
Abstract
Objectives
This thesis aims to explore the relationship between tea consumption and ankle–brachial index (ABI) and further studies the relationship between tea consumption and lower extremity atherosclerosis.
Methods
This is a cross-sectional, epidemiological survey of 17,373 subjects selected from the staff of Kailuan Group who had come to Kailuan General Hospital for a health examination from January 2016 to December 2017. Tea consumption was obtained by questionnaires. ABI was measured using an automated analyzer. The other data, such as age, gender, body mass index (BMI), and so on, was collected on the same day of the health examination results. The relationship between tea drinking habits and ABI was studied using logistic regression and multivariate linear regression analysis.
Results
Among the 17,373 analyzed subjects, the difference in age, gender, BMI, heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), uric acid (UA), C-reactive protein (CRP), fasting blood-glucose (Fbg), and ABI was statistically significant in the tea-drinking group and the nontea-drinking group (p < 0.05). Multiple logistic regression models revealed that tea consumption was a positive predictor for ABI (odds ratio (OR) = 0.782, confidence interval (CI), 0.615–0.994) (p < 0.05). Multivariate linear regression analysis of the ABI value showed that frequent tea-drinking has a positive correlation with the ABI value (p < 0.05).
Conclusions
The higher tea consumption is significantly associated with higher ABI which means less risk for lower extremity atherosclerosis.
Keywords
Introduction
Since atherosclerosis usually has no clinical manifestations in the early stage, it is often detected only at an advanced stage or following a cardiac or cerebra vascular event. These diseases usually occur suddenly and fatally. Therefore, early prevention for atherosclerosis is of great significance. 1 As early as 1967, tea was shown to reduce the risk of developing atherosclerosis, though it could not treat atherosclerosis that had already developed. 2 In recent years, studies have also shown that drinking tea can change the level of risk of atherosclerosis, such as reducing the fasting blood glucose (Fbg) and slowing age-related decreases in HDL-C concentrations.3–5 As a manifestation of atherosclerosis in the lower limbs, peripheral artery disease (PAD) can impair walking and even lead to tissue loss, infection, and amputation in severe cases. 6 The major screening test for PAD is the anklebrachial index (ABI), which can measure the ratio of the ankle and brachial systolic blood pressures. 7 ABI has been used as the golden standard diagnostic test for assessing the severity of PAD in lower limbs. The ABI cut off of < 0.9 has been shown to have a greater sensitivity and specificity for angiographically verified peripheral arterial stenosis.8,9 In the current literature reports, they have shown that age and gender have a certain influence on ABI value. The ABI increased with age and was lower in women than in men. 10 Some studies showed that lower ABI was modestly but independently associated with a higher risk of incident diabetes in the general population.11,12 However, the effect of tea drinking on ABI values has not been reported yet. This thesis aims to explore the correlation between tea drinking and ABI values in people participating in physical examination.
Materials and methods
Subjects
The subjects were selected from the staff of Kailuan Group who came to Kailuan General Hospital for a health examination from January 2016 to December 2017. A total of 17,373 subjects who had tea-drinking records and ABI values participated in the survey (ABI outliers have not been included). All subjects were informed that the results of the survey would be used in this thesis, and the participation of subjects was voluntary. The survey procedures and informed consent process were approved by the research protection committee of the hospital.
Recording of tea drinking
All subjects were asked whether they drank tea. If they reported tea consumption, the types and frequency of tea drinking were recorded. The subjects were divided into two groups: the tea-drinking group and the nontea-drinking group. In the survey, the types of tea included black tea, green tea, scented tea, and other kinds of tea. The frequency of tea drinking was divided into four groups as follows: less than once a month, 1–3 times a month, 1–3 times a week, and at least 4 times a week. If the subjects drink tea less than once a year, we consider them to be in the nontea-drinking group. All information on subjects’ tea consumption was recorded by questionnaires and confirmed by physicians.
Measurement of ABI value
Using a validated automatic device (BP-203RPE, II form PWV/ABI and Omron-Colin, Japan), the ABI was measured. The device can simultaneously measure pulse volume in the brachial and ankle arteries based on an oscillometric method with bilateral arm and ankle blood pressure (BP). The ABI was measured at rest in the supine position twice in at least 5 min. It was calculated bilaterally as the ratio of SBP in the ankle to the highest systolic BP in the arm. The value of measurements was averaged. In bilateral ABI values, take the lower one as the final recorded value. In this thesis, if the measured ABI was < 0.9, the subjects were considered abnormal. The value of greater than or equal to 0.9 was deemed to be normal.
Records of other factors
Before conducting the questionnaire and ABI examination, the age and gender of subjects were recorded. Body mass index (BMI) was calculated as body weight divided by the squared height (kg/m2). Heart rate (HR), systolic blood pressure (SBP), and diastolic blood pressure (DBP) were all measured by trained nurses while observers were seated and calm. SBP and DBP were averaged after measuring three times. Total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), uric acid (UA), C-reactive protein (CRP), and fasting blood-glucose (Fbg) were all recorded from the reports of the health examination of this time. Obesity was defined as BMI ≥ 25 kg/m2. 13 HR between 60 and 100 was considered normal. Otherwise, it was abnormal. The TC/HDL-C ratio was calculated and categorized as either ≤ 5.0 or > 5.0. Hypertension was defined as a mean SBP ≥ 140 mmHg and/or mean DBP ≥ 90 mmHg. CRP value of < 5 is normal, and ≥ 5 is abnormal. Diabetes was defined as an Fbg ≥ 7.0 mmol/L.
Statistical analysis
The test data were input by the unified training specially assigned person and uploaded to the laboratory computer’s server through the network to form a database. SAS 9.4 (statistical analysis system 9.4) software was used to analyze the data. All parametric values were expressed as mean ± standard deviation (SD). The counting data was expressed as percentage. When the variance of measurement data was not uniform, the median (25%, 75%) was adopted. One-way analysis of variance was used for enumeration data. Enumeration data with uneven variances used the KruskalWallis nonparametric test. For counting data, the chi-square test or Fisher’s exact test were used. In the survey, the value of ABI (≥ 0.9 or < 0.9) was used as the dependent variable. Tea drinking was used as the independent variable for logistic multivariate regression analysis. Moreover, other factors were used to correct the logistic regression. Odds ratios (OR) took 95% confidence intervals. Multivariate linear regression analysis was performed in the observed population with ABI as the dependent variable and tea-drinking frequency (times/weeks). Moreover, other factors were used to correct the logistic regression. p < 0.05 was statistically significant.
Results
Baseline data analysis
Among 17,373 subjects, there were 13,004 males and 4369 females. 13,666 subjects never drank tea and 3707 drank tea (908 cases who drank tea less than once a month, 955 drank tea 1–3 times a month, 824 drank tea 1–3 times a week, and 1020 drank tea at least 4 times a week). According to the recorded tea types, many subjects drink tea for one specific type of tea among the total of 3444 subjects (783 people drank black tea, 1321 people drank green tea, 922 people drank scented tea, and 418 people drank other types of tea).
Comparison of general baseline conditions between the tea-drinking group and the nontea-drinking group.
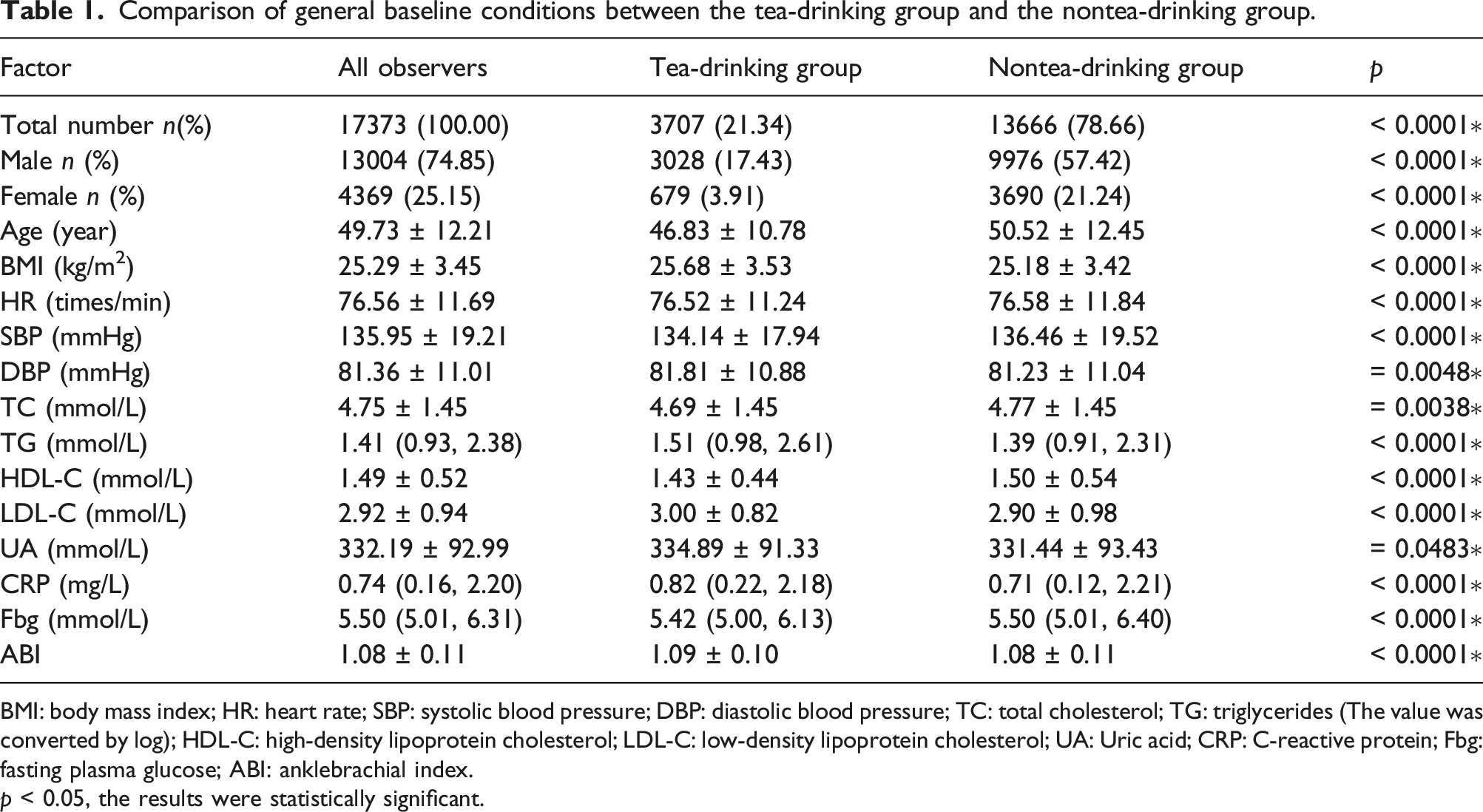
BMI: body mass index; HR: heart rate; SBP: systolic blood pressure; DBP: diastolic blood pressure; TC: total cholesterol; TG: triglycerides (The value was converted by log); HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; UA: Uric acid; CRP: C-reactive protein; Fbg: fasting plasma glucose; ABI: anklebrachial index.
p < 0.05, the results were statistically significant.
Comparison of general baseline of observers with different tea-drinking frequencies.

p < 0.05, the results were statistically significant.
Comparison of general baseline conditions among observers of different tea drinking types.
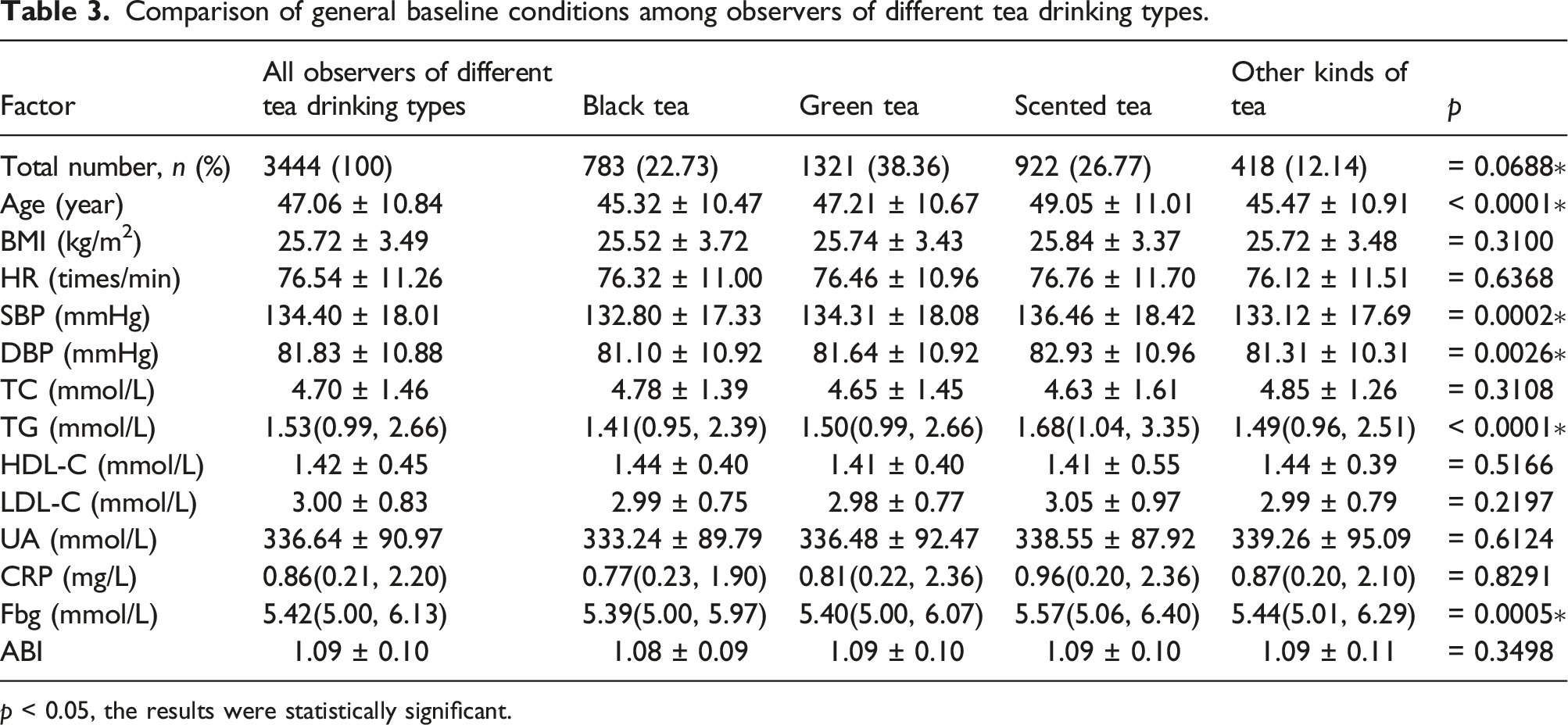
p < 0.05, the results were statistically significant.
Logistic regression analysis of ABI values
Multivariate logistic regression analysis of ABI values in the tea-drinking group versus the nontea-drinking group in all observers.
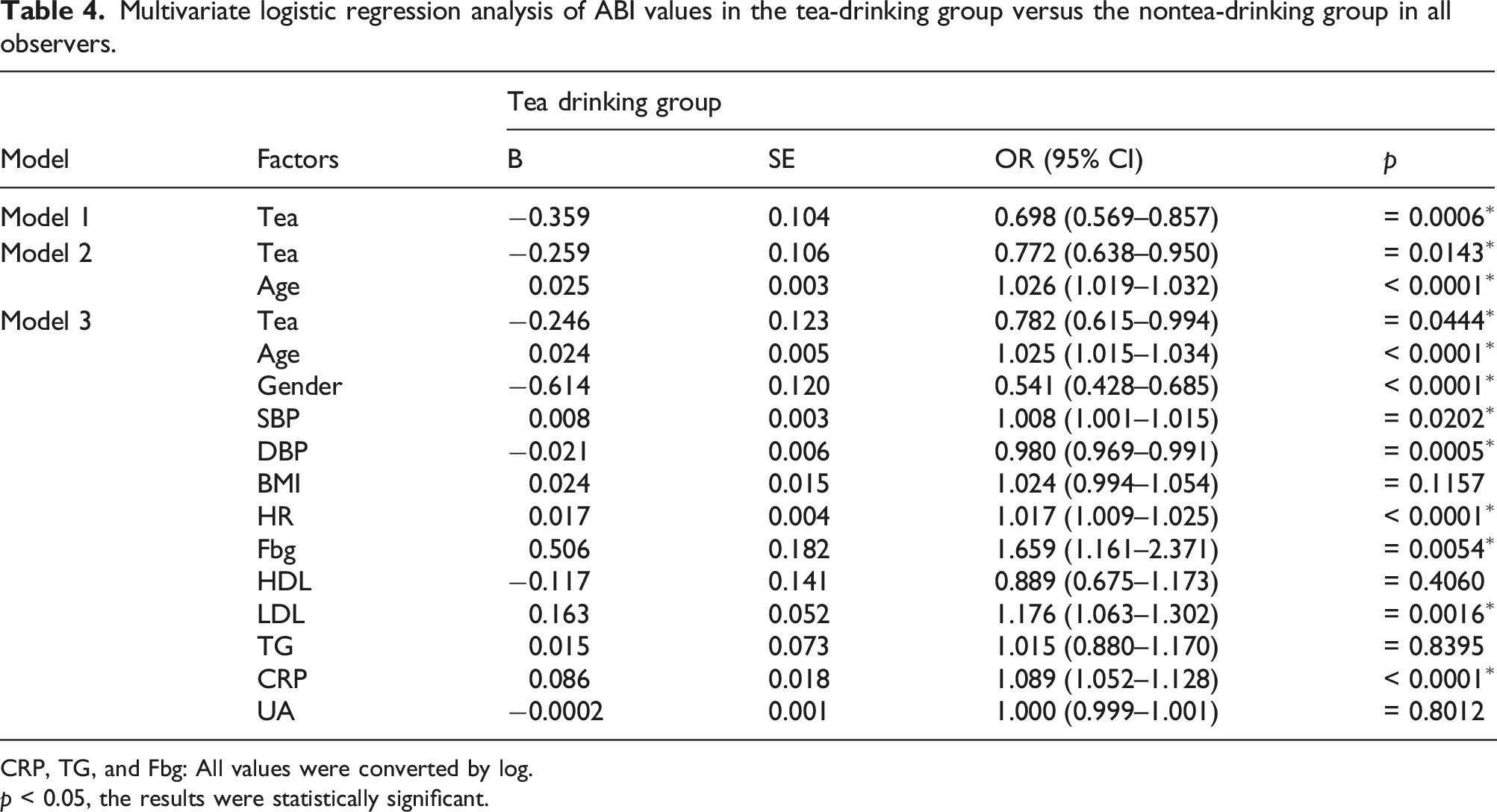
CRP, TG, and Fbg: All values were converted by log.
p < 0.05, the results were statistically significant.
Multivariate linear regression analysis of ABI value
Multivariate linear regression analysis of tea-drinking frequency influencing ABI values in all observers.
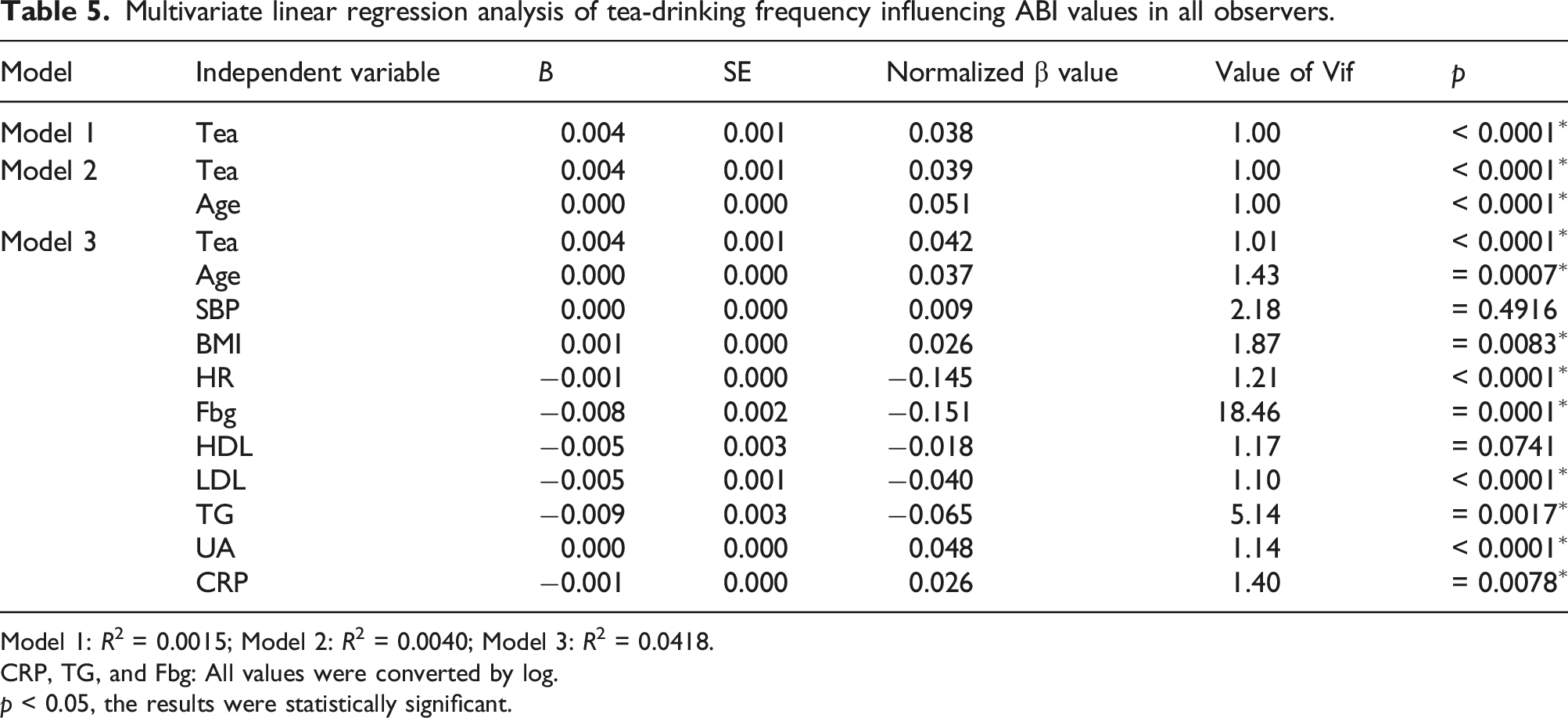
Model 1: R2 = 0.0015; Model 2: R2 = 0.0040; Model 3: R2 = 0.0418.
CRP, TG, and Fbg: All values were converted by log.
p < 0.05, the results were statistically significant.
Discussion
As one of the most common drinks, tea has been accepted by more and more people all over the world. The beneficial components of tea are mainly flavonoids and polyphenols, which have been proven to slow the development of atherosclerosis.14–18 Lower extremity atherosclerosis is one of the manifestations of atherosclerosis. As a predictive parameter for lower extremity atherosclerosis, the low value of ABI indicates a high risk of lower extremity atherosclerosis. 19 The relationship between ABI and tea drinking has not been reported in the literatures, which is also the focus of this thesis.
ABI < 0.9 indicates arteriosclerosis in the lower extremities. When ABI ≥ 0.9, the artery is defined as one in good condition although many studies have reported that a lower ABI (< 0.9) and higher ABI (> 1.3) are both associated with the higher risk of cardiovascular events. 20 This thesis did not include the ABI (> 1.3) because there were only 50 subjects’ ABI > 1.3. The data was deleted due to large disparities in the number of samples from other groups. In this thesis, after adjusting for the other factors of basic data, tea drinking as a protective factor can improve the ABI value by 0.782 times. ABI < 0.9 is associated with a higher risk of lower extremity atherosclerosis. The mechanism of tea that can reduce the index of arteriosclerosis is complicated, and it is also the focus of current research. Relevant studies showed that the protective effects of tea against the development of atherosclerosis were attributable to lowering blood lipid, reducing inflammation, and antioxidants of polyphenols and flavonoids.17,18 The results of several in vitro studies indicate that tea flavonoids also cause vasorelaxation which lowers blood pressure and reduces the risk of atherosclerosis. Results from a meta-analysis suggest that tea catechins can also significantly improve endothelial function, thereby providing an additional benefit for patients with cardiovascular disease.21,22 Meanwhile, in the linear regression analysis, the frequency of tea drinking was positively correlated with the value of ABI, and the difference was statistically significant. At present, a few studies on the relationship between tea drinking and atherosclerosis have been conducted. A meta-analysis demonstrated that daily consumption of either green or black tea, three cups/day, was associated with a reduced risk of ischemic stroke. 23 Studies showed that carotid plaques were less frequent with increasing tea consumption in women. 24 Moreover, high consumption of flavonoids was associated with decreased carotid atherosclerosis. 25 Changes in blood vessel conditions may require the longer term regular ingestion of tea. In the study, the last line of Table 2 states the opposite. The reason of non-statistically significant results of the ABI between two groups may be that the other factors are more influential. Some studies have shown that age and gender have a certain influence on ABI value. After adjusting for other factors, the frequency of tea consumption was still related with ABI. However, the specific frequency of tea consumption needs to be further studied in a large population.
The age and male ratios of the tea-drinking group were lower than those of the nontea-drinking group. From this perspective, younger women are more likely to drink tea than the older men. However, the ABI value was lower in older group, which could be explained by the sensitivity of ABI which was lower in elderly individuals and patients with diabetes. In addition, the increased incidence of arterial calcification can cause increased vascular rigidity and spuriously elevating the ABI in these individuals. 26 In the logistic regression analysis, age was a risk factor for lower extremity atherosclerosis with ABI values below 0.9, while gender (female) was protective. Related research showed that the ABI was lower in younger than older adults until 60–69 years, and lower in women than in men at all ages. 10 In logistics regression analysis, age as a risk factor increased the probability of abnormal ABI value by 1.025 times. Therefore, the stiffness and wave reflection of vascular is deemed responsible for age-related increases.
Although BMI was a risk factor for atherosclerosis, the 95% CI was 0.994–1.054 in the study, which was not statistically significant. On the one hand, the BMI values of the tea-drinking group and the nontea-drinking group were 25.68 and 25.18, respectively. The BMI between the two groups was in the obesity range (> 23.9), and the difference was small. The conclusion that the tea-drinking group can effectively lose weight may not be accurate. Studies have shown that increased visceral fat is associated with higher rates of atherosclerotic plaques, but on multivariate analysis, BMI was not independently associated with the atherosclerotic plaques. Studies showed that the relationship between BMI and subclinical atherosclerosis was partly mediated by BP and plasma glucose.27,28 A study of atherosclerosis risk in 5546 Chinese people showed that categorical BMI analysis did not reveal an increased mortality risk of atherosclerosis at any BMI category among the Chinese. 29 Therefore, BMI may not be a risk factor for lower extremity atherosclerosis.
In the logistic regression analysis, HR and SBP were risk factors for lower limb atherosclerosis with ABI values below 0.9, which could cause a higher risk of lower limb atherosclerosis by 1.017 and 1.008 times, respectively. HR was positively correlated with ABI in the multivariate linear regression analysis, while SBP was not linearly correlated with ABI. The study showed that dietary flavonoids present in green tea, including quercetin and epicatechin, could augment NO status (plasma S-nitrosothiols and nitrite) and reduce endothelin-1 concentrations—a potent vasoconstrictor. 23 Under the action of this mechanism, tea drinking can improve vasoconstriction and reduces SBP. Results of some population studies also suggest that long-term regular ingestion of tea may lower blood pressure. 30
As for the effect of drinking tea on blood lipid, the results of this thesis showed that the TC in the tea-drinking group decreased, but the TG and LDL-C increased, and the HDL-C decreased. Elevated blood lipids have been a risk factor for atherosclerosis in most studies.31–34
The effect of UA on ABI was not statistically significant in the regression analysis. Relevant studies also showed that UA value did not reduce the factors of atherosclerosis, which was consistent with this thesis. 35 The CRP value of the tea-drinking group was also higher than that of the non-tea-drinking group, but CRP values in both groups were in the normal range (0.068–8.2 mg/L). Therefore, the comparison of baseline data of CRP between the two groups had no clinical value. However, CRP was a risk factor for lower extremity atherosclerosis, while the risk was increased by 1.089 times in the regression analysis. Related research showed that CRP was an indicator of inflammation, reducing inflammation and plaque formation. This is consistent with the result of this thesis. 36
The Fbg of the tea-drinking group was also lower than that of the nontea-drinking group. Some studies revealed that tea consumption was associated with a decreased risk of diabetes and a reduced level of fasting blood glucose, which was consistent with the results of this thesis.11,12
Based on a comparison between different types of tea groups, the scented tea group had older age and higher blood pressure (SBP and DBP) and higher TG than other groups. One reason is blood pressure increased, and lipid metabolism decreases with age. On the other hand, green tea and black tea can lower blood lipids and prevent the onset of ischemic stroke.37–40 However, different types of teas are made in different ways, such as green tea (non-oxidized), black tea (oxidized), and other types of tea (maybe partially oxidized). The corresponding composition and content of different teas were complicated and diverse. 41 The other types of teas have been less studied for their effect on atherosclerosis at present. As for the types of tea, the number of black tea, scented tea, and other kinds of teas is < 30% of the tea consumers in our study. This is also a limitation.
In the relevant literatures, physical activity, dietary modifications, reductions in salt and alcohol consumption, and weight loss are also important interventions able to reduce arterial stiffening.42–44 In our study, tea drinking could be good for elevating the ABI and may reduce the risk of lower extremity atherosclerosis. The mechanism of tea consumption has been multifaceted. Nevertheless, the frequent habit of drinking tea may be more conducive to reducing the incidence of lower extremity atherosclerosis. Therefore, more studies on tea’s effect on lower extremity atherosclerosis should be made in the future.
Conclusion
In conclusion, after adjusting for possible affecting factors, higher tea consumption is significantly associated with higher ABI. Thus, drinking tea may be a primary preventative measure against lower extremity atherosclerosis. Further research should be conducted to explore the mechanisms of tea consumption and atherosclerosis.
Footnotes
Acknowledgements
First and foremost, I would like to express my deepest gratitude to Professor Xue-Mei Liu, especially for her constant encouragement and guidance. Professor Liu has walked me through all the stages of the writing of this thesis. Secondly, I also would like to thank others for their support in data collection. Due to a large number of medical examiners, a lot of the work was done with the help of everyone. Thirdly, my thanks go to Shou-ling Wu. It is because of Wu’s suggestions of data collection platform that I could complete this thesis. Moreover, everyone in the team has contributed to the completion of this thesis with their kind assistance and support.
Author contributions
(I) Conception and design: Li-Shuang Gu and Xue-Mei Liu; (II) administrative support: Shou-ling Wu; (III) provision of study materials or patients: Li-Shuang Gu and Xue-Mei Liu; (IV) collection and assembly of data: Li-Shuang Gu, Xue-Mei Liu, and Jing-jing Bao; (V) data analysis and interpretation: Li-Shuang Gu and Xue-Mei Liu; (VI) manuscript writing: All authors; and (VII) final approval of manuscript: All authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.