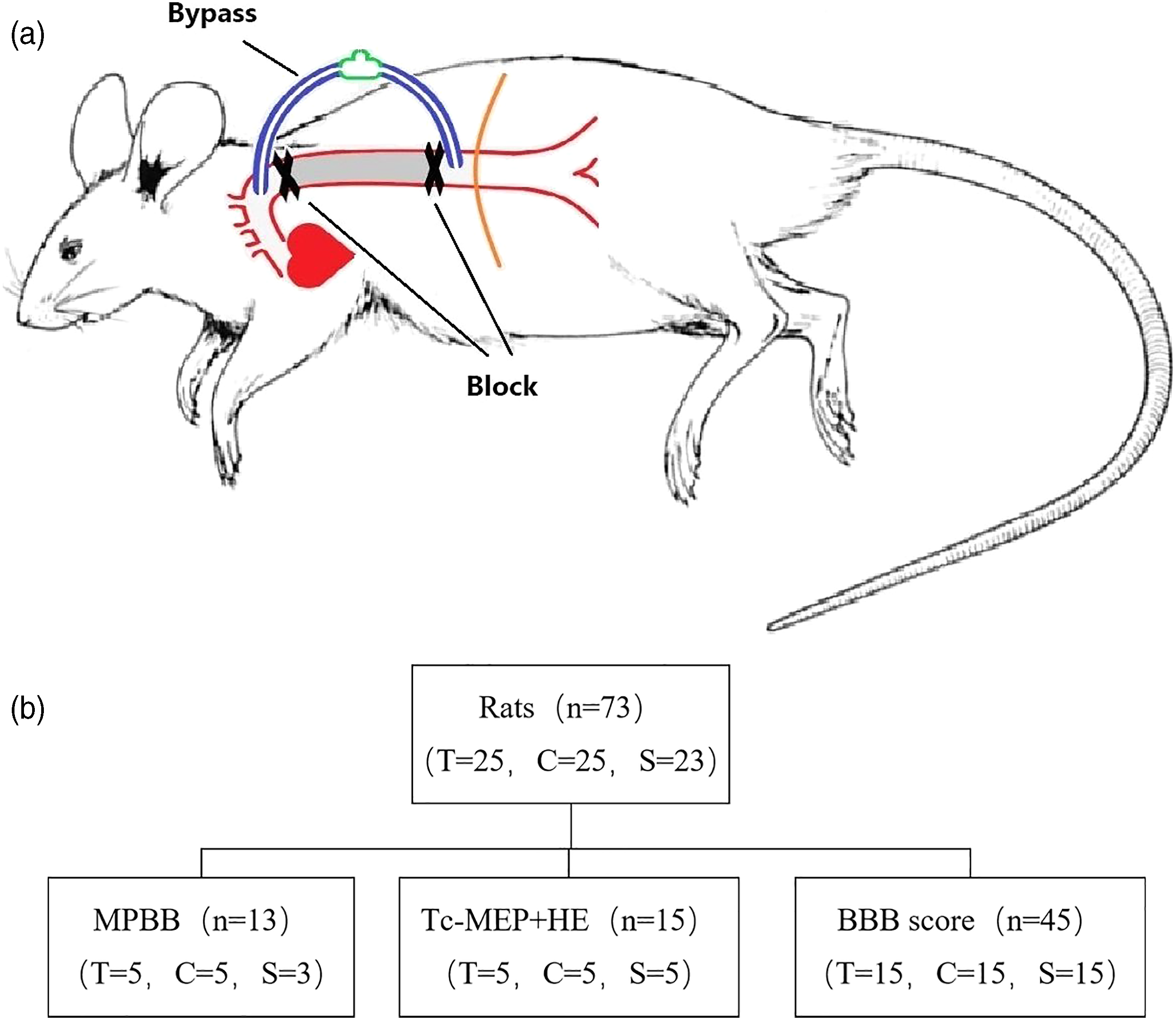
The treatment method
Animal anesthesia
Isoflurane-induced anesthesia was used. A venous catheter (PE-10) was inserted into the left external jugular vein to continue the infusion of ketamine (25 mg/kg/h). Tracheal intubation was given, and mechanical ventilation was performed. Isoflurane was discontinued after stabilization. After the surgery, the ketamine infusion was discontinued. The tracheal intubation was removed after recovery of spontaneous respiration.
Operation method
Rectal temperature was monitored with a flexible probe in all rats. The rats were put under the body heat preservation pad equipped with an infrared heating lamp. The heat preservation pad and infrared heating lamp were used to maintain the body temperature at 37.5 ± 0.5°C.
The treatment group
Rats were placed in the right decubitus position with a left posterolateral thoracic incision. The fourth intercostal area was exposed, the descending aorta was separated 0.5 cm from the subclavian artery, the proximal end was sutured with a purse-string suture using 7-Prolene thread and silk thread was inserted close to the distal end of the purse-string suture as the proximal occlusion site at the landing zone 3. The eighth intercostal area was exposed. The distal purse-string was sutured to the aorta above the diaphragm. The obstruction thread was sewed close to the proximal end of the diaphragm as the distal occlusion site (T11). An 18G trocar was inserted from the proximal purse-string, and 3 mg/kg of heparin was pushed into the tube. The distal purse-string was catheterized in the same way. A three-way switch was used to connect the proximal and distal ducts to form a bypass circulation of the thoracic aorta. The proximal and distal ends of the thoracic aorta were blocked with noninvasive arterial clips (Figure 1(a)). After 20 min of occlusion, the noninvasive clamp was opened to restore aortic blood flow. Heparin was neutralized in the body with protamine (1:1). Fluids were replenished appropriately through the three-way switch as needed. The trocar was pulled out, and the purse-string was tied. Hemostasis and chest closure were performed. Erythromycin ointment was applied to the surgical incision. The patients were caged separately after surgery. An intramuscular injection of 200,000 units of penicillin was given twice a day for seven consecutive days. Rats with urinary retention were artificially assisted in urinating and defecating three times a day. Attention was paid to the prevention of infection, pressure sores, and autophagy.
The control group
The method of thoracotomy was the same as that of the treatment group. 1 mg/kg of heparin was injected subcutaneously prior to aortic clipping. The thoracic aorta was blocked by a single noninvasive artery clip at the landing zone 3, and the clip was opened 20 min later. Subsequent treatment was the same as the treatment group.
The sham operation group
The method of thoracotomy was the same as that of the treatment group, but the thoracic aorta was not blocked.
Measure mean arterial blood pressure
The thoracic aorta and caudal artery blood pressure was monitored before and after thoracic aortic occlusion in 13 rats: three rats in the sham group, five rats in the control group, and five rats in the treatment group. The anesthetic and surgical methods are the same as above. The blood pressure of the thoracic aorta (reflecting the perfusion pressure of the thoracic spinal artery) and caudal artery (reflecting the perfusion pressure of the celiac artery) were monitored. The method was as follows. At the T8 level of the thoracic aorta, a 7-Prolene purse-string suture was used to place a venous catheter (24 G), and a pressure sensor was connected. Mean arterial blood pressure (MABP) was continuously monitored before and after thoracic aortic occlusion and during 30 min of reperfusion. A proximal caudal incision was performed to expose the caudal artery, and an intravenous catheter (24G) was inserted. A pressure sensor was connected to monitor the distal MABP throughout the process.
Transcranial motor evoked potentials (Tc-MEP) monitoring
A needle-shaped electrode was selected, and the stimulation electrode was placed at the C1 and C2 points on the head. The recording electrodes were placed on the proximal muscles of the upper extremity and the gastrocnemius muscles of the hind extremity. The Cadwell 32 channel intraoperative monitoring system was used (Cascade, Cadwell, USA). Baseline data were obtained before thoracotomy and monitored every minute after aortic occlusion and every 2 min after waveform disappearance until the end of surgery. All-or-none of the Tc-MEP abnormalities were judged as the standard, and the loss of potential indicated an absence of spinal cord function. 10
Spinal motor function assessment
A total of 15 rats from each group were used to evaluate post-SCII locomotion function by the BBB score.11,12 The hind limb movements, forelimb to hind limb coordination, fine motor functions of the claw, and whole body movements were evaluated in the BBB score with a discrete scale ranging from 0 (no hind limb movement) to 21 points. The normal movement is score 21, including consistent toe clearance, consistent trunk stability, coordinated gait, and tail is consistently up. The lower score suggested the damages of locomotion function. The outcome measures of BBB score were performed by two independent examiners blinded to the experimental groups, and the mean of the two outcomes was used as the final BBB score of each rat. The scores were evaluated at 0 days preoperatively and 1, 3, 5, 7, 14, and 28 days postoperatively.
Immunohistochemical analysis of the spinal cord
A total of five rats from each group were euthanized (150 mg/kg 1% pentobarbital sodium was intraperitoneally injected) 7 days after the operation. Immediately, the rats were transcardially perfused with 0.9% normal saline, followed by 10% paraformaldehyde. Then, the spinal cord was removed and fixed with 4% paraformaldehyde. After dehydrated overnight with 30% sucrose solution in 4% paraformaldehyde, spinal cord sections were made, and the spinal cord at the T8 level in the central ischemic area was stained with hematoxylin-eosin (H&E) and observed under the microscope.
Statistical analysis
Statistical analysis and plotting were carried out using GraphPad Prism software (version 7.0). MABP and BBB were scored by one-way analysis of variance. The Kaplan–Meier method was used for survival analysis, and the log-rank test was used to compare the survival rates between the two groups. p-values <0.05 were considered statistically significant.
Results
MABP
Comparison of mean arterial pressure (MABP) of thoracic aorta and caudal artery in three groups at different time points during operation.
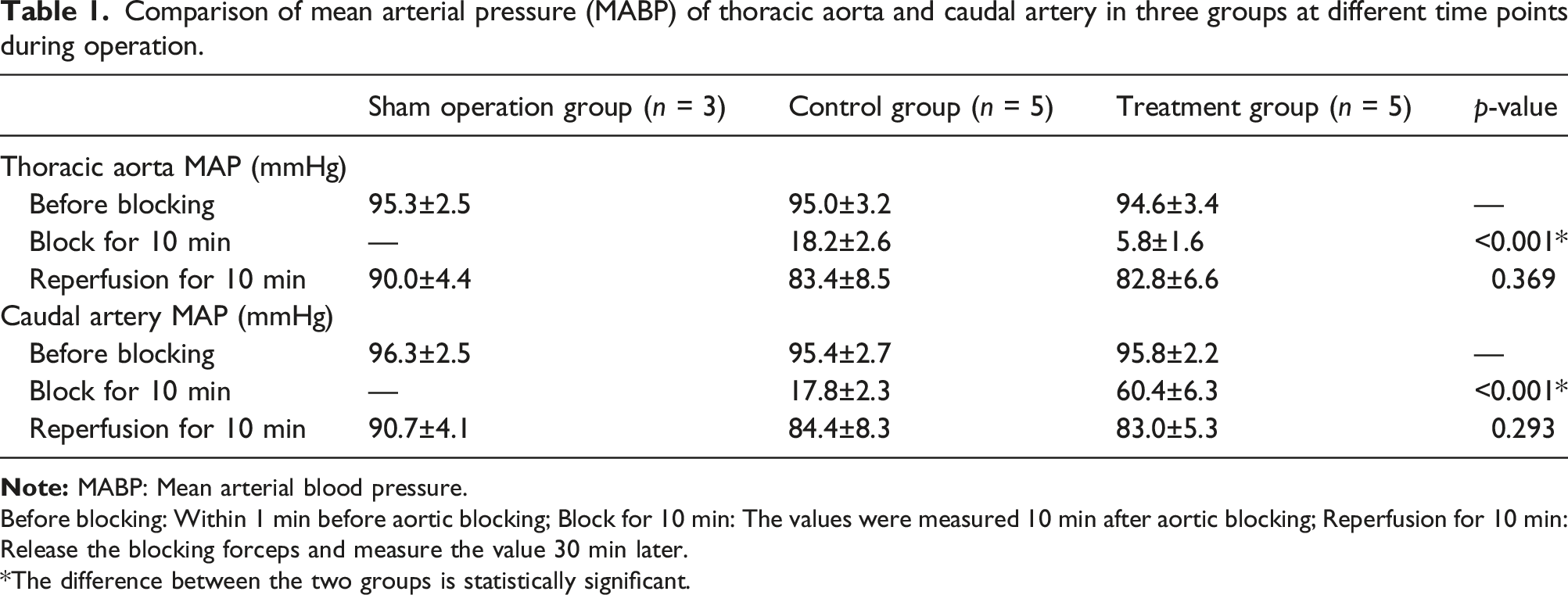
Before blocking: Within 1 min before aortic blocking; Block for 10 min: The values were measured 10 min after aortic blocking; Reperfusion for 10 min: Release the blocking forceps and measure the value 30 min later.
The difference between the two groups is statistically significant.
Results of Tc-MEP
After stabilizing from anesthesia, the Tc-MEP wave was detected as a biphasic wave, which was used as a baseline. The upper extremity Tc-MEP was used as a reference, and the waveform of the lower extremity Tc-MEP disappeared after thoracic aorta occlusion in both treatment and control groups. The time points of disappearance were different, with the treatment group averaging 6 min and the control group averaging 8 min. After blood flow was restored to the aorta, the Tc-MEP waveform still did not recover at the end of the operation in both groups, indicating impaired spinal motor function caused by spinal cord ischemia. There was no change in the Tc-MEP waveform in the sham operation group (Figure 2). The disappearance of transcranial motor evoked potential (Tc-MEP) waveforms after thoracic aortic occlusion indicates impaired spinal motor function.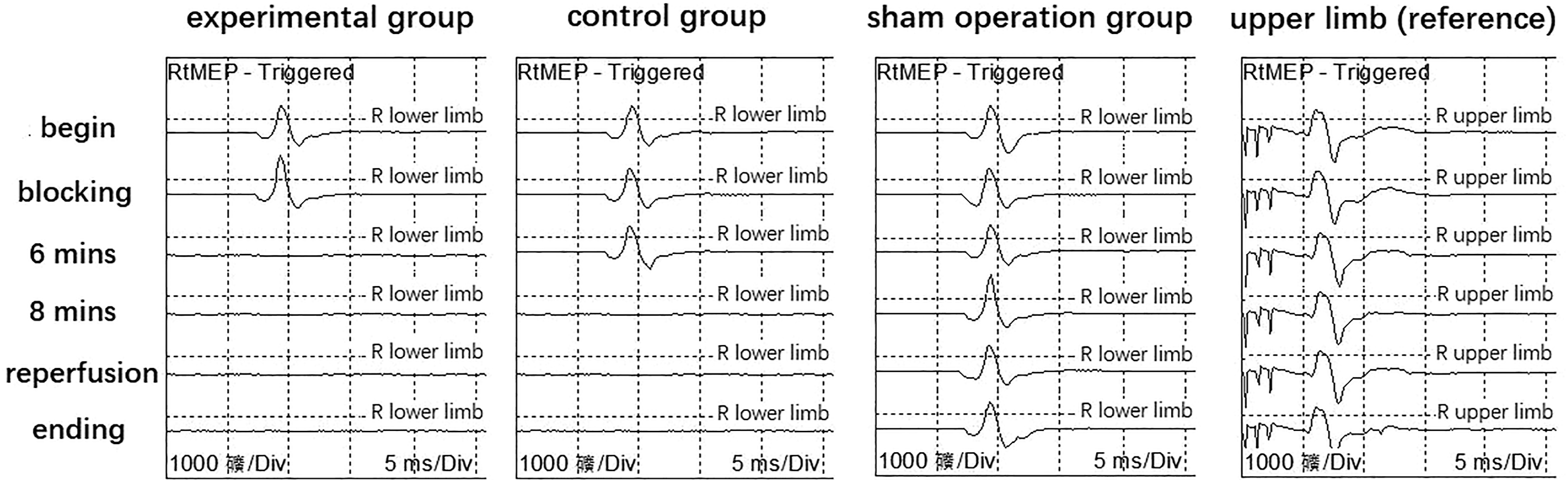
BBB locomotion score
The BBB scores of the treatment and control groups decreased after the operation, and the treatment group was significantly lower than the control group (p < 0.05). There was partial recovery over time. There was no decrease in BBB scores in the sham operation group (Figure 3). Line chart of the BBB scale (Basso, Beattie & Bresnahan locomotor rating scale) motion score. There was a significant difference between the treatment group and the control group. (Note: * p < 0.05, ** p < 0.01, *** p < 0.001, ****p < 0.0001).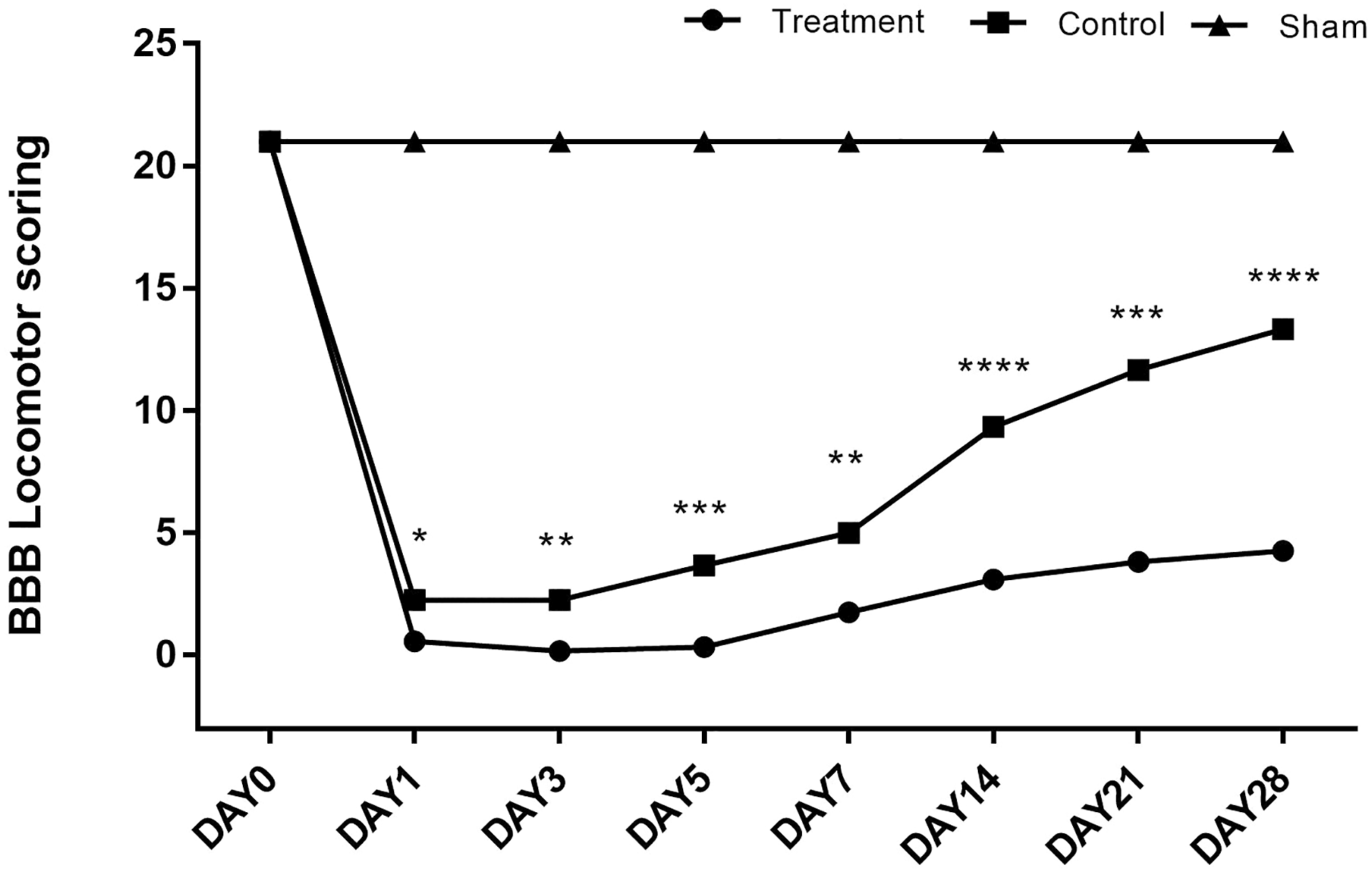
H&E staining of the spinal cord
In the treatment group, many neurons were denatured and necrotic, accompanied by infiltration of inflammatory cells and proliferation of surrounding glial cells. In the control group, neuronal degeneration, multiple neuronal necroses, inflammatory cell infiltration, and glial cell proliferation were observed. In the sham operation group, the spinal cord tissue structure was intact, the neuron morphology was normal, the distribution was uniform, the nuclear structure was clear, and the capsule was complete (Figure 4). Histological changes of the thoracic spinal cord in rats 7 days after surgery (H&E staining) (X200). (a) In the sham operation group, the histology was normal. (b) In the control group, the number of neurons decreased, and inflammatory cells were infiltrated. (c) In the treatment group, few neurons survived, and inflammatory cells infiltrated.
Survival analysis
Taking 28 days after surgery as the endpoint of the experiment, the survival rate of the treatment group was 73.3%, and the control group was 40.0%, showing a significant difference (Figure 5). The causes of death in the treatment group were excessive blood loss and infection. In the control group, death was concentrated 3 days after surgery, and the causes of death were kidney infection, intestinal ischemia and infarction, excessive blood loss, pulmonary infection, and bladder infection. The causes of death in the sham operation group were excessive blood loss and pulmonary infection. The 28-day survival rate (Kaplan–Meier survival curve, log-rank test) was significantly different between the treatment and control groups. * p = 0.0412.
Discussion
SCII is a serious complication of thoracic and abdominal aortic aneurysm surgery. Previous studies have shown that some methods in protecting SCII have been widely published with reproducible results across human studies and animal models, including systemic or regional hypothermia and cerebrospinal fluid drainage.13–16 At present, the pathophysiological mechanism of SCII is remain unclear and the preparation of treatment animal models simulating clinical practice is of great significance for the study of SCII. However, the survival time of current SCII models occluding the thoracic aorta is short,1,3,4 which limits the in-depth study of SCII and reperfusion injury.
This treatment method is an improvement of the model of SCII established by occlusion of the thoracic aorta in rats. While guaranteeing to block most of the blood supply to the spinal cord, the proximal and distal bypass circulation of the blocked segment can be established to provide blood supply to the distal organs during the occlusion period to avoid the distal ischemic spine injury caused by aortic occlusion. Therefore, it provides an effective method for establishing a long-term survival model of spinal cord ischemia. Intraoperative evoked potential monitoring, postoperative BBB scores, and spinal cord pathologies all confirmed the establishment of the spinal cord injury model. Compared with traditional thoracic aortic clipping, SCII was confirmed, and the survival rate at 28 days was improved.
The spinal cord is supplied by a network of longitudinal spinal anterior and posterior arteries from the vertebral artery and root arteries from the aorta.1,2 In this study, the aortic occlusion range was selected as T4–T11, covering the main area of the emitting segments. After aortic occlusion, aortic blood pressure at the T8 level was measured, reflecting perfusion pressure in the spinal artery. The treatment group was significantly lower than the control group (5.8 ± 1.6 vs 18.2 ± 2.6), which explains the severity of spinal cord injury in the treatment group. During aortic occlusion, the caudal blood pressure reflected the perfusion blood pressure of the abdominal organs, which was much higher in the treatment group than in the control group (60.4 ± 6.3 vs 17.8 ± 2.3). Ischemic injury of the abdominal organs was reduced, and the necropsy of the dead rats also confirmed the hypothesis.
Compared with the traditional method of occlusion of the thoracic aorta, the effect of SCII in thoracic aortic occlusion combined with aortic bypass circulation was more accurate for the same occlusion time. At the same time, ischemic injury of the abdominal organs was avoided, which was beneficial to the long-term survival of rats. Though large animal models may more accurately reflect some of the techniques and adjuncts possible with humans, the costs of large animal models are significantly higher than that in rat models of SCII. Certainly, some of the inherent differences in the neurological and vascular anatomy between humans and rats complicate the ability to translate rat results into meaningful human interventions. Therefore, more study in rat models of SCII should been explored to translate these results into clinical application. However, this method of occlusion in treatment group is more complex and needs a more skilled and delicate surgical procedure compared to traditional method. In addition, our study found that this operation in treatment group had a longer operative time and a higher complication rate compared to traditional method, such as excessive blood loss and intraoperative death. Therefore, the operation requires a higher degree of finesse and good animal experiment operation technology.
Conclusion
A long-term survival rat model of SCII was established by thoracic aortic occlusion and aortic bypass. The treatment results showed that the model was effective and had a high long-term survival rate, and could be used as a good choice for the clinical SCII model.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research on the application of basic technology in Yunnan Province (2017FE468-192).
Ethics approval
This study was conducted with approval from the Animal experiment ethics committee of Kunming Medical University (No: 2017-L-36).