
Abstract
Objectives
Analysis of patient injuries offers possibilities for improving quality in patient care. The aim of this study was to identify errors and adverse events leading to patient injuries in the treatment of internal carotid artery stenosis (ICAS).
Methods
A retrospective analysis was performed on data from Finnish patient injury claims and patient insurance center decisions in the treatment of ICAS, 2004–2017. Contributing factors to injury were identified and evaluated.
Results
During the 14-year study period, 42 patient injury claims involving ICAS treatment were closed in Finland. One claim involved carotid artery stenting, and the other operations were carotid artery endarterectomies. Nine of the claims were compensated (seven for operations and two for evaluations). Fully trained vascular surgeons had carried out all the operations and evaluations. Stroke was the most common complaint in the claims (n = 12). Six of the compensated patients were symptomatic prior to the interventions. Injuries were related to errors in decision-making and patient selection in two cases. Four patients received compensation for nerve injury and three for stroke. No deaths were compensated as patient injuries. Most negative claim decisions were related to the injury having been unavoidable.
Conclusion
Compensated patient injuries involving the treatment of ICAS are rare but often serious and mostly involve open surgery. Patient injury claims provide a valuable source of information for recognizing errors in care and offer possibilities to improve patient safety.
Keywords
Introduction
Stroke causes almost a million deaths annually in Europe. Stroke cost the healthcare systems of the EU €20 billion in 2015, so successful prevention of stroke could have vast clinical, social, and financial benefits. 1 Carotid artery stenosis causes about 10–15% of ischemic strokes. 2
The treatment goal with patients who have carotid artery disease is to decrease the risk of stroke. Internal carotid artery stenosis (ICAS) can be treated by carotid endarterectomy (CEA) or stenting (CAS). The evidence base for CEA among appropriate patients is strong. In selected cases, ICAS may be treated endovascularly with CAS. 3
Interventional treatment of ICAS carries significant and well-known risks. The authors of one meta-analysis concluded that CEA is associated with a risk of stroke or death in up to 5% of symptomatic and 3% of asymptomatic patients. 4 In more recent studies, the proportion of patients who experienced significant complications was lower, but compared with CEA, CAS has been associated with a slightly higher risk of periprocedural stroke or death.5–8 Both procedures are, however, equally effective in preventing stroke in the long-term.7,9,10 CEA is also associated with other complications including infection, cranial nerve injury, myocardial infarction, and postoperative hemorrhage, which are less common with CAS. Possible complications in CAS are puncture site hematoma, pseudoaneurysm, and thrombosis of the punctured artery.3,11
In Finland, both the national and European guidelines regarding treatment of ICAS are followed.3,12 Good cooperation among the neurologist, vascular surgeon, and interventional radiologist is vital when planning interventions, 3 and medical therapy is a crucial part of the treatment. 3 The decision to proceed to carotid intervention is based on symptoms and the degree of carotid stenosis,3,12 and the choice between the two procedures should be based on minimizing periprocedural risks. 11
Treatment can lead not only to well-known complications but also to patient harm in the form of patient injuries. Prevention of patient injuries should be a high priority in all healthcare. Patient injury claim data and insurance records can provide detailed information on patient injuries, 13 and analysis of these data can reveal information about rare events and procedural errors that often are not easily detectable in clinical trials. 14 Although the risks involved in treatment of ICAS have been thoroughly investigated, only a small number of published studies have assessed patient injuries in vascular interventions, especially in treatment of ICAS.15–18
Aims
Our aim was to explore the sources of errors and adverse events leading to patient injury claims involving CEA and CAS in Finland from 2004 to 2017.
Methods
Material
All patient injury claims closed during 2004–2017 and involving vascular surgery were searched from the Finnish Patient Insurance Center’s (PIC) claim records. Cases involving treatment of ICAS were identified by using International Classification of Diseases (10th revision) codes for carotid artery stenosis and/or codes for carotid artery procedures in the Nordic Classification of Surgical Procedures. The search was then widened to include all specialties not limited to vascular surgery to ensure identification of all claims regarding treatment of ICAS.
Background information concerning annual numbers of CEA and CAS performed in Finland was collected from the database of the Finnish Institute of Health and Welfare. 19
Patient insurance in Finland
Finland’s healthcare system is founded on government-subsidized municipal social welfare and healthcare services. PIC handles all patient injury claims in Finland in the public and private sectors and pays compensation accordingly if the claim is upheld. All official healthcare providers in Finland are mandated to have patient insurance according to the Patient Injuries Act (Potilasvahinkolaki 585/1986). The insurance covers any personal injury caused to patients in the course of medical care. Only cases that fulfill criteria described in the Patient Injuries Act can be compensated by the PIC. 20
Patients in Finland can use the assistance of the hospital ombudsman to file a claim with the PIC for suspected patient injury. The claim includes the patient’s written petition and all of the medical records of the treatment facility involved in the suspected injury. All claims are evaluated by an impartial medical professional and by the insurance board in the PIC. The PIC processes all Finnish patient injury claims. No other instances such as courts are involved in the process.
The seven compensation criteria or types of injury are classified as treatment-, infection-, accident-, or equipment-related injuries, injury arising from damage to treatment premises or the equipment used for the treatment, injury arising from an incorrect supply of pharmaceuticals, and unreasonable injury. A treatment injury is the most typical, and compensation criteria involving these injuries include that the injury could have been avoided had an experienced medical professional acted differently. Unreasonable injury can be compensated even if no fault is found in treatment but the injury is considered materially disproportionate with the initial situation. 20
Methods
Medical records, expert assessments, and indemnity decisions were analyzed in all compensated cases. Age, sex, diagnosis, and major comorbidities were recorded, as was information about healthcare providers and institutions.
In non-compensated cases, only a summary of the case was analyzed. This summary included diagnosis number, operation code, patient age, reason for complaint, and the claim decision.
Statistical analysis
Study data are given as categorical variables, frequencies, and percentages. Because there was no hypothesis, no statistical testing was performed.
Ethical considerations
The study protocol and data search received approval from both the PIC and the University of Turku. Because PIC is obliged by law to provide research data, no separate patient consent was required. All information regarding patient identity was excluded. Because this was a retrospective analysis of insurance charts, no separate approval from the ethics committee was required.
Results
During our 14-year study period, 42 patient injury claims involving treatment of ICAS were closed. One (2%) of the claims involved CAS. In other cases, if a patient was operated, CEA was performed. Among the claims, 21% (n = 9) were compensated. These claims made up 7% of the 136 compensated patient injuries related to vascular surgery during the study period. Not all compensated cases involved operative care but, if an operation was performed (n = 7), it was CEA.
In 2017, a total of 787 CEA and 59 CAS were performed in Finland.
19
Annual procedure numbers for CEA and CAS are presented in Figure 1. Annually 0.0–0.5% of all carotid artery procedures led to a compensated patient injury. Annual numbers of carotid endarterectomy (CEA) (black bar) and carotid artery stenting (CAS) (gray bar) in Finland according to the National Institute of Healthcare and Welfare statistics.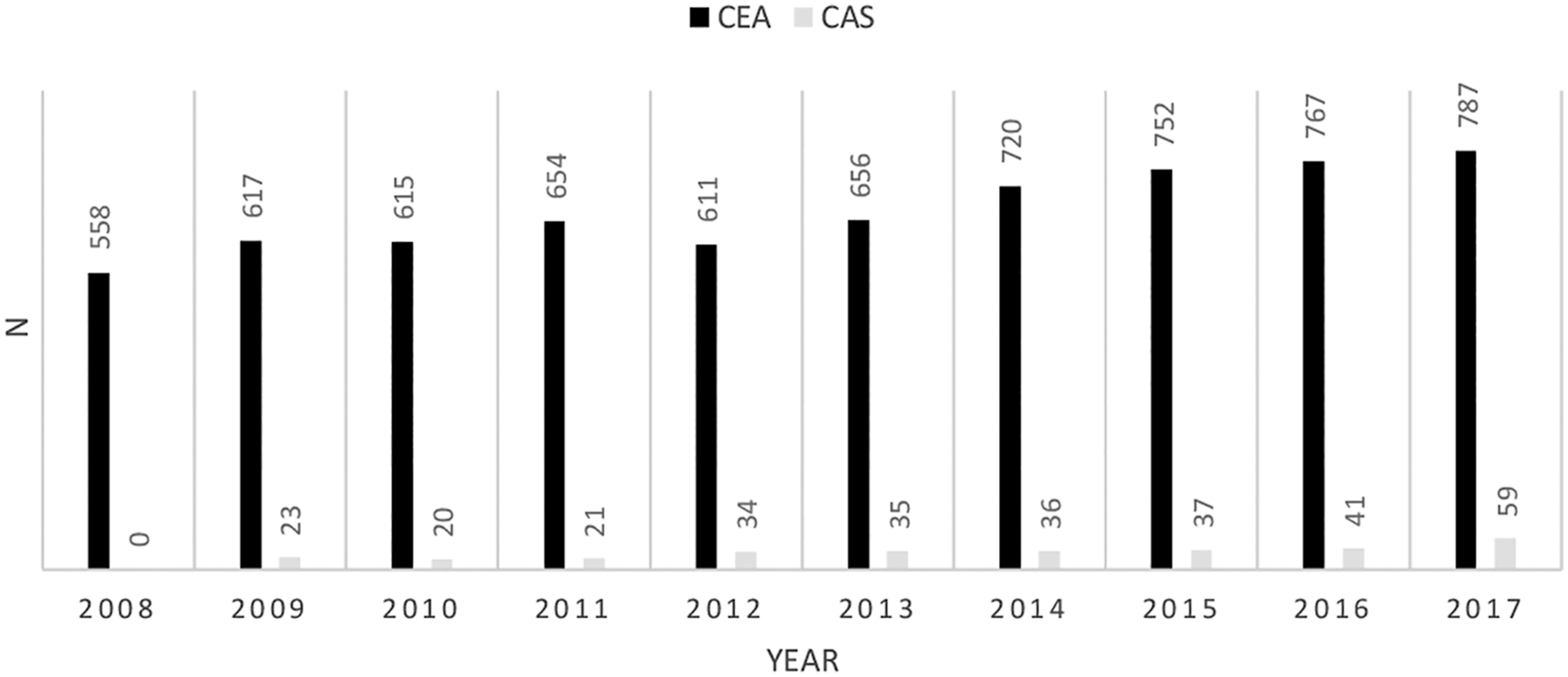
Preoperative symptoms, their timing, stenosis percentage, and operation type in nine compensated patient injury cases involving treatment of internal carotid artery stenosis in Finland, 2004–2017.
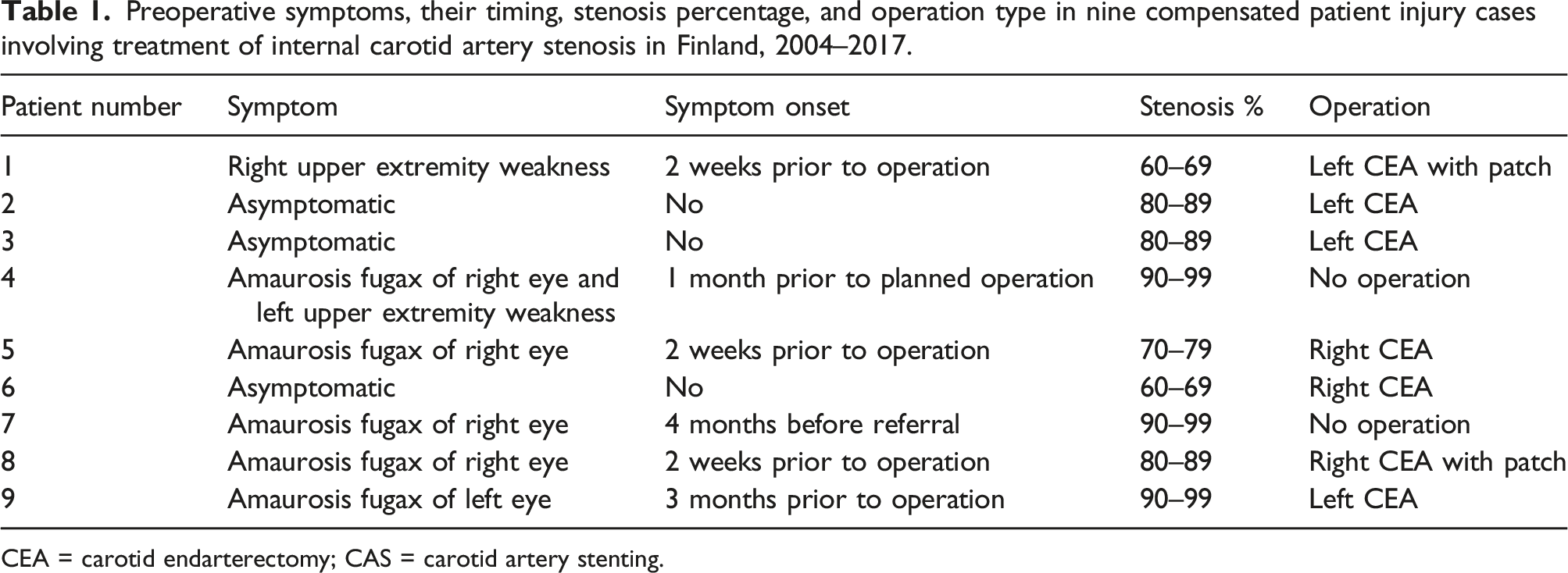
CEA = carotid endarterectomy; CAS = carotid artery stenting.
Of the compensated patients, seven (78%) were treated in a tertiary care hospital and two (22%) in a secondary care hospital. All operations involving the seven compensated patients were carried out by a fully trained vascular surgeon. In addition, the two patients who were not operated on had been evaluated by a vascular surgeon.
Claim incidents and their consequences
Reasons for complaints for 42 patients treated for carotid artery stenosis and number of compensated cases (for five patients, two complaints were identified).
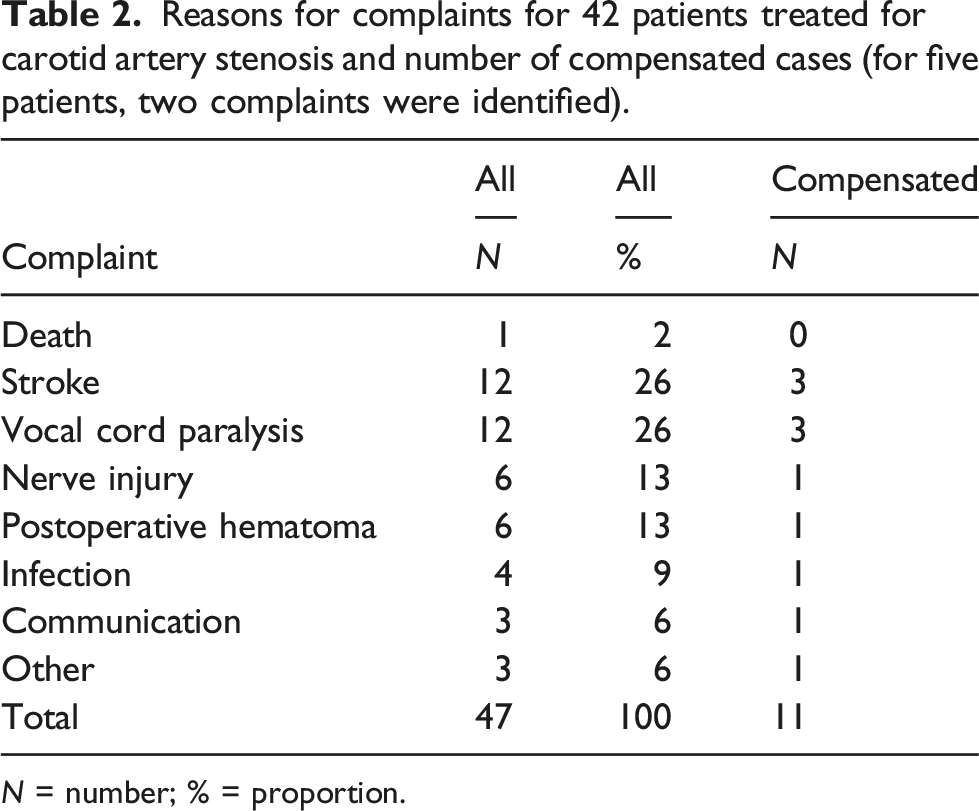
N = number; % = proportion.
Incident types and consequences in nine compensated patient injury cases involving treatment of CEA and CAS in Finland, 2004–2017.
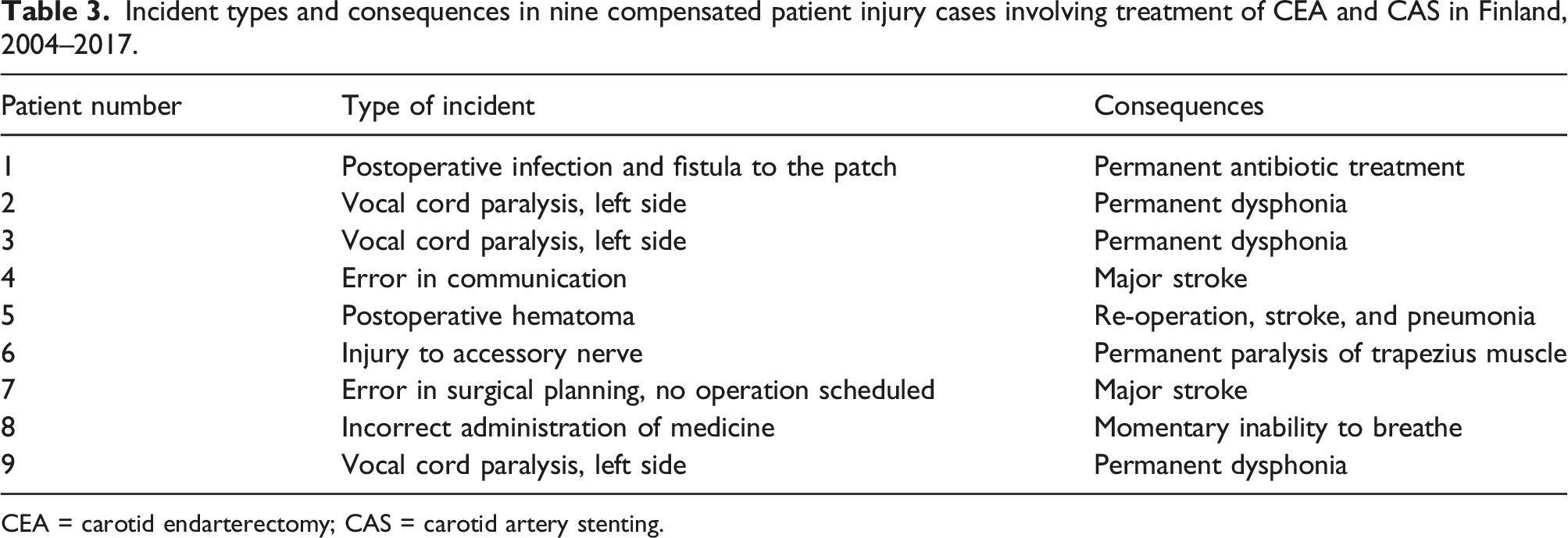
CEA = carotid endarterectomy; CAS = carotid artery stenting.
Death
No deaths were compensated as patient injuries. Compensation was sought for the death of one (2%) patient, who had died because of problems during the CAS operation. A cerebral emboli protection filter had gotten stuck during the operation and had to be surgically removed, and the patient eventually succumbed to postoperative complications. It was deemed that CAS always carries risks of such filter removal problems, and no fault in treatment was found.
Stroke
The most common reason for filing a complaint was stroke (n = 12). Three (25%) of these patients received compensation in connection to patient injury. Stroke was not compensated in any of the other nine (75%) cases because no fault in the treatment was found, and stroke was deemed to be a known possible consequence after high-risk surgery.
Of the three patients who were compensated for stroke, one (patient 4) had already been scheduled for CEA and was waiting for the operation at another hospital. The operating hospital ordered his only blood-thinning medication (aspirin) to be ceased 7 days preoperatively. The patient suffered a stroke on the way to the operation. Later, it was discovered that the operating hospital had provided outdated instructions, and the medication should have continued. For unknown reasons, old information had been sent to the patient’s hospital. Because of the stroke, the patient was left with major permanent disabilities.
For patient 5, the stroke occurred after postoperative hematoma evacuation. The patient had to wait for more than 24 h before the decision to re-operate was made and the hematoma was evacuated. It was found that the operation to evacuate hematoma should have taken place immediately after discovery of the hematoma. This patient also developed postoperative pneumonia requiring intensive care unit admission, but eventually, he mostly recovered from the stroke.
Patient 7 had symptomatic carotid stenosis. The patient also had schizophrenia and after first refusing surgery, ultimately consented to it. The evaluating vascular surgeon decided to wait to see if new symptoms emerged. After the patient had experienced no symptoms for 6 months, the stenosis was considered asymptomatic, and no operation was performed. The patient experienced a major stoke a few months later and required permanent care in a nursing home.
Nerve injury
Of 18 complaints associated with nerve injury, 12 (67%) involved vocal cord paralysis and 6 (33%) other nerve injury. Compensation was paid for a permanent injury to the accessory nerve to one (6%) patient and for permanent vocal cord paralysis to three (17%) patients.
In 11 (61%) non-compensated patients, the vocal cord dysfunction was only mild or reversible, and no compensation was granted. In some patients, the time that had passed since the operation was deemed too short, and the patient was advised to file a new claim if the symptoms persisted.
Hematoma
Six patients filed a claim because of postoperative hematoma. One (17%) patient (patient 5) received compensation for it. The reason for compensation was that hematoma evacuation was delayed for more than 24 h and led to serious consequences. This patient was also compensated for stroke.
Re-operation because of hematoma in the other five (83%) patients was considered non-compensable because it was performed in a timely way. Hematoma was considered an acceptable complication after CEA.
Infection
Four complaints involved postoperative infection. One (25%) patient developed a wound infection that led to infection of the prosthetic patch and fistula development. The fistula healed eventually with antibiotics, but lifelong antibiotics were deemed necessary, so the infection injury was compensated. In the other cases (75%), no compensation was paid because the consequences of infection were considered minor.
Communication
For three patients, the claims involved effects from problems in communication either between the patient and doctor or between treatment facilities. Only for patient 4 (33%) were the communication problems considered to have led to patient injury, which was the faulty communication between treatment facilities. Patient 4 also received compensation for stroke. In the other two patients (67%), communication was evaluated as having been sufficient.
Other
Three patients had other reasons for seeking compensation. In one (33%) patient (patient 8), incorrect administration of muscle relaxant (rocuronium bromide) before anesthetic left the patient awake and briefly unable to breathe. This error in anesthesia caused the patient significant stress and prolonged anxiety but resulted in no long-term consequences. This case was compensated as patient injury. The other two patients (67%) did not receive compensation. They had filed claims involving postoperative neck pain and re-stenosis after CEA.
Discussion
Patient injuries involving CEA and CAS are rare. Most patient injuries are related to well-known treatment complications such as stroke (33%), which can have major consequences. In this study, no deaths were compensated as patient injuries.
During our study period, 21% of the claims fulfilled the PIC’s compensation criteria. A total of 38% of claims in Sweden and 31% in the United Kingdom involving treatment of ICAS led to compensation. In Sweden, 0.4% of procedures led to a claim.17,18 PIC’s compensation criteria exclude injuries with only minor consequences, such as temporary dysphonia, which might explain the smaller percentage of compensated cases in Finland.
The Finnish patient insurance system is not designed to determine a guilty party. Documentation of experienced patient harm is encouraged in the patient files and it can ease the evaluation of patient injury claims. Patients receive compensation for the extra costs and losses incurred because of patient injury, so the compensation sums are small and do not attract claims being filed for monetary benefit only. Compensation sums paid by PIC are confidential and therefore cannot be published. In the United States, compensation sums paid for CEA-related injuries averaged more than US$1.5 million and can have a major role in injury claims. 15
Carotid endarterectomy carries significant risks of stroke, as high as 5%. 4 In previous Finnish studies, 3.6% of symptomatic and 0.3% of asymptomatic patients either died or suffered a stroke after CEA. 21 Only a small portion of these postoperative strokes led to a patient injury claim, and even fewer to compensation. It should be kept in mind that not all complications are automatically patient injuries and that defined criteria exist for their evaluation in Finland. Stroke is compensated by PIC only if the treatment did not meet the expected standard and something could have been done differently. Because of the seriousness of the underlying disease, risk of stroke can be considered acceptable and therefore non-compensable. Most non-compensated claims were declined because the injury would not have been avoided through different actions.
All operations leading to compensated patient injury were performed by a fully trained vascular surgeon, so lack of expertise does not explain the injuries. High operator and hospital volume have been associated with a decreased risk of death and stroke after carotid revascularization. 22 According to guidelines, all operating units should be aware of their complication numbers, and operations should be performed in units with low complication rates.3,12 Hospital size had little effect on patient injuries, as most injuries occurred in university hospitals. One stroke occurred during transport to a university hospital for an operation. Although centralization has advantages, long distances carry their own risks.
Correct patient selection and decision-making are key to good results in the treatment of ICAS. Informed consent requires the healthcare provider to educate the patient about the risks, benefits, and alternatives of a given procedure or intervention, and the patient must be competent to make a voluntary decision about whether to undergo the procedure or intervention. Risks and benefits in treatment of ICAS must be weighed individually, and the patient must be informed preoperatively about the risks and accept them.23,24 As in our material, in the United States, it also has been concluded that inadequate informed consent has a major role in litigation claims. 15 In our data, the case of a patient with schizophrenia who declined treatment is controversial. Despite a clear indication for carotid endarterectomy, the patient had first declined treatment, and even later communication could have been convoluted.
Carotid artery stenting can be considered for treatment of ICAS if surgery carries an excessive risk or is contraindicated, if the location of the stenosis is inaccessible to surgical procedures, or the neck is scarred or damaged by radiation therapy. In a previous Finnish study, the primary success rate with CAS was 98%, and stroke developed in five (3.7%) patients after CAS. Other reported complications were myocardial infarction, brain hemorrhage, inguinal pseudoaneurysm, and femoral artery stenosis. No deaths were reported. 25
In the current study, patients filed claims for patient injury only very rarely after CAS. Only one of the claims involved CAS, and it involved the death of the patient. No other complications after CAS were reported in the patient injury claims. This low rate might be explained by the relatively small number of CAS procedures performed. Annually, only 0–7% of ICAS procedures were CAS. It also is possible that patients do not file claims after endovascular procedures as readily as after open surgery, even when experiencing an injury. Endovascular procedures are less invasive and thus might be associated with a higher tolerance for complications. In addition, various technical developments have improved the safety profile of CAS during the last decade. These include the use of embolic protective devices and development of stent construction, as well as a transradial instead of a transfemoral approach in the case of aortoiliac problems or difficult aortic arch anatomy. 26
Much discussion has focused on the correct timing of carotid operations. None of the compensated patient injuries in this study involved the timing of the original intervention. The symptomatic patients had experienced their first symptoms from 2 weeks to 3 months before the operation. Delays can occur if a patient seeks help late, referral to the vascular surgeon is delayed, and or the operation is delayed. There is evidence that CEA benefits symptomatic patients most if performed within 14 days of the index event. 3 Only one of the compensated symptomatic patients was operated within that time frame. Information about timing of the operation was not available for the non-compensated patients. It is possible that in the future, correct timing of the operation will be a compensation criterion for patient injury.
The hypoglossal and vagal nerves and the lower branch of the facial nerve are in anatomical proximity to the internal carotid artery. Nerve injuries can cause serious dysfunction in speaking and swallowing. 12 Injuries to these nerves have been reported in 5.2% of patients after CEA, 8 but most cranial nerve injuries after CEA are temporary. In our study, only 22% of the reported nerve injuries in claims were considered permanent, but 44% of the compensated injuries involved a cranial nerve. In Sweden, the most common reason for compensation after CEA was cranial nerve injury (71.4%), and in the United States, 25.0% of cases of CEA litigation related to cranial nerve injury.15,17 The numbers are small, however. Cranial nerve injuries can be avoided with good anatomical knowledge, with careful use of instruments, and by avoiding forceful retraction. In CAS, cranial nerve injuries are rare.
Neck hematoma after CEA occurs in 2.4–5.5% of patients, and requires immediate intervention.3,27,28 Delaying treatment can have life-threatening consequences because of compromised airway. In our material, the delay in hematoma evacuation was a clear indication for compensation. Delays in timely recognition of complications have led to litigation claims in the United States, as well. 15
Infection of a vascular patch is a rare phenomenon, occurring in 0.8–1.4% of CEAs. It can lead to serious complications, including pseudoaneurysm formation and patch rupture. 3 In our patients, no serious consequences were reported. Because lifelong antibiotic treatment was deemed necessary, it is possible that new complications may emerge. The injured patient had received no antibiotic prophylaxis prior to operation. Even though infection following CEA occur seldom it is worth considering antibiotic prophylaxis before CEA, especially if a vascular patch is used.
Patient injury data should be used to improve patient safety in carotid artery procedures. Compensated patient injuries should be processed and discussed in all operative units in order to avoid patient injuries in the future. Patient injuries give valuable information that can be used to educate the next generation of vascular surgeons. Not all complications are preventable, but prevention of patient injuries should be a high priority. 29 Information learned from such analyses of patient injuries serves as a tool in healthcare to improve patient care.
Study strengths and limitations
Our data came directly from the PIC insurance chart registry, which is nationwide and highly representative. The PIC registry does not capture all complications in vascular surgery in Finland but only cases for which the patient filed a claim for a suspected patient injury. Unfortunately, no national registry for vascular surgery procedures exists currently in Finland. A uniform registry could give more information on performed carotid artery procedures and would be valuable in identifying complications which might fulfill patient injury criteria even though no claim was filed.
Closed claim analysis has limitations. Inadequate knowledge about the insurance system might influence claim frequency. Not all patients seek compensation from patient insurance even after experiencing an injury. Carotid artery stenosis patients are often elderly, and this might influence the rate of claims submitted.
Conclusion
Patient injuries in treatment of ICAS were rare. Treatment of ICAS can lead to serious consequences, and patients are expected to tolerate some complications. Common complications such as stroke were compensated as patient injuries only if the expected standard of care was not met. Correct patient selection, communication, and comprehensive informed patient consent are vital in the process. Patient injury analysis can be used as a valuable tool in improving quality of care.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.